RABIES Zoonotic viral infection causing acute e Encephalitis

RABIES • Zoonotic viral infection causing acute e Encephalitis in mammals. • Rabies virus member of Rhabdoviruses • Bullet shaped (-) RNA viruses • Lyssaviruses – Rabies – Mokola – Duvenhage – European bat lyssavirus (EBLV) – Australian bat lyssavirus (ABL)

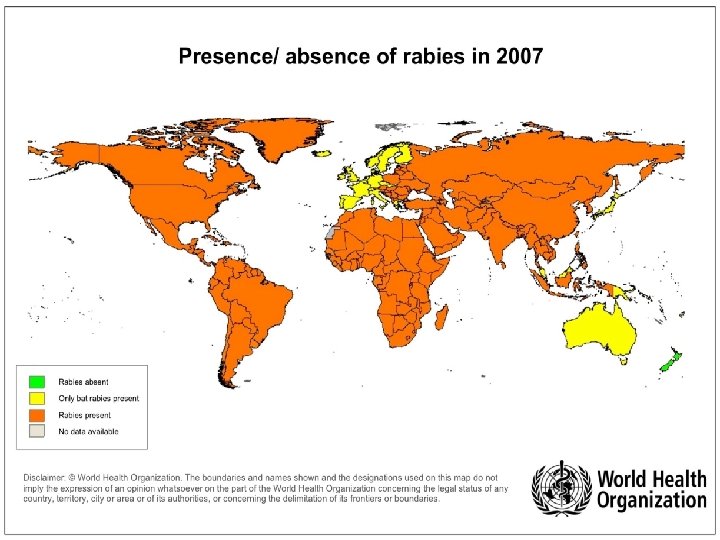
Epidemiology • Virus is maintained in enzootic reservoirs • Two patterns – Urban: pets – Sylvatic: Small number of wild mammals and bats • Almost 55, 000 deaths annually in mostly developing countries

Rabies transmission • Spread between mammals is by – Bites – Contact with mucous membranes – Inhalation of aerosols (bats) – Contact with broken skin or wounds – Ingestion of infected prey – Transplacental • Human infections acquired by – Bites – Salivary contamination of mucous membranes, broken skin, wounds – Aerosols – Rare: Corneal transplant graft, improperly inactivated vaccine, transplacental

Pathogenesis of rabies • Following virus entry the virus remains inactive for days to months • Host immune defences may eliminate the virus at this stage, especially if vaccinated • There is some replication in local tissues • Virus enters peripheral nerves and is transported to the central nervous • system (CNS) via retrograde flow in axons. Typically this occurs via sensory and motor nerves at the initial site of infection. • Once virus enters the nerves it is not accessible to the host immune defenses

• Incubation period to onset of clinical signs varies from a few days to several years, but is typically 1 to 3 months. • Dissemination of virus within the CNS is rapid, and causes the classic behavioural changes associated with rabies • Passive centrifugal spread of virus to peripheral nerves and to highly innervated peripheral tissue such as the salivary glands. • Potentially infectious to other in contact with saliva, blood, tissues

Clinical presentation • • • Nonspecific prodromal illness Clinical types – Furious rabies – Paralytic rabies • Mortality ~ 100%

• Furious rabies – Most common – aerophobia, hydrophobia, bizarre behaviour, disorientation and hyperactivity – signs of autonomic instability such as hypersalivation, hyperthermia and hyperventilation may occur – deteriorate over a few days, followed by death • Paralytic rabies – Uncommon – Progressive paralysis, beginning nearest to site of bite, progressing to quadraparesis and laryngeal paralysis – autonomic problems such as constipation, urinary retention, fever, sweating Deteriorate to death

Untreated mortality following rabid dog bite • Early estimates – Severe head wounds 100% – Severe facial bites: 60 -80% – Bites on hands: • Severe: 70% • Superficial: 2% – Bites on legs: 20%

Diagnosis of rabies • Saliva – Detection of rabies RNA by PCR and isolation of virus in cell culture. • Neck Biopsy – A section of skin 5 to 6 mm in diameter should be taken from the posterior region of the neck at the hairline. The biopsy specimen should contain a minimum of 10 hair follicles and be of sufficient depth to include the cutaneous nerves at the base of the follicle. – For PCR and immunofluorescent staining for viral antigen in frozen sections of the biopsy. • Serum and cerebral spinal fluid (CSF) – At least 0. 5 ml each of serum and CSF should be collected – If no vaccine or rabies immune serum has been given, the presence of antibody to rabies virus in the serum is diagnostic and tests of CSF are unnecessary. – Antibody to rabies virus in the CSF, regardless of the immunization history, suggests a rabies virus infection. – Laboratory tests for antibody include indirect immunofluorescence and virus

Prevention of rabies • Avoid exposure • Pre-exposure rabies vaccination - Three IM (IM or SC if HDCV is used) injections of 1 m. L of rabies vaccine at days 0, 7 and 28 • Post-exposure prophylaxis • Local measures – Immediate and thorough washing with soap and water, and apply a virucidal preparation such as povidone iodine solution – primary suture of a bite from a potentially rabid animal should be avoided • Human rabies immunoglobulin (HRIG) • – Give as early as possible, but no later than 7 days after first vaccine dose • – Infliltrate as much as possible around the wound, the rest given i. m. • Rabies vaccine – days 0, 3, 7, 14 and 28– 30 – modified if previously vaccinated
- Slides: 11