Radial Club Hand Correction of Deformity Centralization n

Radial Club Hand

Correction of Deformity Centralization n Radialization n Distraction n Distal Ulnar Osteotomy n Problems: 1. High recurrence rate 2. Growth arrest distal ulna
 n Modification of Buck Gramko method Buck Gramko: called")
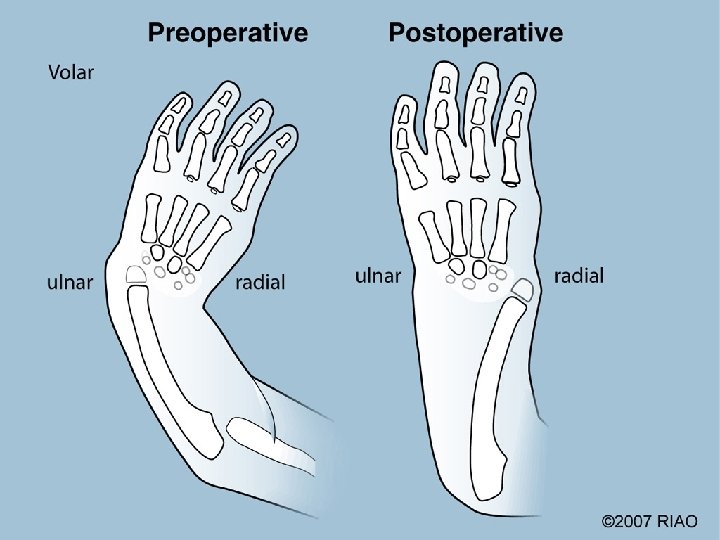
New Method: Ulnarization (Paley 1998) n Modification of Buck Gramko method Buck Gramko: called this radialization since makes ulna into a radius n Paley: called this ulnarization since moves carpus to the ulnar side of the ulnar head n

