Qualitative Comparison of Barriers to Antiretroviral Medication Adherence

Qualitative Comparison of Barriers to Antiretroviral Medication Adherence Among Perinatally and Behaviorally HIVInfected Youth Idia B. Thurston 1, Laura M. Bogart 1, Errol L. Fields 1, Margie R. Skeer 2, Laurel A. Sticklor 1, Elizabeth F. Closson 2, Steven A. Safren 2, 3, & Matthew J. Mimiaga 2, 3 1 Children's Hospital Boston/Harvard Medical School, 2 The Fenway Institute, Fenway Health, 3 Harvard Medical School/Massachusetts General Hospital
 Medication Adherence in Youth • Recommendation for Adherence")
• Barriers to Antiretroviral (ARV) Medication Adherence in Youth • Recommendation for Adherence

HIV Infection in U. S. Youth • Over 25, 000 HIV-infected 13 -24 year-olds • ~77% are behaviorally-infected and 23% are infected via perinatal or other exposures • Advances in ARV treatment have resulted in extended life expectancy CDC, 2010, Palella et al. , 1998; USDHHS 2008

To achieve viral suppression, ideal adherence to ARV: 85 -95% Estimated adherence rate in HIV+ youth: 28 -69% Reisner et al. , 2009

Interventions for Youth • Improvement in youth adherence is needed • Counseling sessions promoting adherence skill-building are effective in HIV-infected adults • Few studies have used such strategies with HIV-infected youth Reisner et al. , 2009

Study Aims • Conduct formative qualitative research to explore barriers to ARV adherence in youth • Examine barriers that affect youth differentially based on mode of infection • Identify factors to adapt a behavioral intervention to improve youth adherence

METHODS: Participants • 28 adolescents and young adults • Recruited during outpatient clinic visits at a hospital and community health center in Boston • Eligibility criteria: o o o HIV-positive 13 -24 years old Prescribed/recommended ARVs in past 6 months

Qualitative Interviews • Participants completed 45 -90 min interviews • Semi-structured interviews covered: o o Experience taking ARV Facilitators and barriers to adherence Knowledge of ARV Psychosocial and behavioral adherence factors

Data Analysis

Data Analysis

Data Analysis

RESULTS: Socio-Demographics • 28 HIV-infected youth • Mean Age = 20 years (SD = 2. 7) o Age range 14 -24 years old • Education § Middle School (4%), High School (54%), and College (43%)

Gender

Race and Ethnicity

Sexual Identity

THEMES

Adherence Themes Across Perinatally and Behaviorally-Infected Youth

Adherence Themes Across Perinatally and Behaviorally-Infected Youth

APATHY ABOUT CONSEQUENCES OF NONADHERENCE When I was young I used to think if I missed two doses in a row I am just going to die…as you get older you realize the truth…you’re not going to like [get] sick or die the next day but at the same time you don’t want to let yourself think that cause then you’ll let yourself slack off. 19 -year-old Male
![IRREGULARITY OF DAILY SCHEDULE If I have more [school] work to do that night](http://slidetodoc.com/presentation_image_h2/4eb0e34a9451202fa3eef10e5634055e/image-21.jpg "IRREGULARITY OF DAILY SCHEDULE If I have more [school] work to do that night")
IRREGULARITY OF DAILY SCHEDULE If I have more [school] work to do that night I might be up until 1 or 2 instead of going to bed at like 10 or 11, which would mean that…if I don’t want to get the side effects…interfering with my homework, then I would have to take them later than I normally would. 20 -year-old Female

Adherence Themes: Perinatally-Infected Youth

Adherence Themes: Perinatally-Infected Youth

COMPLICATED DISCLOSURE DUE TO PARENTAL HIV My father didn’t want people knowing about my status, so it was better to just keep it hidden… we never really had any conversations about [HIV], not until recently, but for all the years growing up…we never talked about it. It was basically just take your medication and don’t talk about it. 24 -year-old Female
 It’s like “take it. ” And it’s")
REACTANCE (I. E. , OPPOSITION TO INSTRUCTIONS) It’s like “take it. ” And it’s like “Okaaay like shut up” you just take it because someone’s telling you to take [it]…I think that creates a factor in people and…when…they become independent they’re like “F*** this s*** ain’t no one gonna tell me when to take [it] so I am not going to take it. ” 21 -year-old Female

Adherence Themes: Behaviorally-Infected Youth

Adherence Themes: Behaviorally-Infected Youth

GREATER CONTROL OVER MEDICATION INITIATION I actually did refuse to get on meds until uh, February or March of this year. I wasn't ready to do it… I never stuck [to] it, and it was an adherence issue is why I got off them. 24 -year-old Transgender: F to M
![SELF-BLAME FOR HIV INFECTION I was kind [of] going through a rough part and](http://slidetodoc.com/presentation_image_h2/4eb0e34a9451202fa3eef10e5634055e/image-29.jpg "SELF-BLAME FOR HIV INFECTION I was kind [of] going through a rough part and")
SELF-BLAME FOR HIV INFECTION I was kind [of] going through a rough part and I was trying basically to get back at um—I don't know…if I was getting back or proving a point to myself but I um, went and had sex with a random person from a night club and I didn't take care of myself and I got infected. 24 -year-old Male