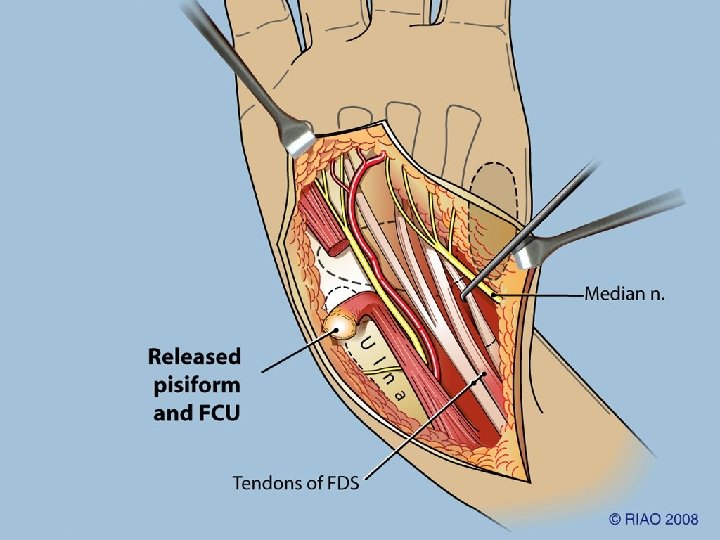
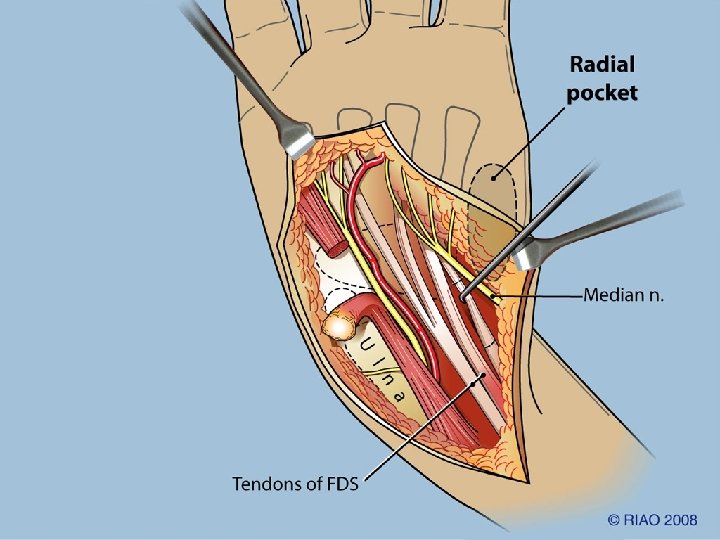
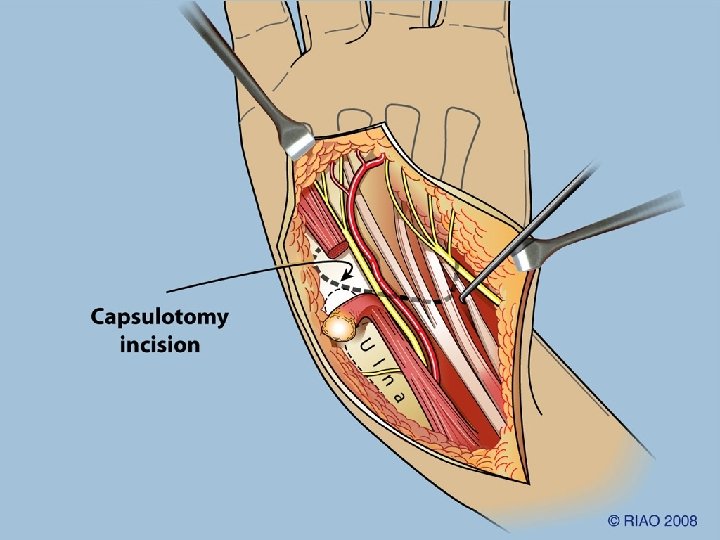
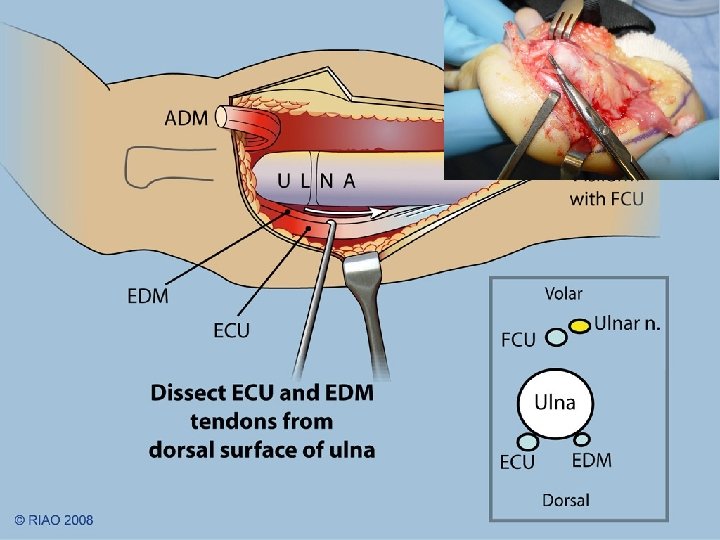
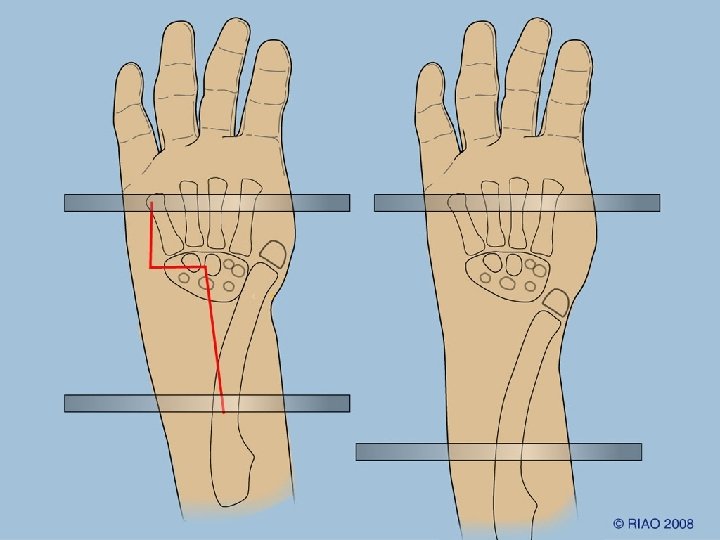
Ulnarization of the Carpus with Tendon Transfer of FCU

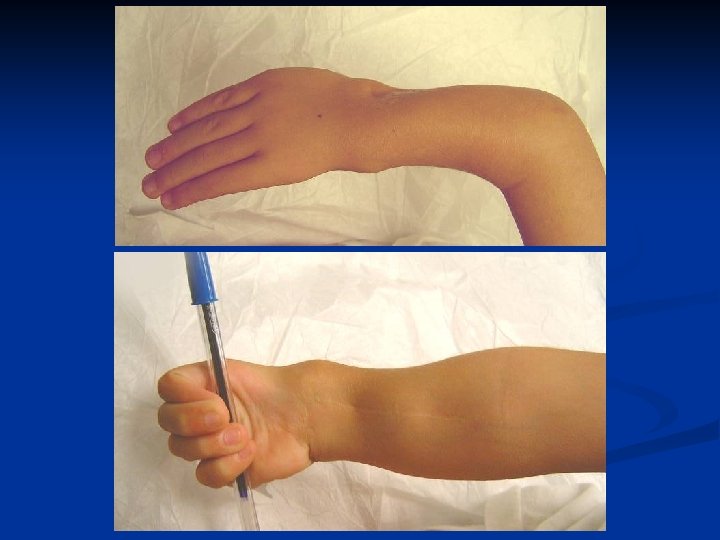
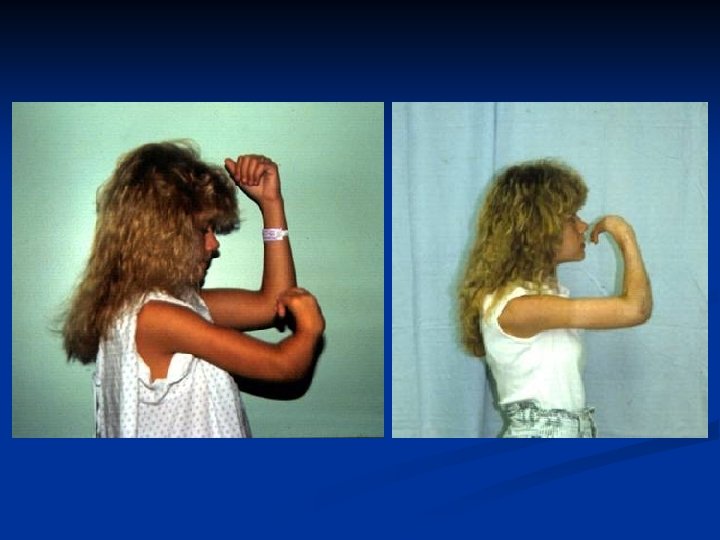
RCH: Poor Grip Strength Due to lack of fulcrum n Forearm shortening affects muscle length curve (Blick’s) n Excessive palmar flexion pull: dorsi flexion of hand increases grip strength n

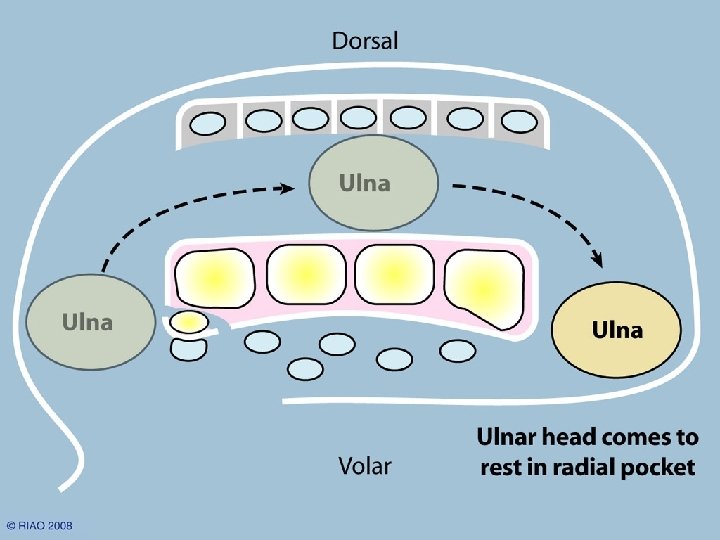
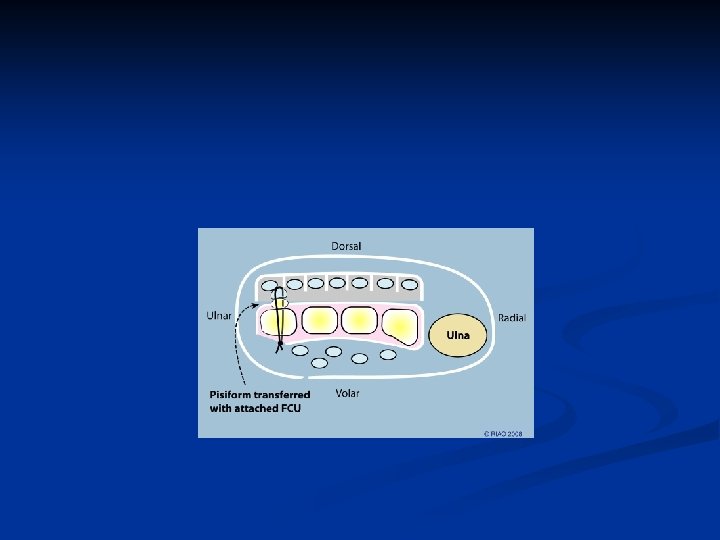
Ulnarization n Converts head of ulna into a fulcrum due to radial pull of muscles fulcrum Muscle pull