Conclusions • Adolescents have some adherence barriers that are similar to adult barriers • Barriers unique to adolescents also emerged • Certain themes were unique to perinatal versus behaviorally infected youth

Recommendations • Practice guidelines should focus on the impact of adolescent development and unique barriers on engagement of youth in care • Adherence interventions may need to tailor content and delivery based on source of HIV infection

Limitations • Small convenience sample of 28 youth • May not be generalizable to all youth with HIV

Next Steps: Intervention Development Positive STRATEGIES TO ENHANCE PROBLEM-SOLVING SKILLS

Acknowledgments • Sources of support: Harvard Center for AIDS Research P 30 AI 060354; Children’s Hospital Boston Division of Adolescent/Young Adult Medicine & MCH/HRSA LEAH T 71 MC 00009 • Research staff: Jess Ratner, BA, & Madeline Wachman, BA • Community Partners: Boston HAPPENS and Children’s Hospital AIDS Program

THANK YOU Idia B. Thurston Idia. thurston@childrens. harvard. edu

EXTRA SLIDES

References • Centers for Disease Control and Prevention. HIV Surveillance in Adolescents and Young Adults. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2010. • Palella FJ, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med 1998; 338: 853 -860. • Reisner SL, Mimiaga MJ, Skeer M, et al. A review of HIV antiretroviral adherence and intervention studies among HIV-infected youth. Top HIV Med 2009; 17: 14 -25. • U. S. Department of Health and Human Services Panel on Antiretroviral Guidelines for Adult and Adolescents. Guidelines for the use of antiretroviral agents in HIV-1 -infected adults and adolescents. Department of Health and Human Services. January 29, 2008; 1 -128. http: //www. aidsinfo. nih. gov/Content. Files/Adultand. Adolescent. GL. pdf.
 N (%) Behaviorally Infected: 12")
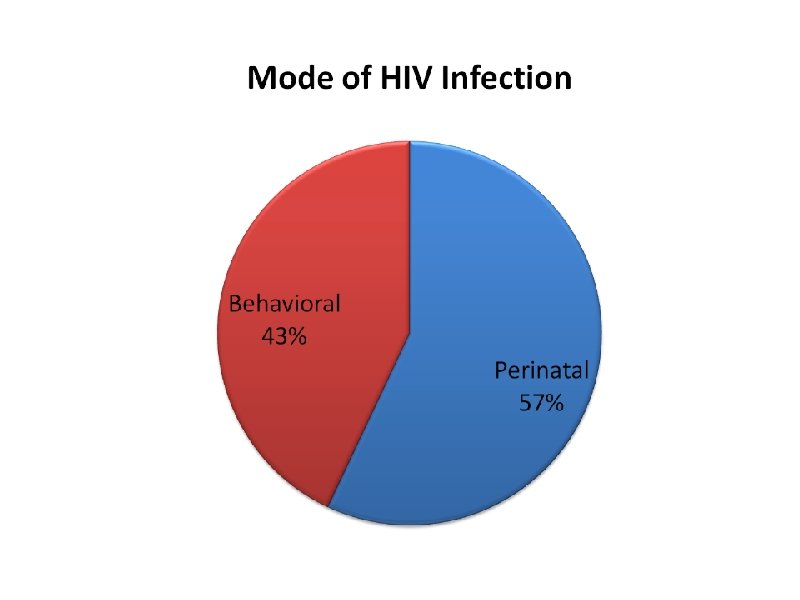
Demographics by Mode of Infection Perinatally Infected: 16 (57) N (%) Behaviorally Infected: 12 (43) N (%) Age Range: 17 -24 years Mean: 19 years (SD = 3) Range: 14 -24 years Mean: 23 years (SD = 2) Gender Male: 6 (37) Female: 10 (63) Transgender: 0 (0) Male: 10 (83) Female: 0 (0) Transgender: 2 (17) Race Black: 8 (50) White: 1 (6) Other*: 7 (44) Black: 3 (25) White: 5 (42) Other*: 4 (33) Ethnicity Latino: 2 (13) Latino: 3 (25) Sexual Identity Gay, Bi, Other: 2 (13) Straight: 14 (87) Gay, Bi, Other: 11 (92) Straight: 1 (8) Education Middle School: 1 (6) High School: 10 (63) College: 5 (31) Middle School: 0 (0) High School: 5 (42) College: 7 (58)
- Slides: 38