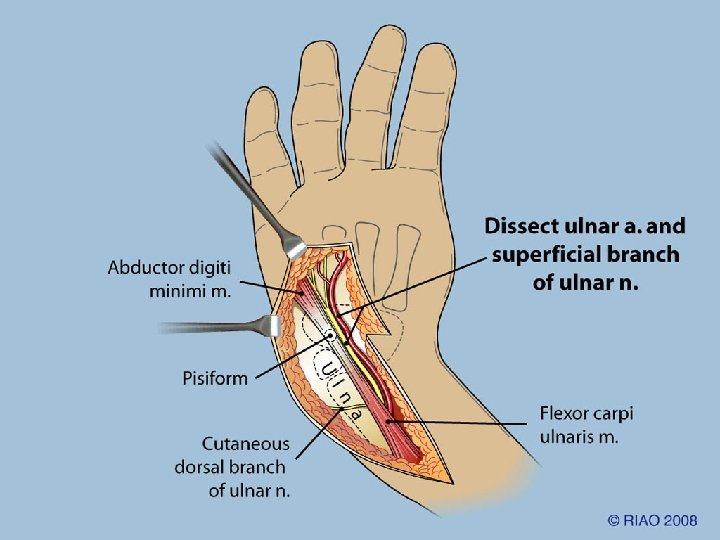
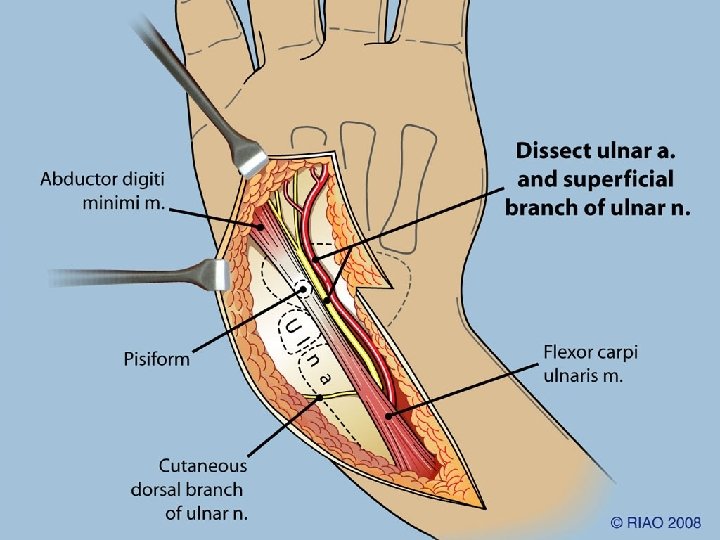
Flexor Carpi Ulnaris Transfer • FCU is the major deforming flexor force • Transfer to dorsum converts it to a correction force • This helps improve finger flexion ROM and strength
 n Improves grip strength n")
Lengthening Improves muscle tension (Blick’s curve) n Improves grip strength n
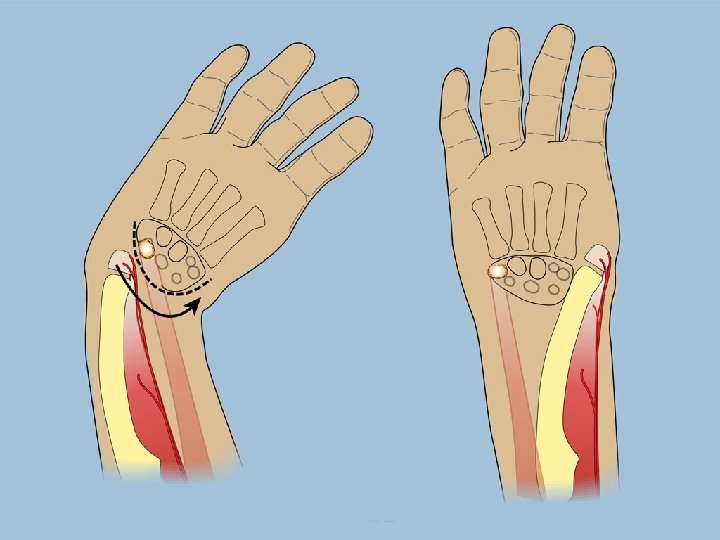
 Name describes direction of carpal translocation")
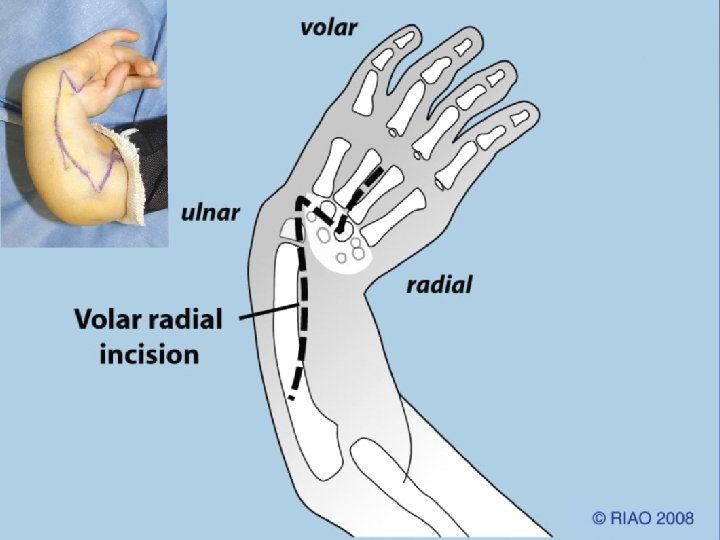
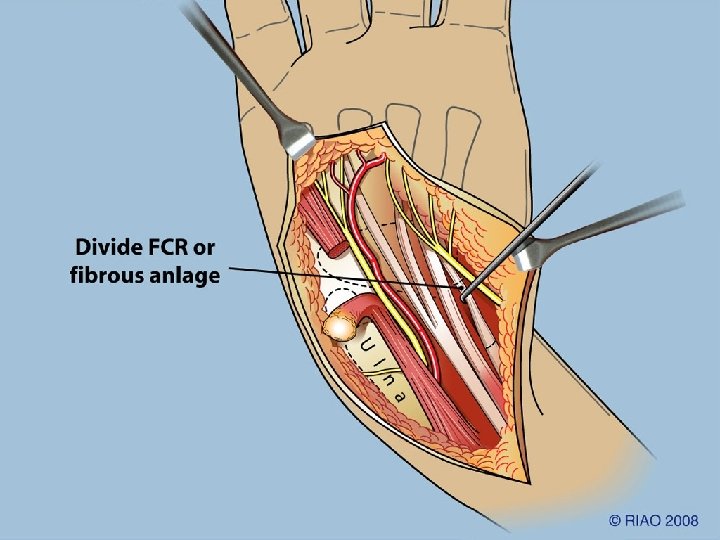
Ulnarization vs Radialization n n n Paley (1998) Name describes direction of carpal translocation Volar approach Visualize all the N-V structures Transfer FCU tendon Extensile for elbow contracture release n n n Buck-Gramko (1979) Name describes change of ulna to a radius Dorsal approach Cannot visualize N-V structures Transfer FCR* *FCR usually absent








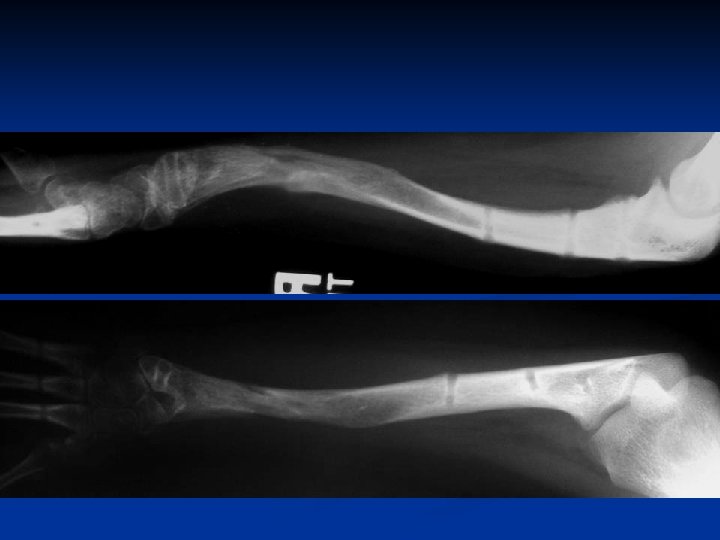
8 year followup





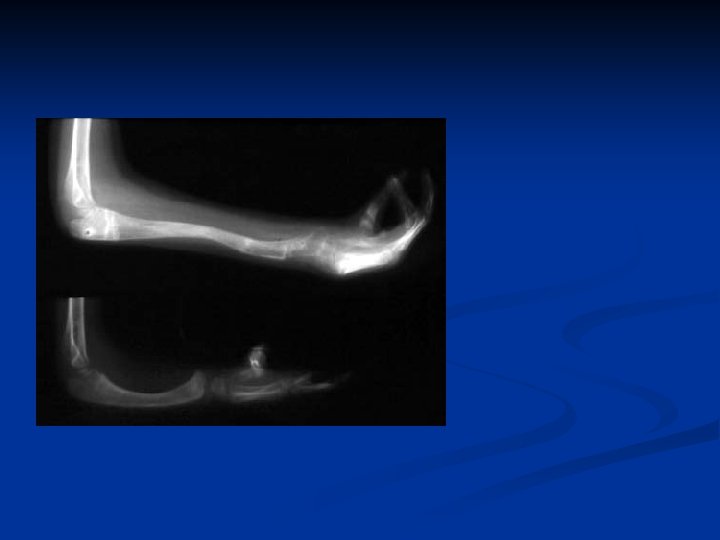
7 yr. followup radiographs

Ulnarization: Results 15 patients; 21 hands n Followup 1 -7 years n Recurrence: 0 n Growth arrest: 0 n

Ulnarization: Complications n 2 skin necrosis treated by debridement and secondary closure
")
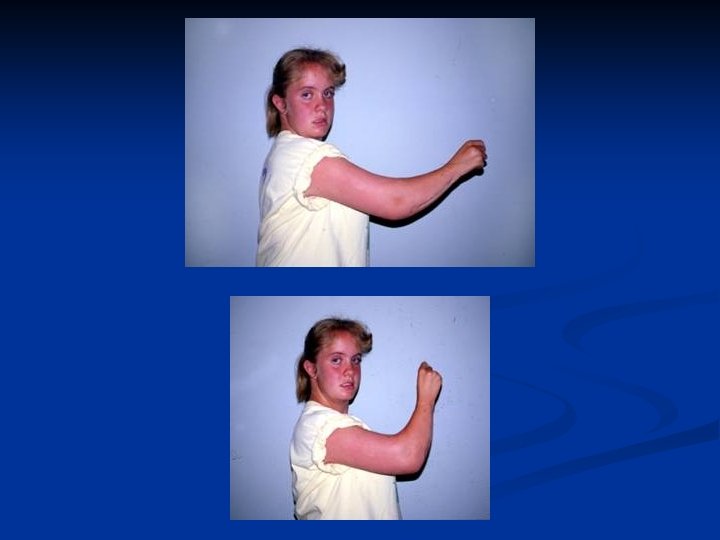
Wrist Dorsiflexion PASSIVE preop -15° postop +36° ACTIVE postop 9°(10 -20°)
 Postop: 102 mm (58 -188 mm) No Growth")
Preop: 79 mm (40 -175 mm) Postop: 102 mm (58 -188 mm) No Growth Inhibition

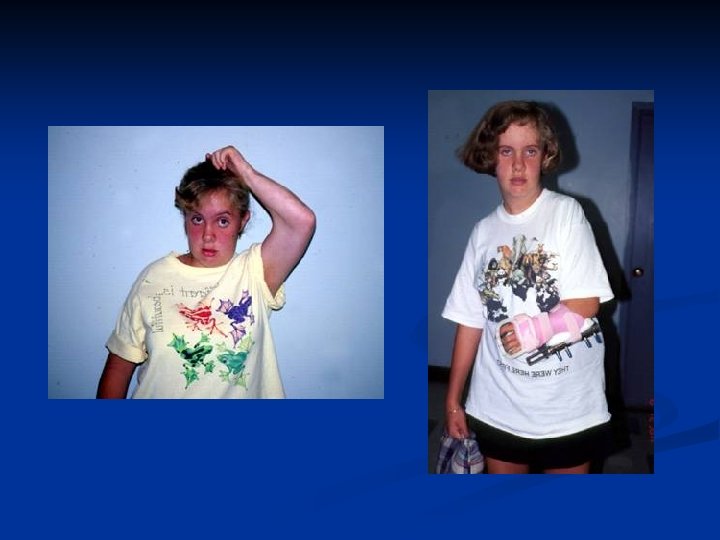
Conclusion • safe • no recurrences • no growth arrest • low complication rate • improves grip strength • active dorsiflexion • improves activities of daily living • improves cosmesis

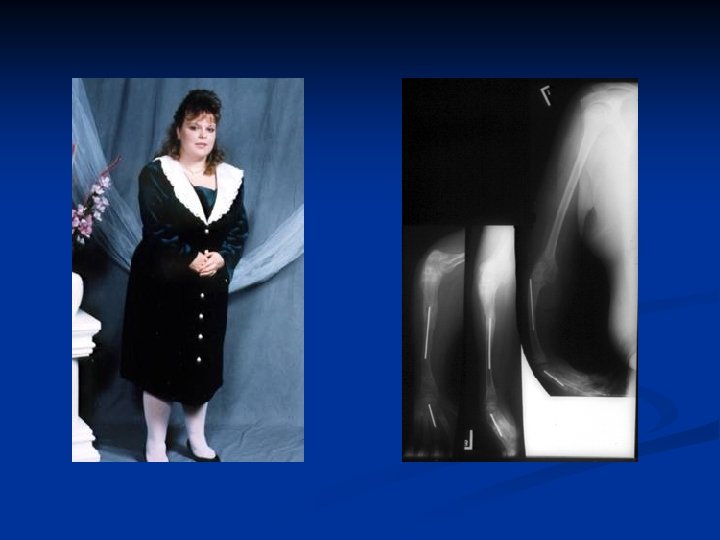
Lengthening of the Forearm for Radial Clubhand

Strategy Dependent on age at presentation Age 6 10 years Two lengthenings

• Before age 10 years st 1 lengthening 4 -6 cm • After age 10 years nd 2 lengthening 6 -8 cm





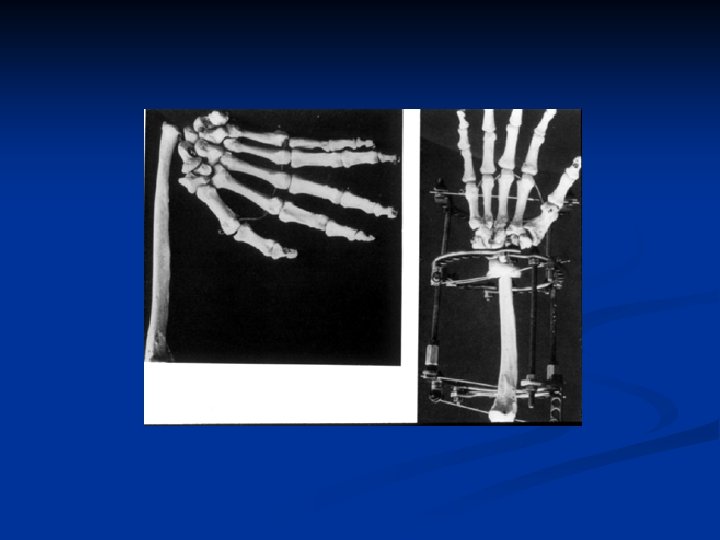
before after normal Before vs After 1 st Lengthening vs Normal side




preop st lengthening 1 st 1 lengthening: 7 cm 8 cm 2 ndlengthening: lengthening 2 nd 10 cm Total length gain 18 cm

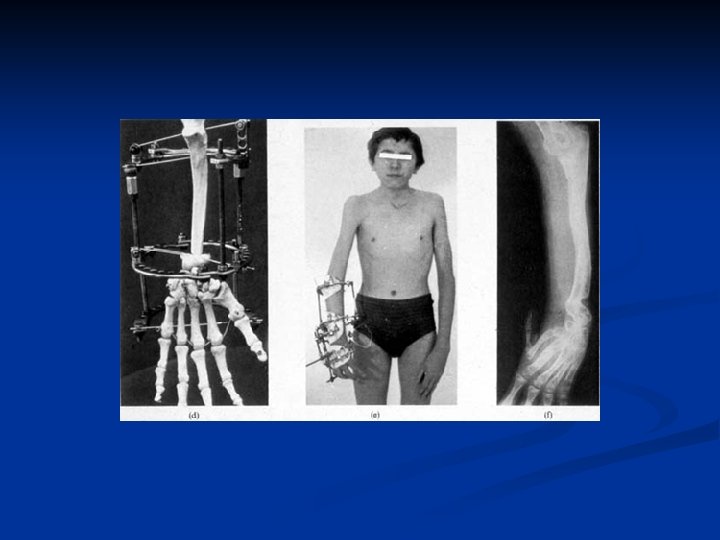
7 y. o. girl with rch and partial growth arrest 1 st Lengthening: 6 cm

before after



2 nd Lengthening


Strategy Dependent on age at presentation • Age 11 20+ years one lengthening 8 12 cm
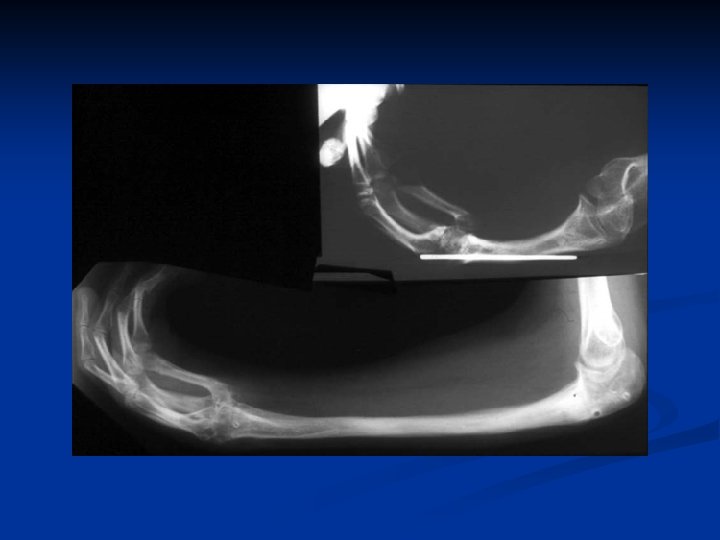



Distal Ulnar Osteotomy Reorient Original Ulno Carpal Psuedo Joint

16 y Radial clubhand 1 y centralization 2 y pollicization


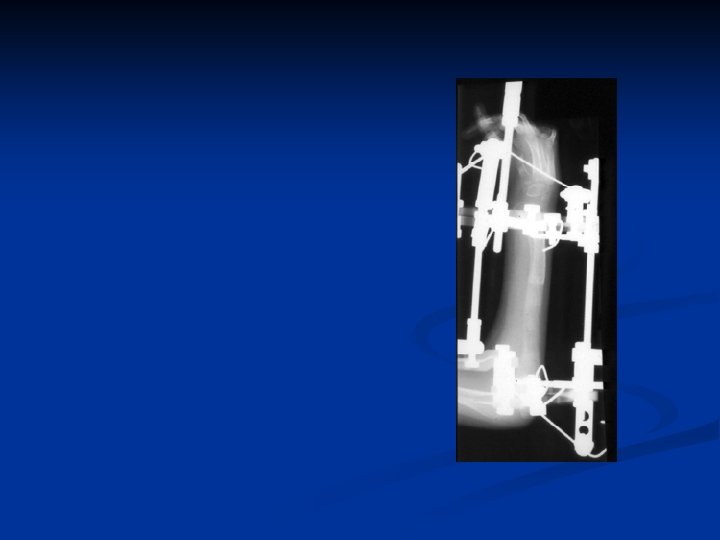
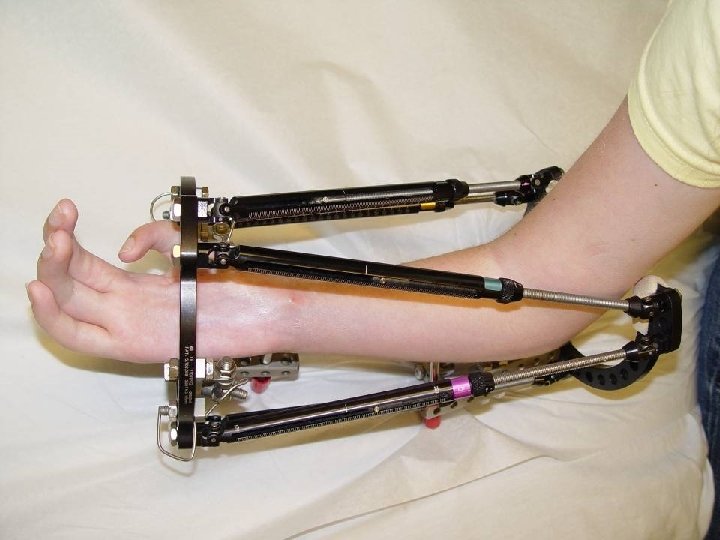
12 Feb 03 Osteotomy R ulna + application TSF Intraop Post-op


During distraction

4 months post op.







Materials • 24 forearms • 20 patients

Range of Motion Decreased Same Increased 0 1 4

Complications Refractures 3 Premature Consolidation 1 Reoperation for Complications 2

Grip Strength Improved Worsened 24/24 0/24

Follow-up Mean Range 10 years 1 13 years
 Range (cm) Mean (cm) 6 9 10 14 5 8 8")
Lengthening Age (yr) Range (cm) Mean (cm) 6 9 10 14 5 8 8 10 7 9

Lengthening Once 24 Twice Total 6 28

Range of Motion • Finger flexion: increased range and grip strength in all patients • Finger extension: decreased MCP extension in 2 patients (20°) • Elbow extension: transient contracture in all patients, return to preop levels in all • Elbow flexion: improved in 2 and unaffected in 7

Lengthening Amount • Mean, 7. 6 cm • Range, 5 11 cm

Strategy This study Age 0 5 years: correction hand/pollicization 6 Age 6 10 years: 1 st stage lengthening 12 Age 11 -16 years: 2 nd stage lengthening 6 Age 11 20 years: one lengthening 6

Additional Deformity Correction • Distal ulnar osteotomy for hand angular realignment • Mid ulnar osteotomy for correction of ulnar bow • Bilaterals: Supination of forearm at end of lengthening for perineal care

Conclusion • safe • low complication rate • improves grip strength • improves pollicization pinch • improves ADL • improves cosmesis • improves body image
- Slides: 99