PYOGENIC LIVER ABSCESS Dr B Ramdas Rai Prof

PYOGENIC LIVER ABSCESS Dr. B. Ramdas Rai Prof. & Unit Chief YMCH

• Aetiology 1. Biliary sepsis: a. Empyema gallbladder. b. Cholangitis. c. After biliary tract surgery. d. Instrumentation. 2. Portal vein sepsis: a. Appendicitis. b. Diverticulitis

3. Distant infections: a. Pneumonia. b. Upper U. T. I. c. Endocarditis. 4. Super added infections: a. Amoebic liver abscess. b. Hydatid cyst. 5. Cryptogenic liver abscess—No identified primary infection. 6. Trauma becoming common cause.

Causative bacteria • E. coli—commonest • Klebsiella • Proteus • Pseudomonas • Clostridia

• Clinical Features • Pain in the right hypochondrium. • High fever, with rigors. • Weight loss. • Jaundice—occasionally. • Inter-costal tenderness. • Tender, soft liver. • Features of toxicity

Diagnosis • Ultrasound abdomen, CT scan. • LFT, total count. • Ultrasound guided aspiration of pus after controlling prothrombin time.

Treatment • Systemic antibiotics—combination of third generation cephalosporins and metronidazole. • Ultrasound guided aspiration/pigtail catheter. • Occasionally open drainage is required. • Treating the primary causes is very essential.

Complications • Septicaemia, liver failure. • Rarely rupture & peritonitis can occur. • Klebsiella hepatic abscess can cause dangerous endogenous endophthalmitis commonly in diabetic patients impairing vision.

Dr. B. Ramdas Rai Prof. & Unit Chief YMCH

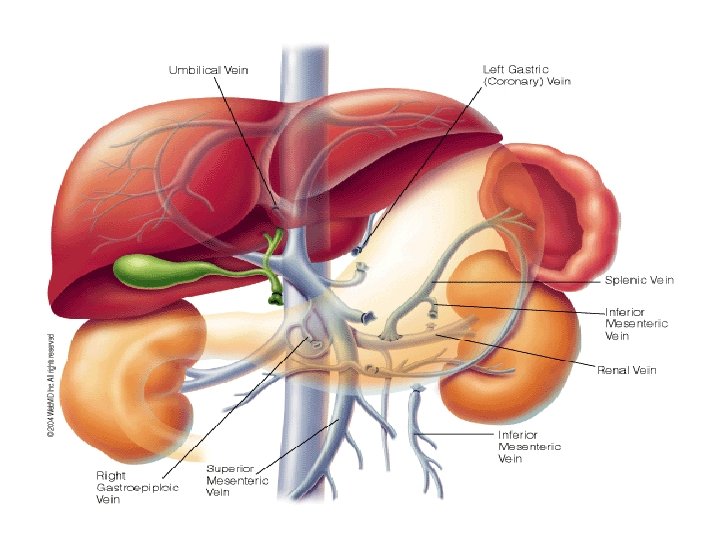
FORMATION q Portal vein is formed by confluence of SMV and Splenic vein q behind the neck of pancreas q at the level of L 1 or L 2 Portal vein is formed by confluence of SMV and Splenic vein behind the neck of pancreas at the level of L 1 or L 2

Anatomy of portal circulation • 5 – 8 cm long • 0. 8 cm diameter • Its main tributaries -Left gastric -Pyloric -Cystic -Pancreaticoduodenal

Contd… • In porta hepatis portal vein divides into two branches which goes to each lobe • Open into sinusoids • Empty into central veins • Sublobular veins • Interlobular veins • Hepatic vein -3 in no • IVC

PHYSIOLOGY OF PORTAL CIRCULATION • Hepatic blood flow – 1500 ml/min (25% of cardiac output) • Portal vein contributes 2/3 rd of the total hepatic blood flow • Hepatic arterial perfusion accounts for more than 50% of the livers oxygen supply

Contd… • Portal vein is a valveless structure resistance to Portal Blood Flow(at any level between right side of heart to splanchnic vessels) retrograde flow of blood from high pressure Portal Venous System to low pressure systemic venous circulation

DEFINITION

PATHOPHYSIOLOGY • Portal hypertension results from changes in portal resistance in combination with changes in portal inflow. • Ohm’s law is V = IR, where V is voltage, I is current, and R is resistance. This can be applied to vascular flow; ie, P = FR, where P is the pressure gradient through the portal venous system, F is the volume of blood flowing through the system, and R is the resistance to flow • This states that increases in portal resistance or portal flow can contribute to increased pressure. • Portal hypertension almost always results from increases in both portal resistance and portal flow

PATHOPHYSIOLOGY Role of Nitric Oxide in Portal Hypertension -NO is produced in the vascular endothelium from Larginine -It is a gas with a very short half-life -It is a local vasoactive factor -In vascular smooth muscle cells, NO induces a reduction of vascular tone. -Using inhibitors of NOS, have shown that an overproduction of NO contributes to portal hypertension
Gastric Zone : 2 -3 cms below the GE")
Zones of Gastro –Esopageal Varices 1)Gastric Zone : 2 -3 cms below the GE junction where the veins join & drain into short gastric & left gastric veins 2)Palisade Zone: Which extends for 2 to 3 cms in the lower esophagus 2)Perforating Zone: Where the network of submucosal veins connects via perforating veins the periesophageal veins. These perforating veins normally have valves that direct blood into the periesophageal veins. In portal hypertension, the valves of the perforating veins are incompetant & allow retrograde flow 4)The Truncal Zone: which is approximately 10 cms long & has 4 longitudinal venous columns.

PATHOPHYSIOLOGY • SEQUENCE OF EVENTS ü Block to portal flow leads to increased portal pressure ü Splanchnic vascular bed response - initial vasoconstrictor - secondarily vasodilator response ü Collaterals develop ü Plasma volume expansion
Cardio oesophageal junction (esophago gastric varices) 2) Periumbilical or")
Porto systemic collaterals-Sites Veins around 1)Cardio oesophageal junction (esophago gastric varices) 2) Periumbilical or abdominal wall collaterals 3)Retroperitoneal veins 4) Rectum (haemorrhoids) 5) Bare area of the liver

Clinical Features • Variceal bleeding • Ascites • Encephalopathy

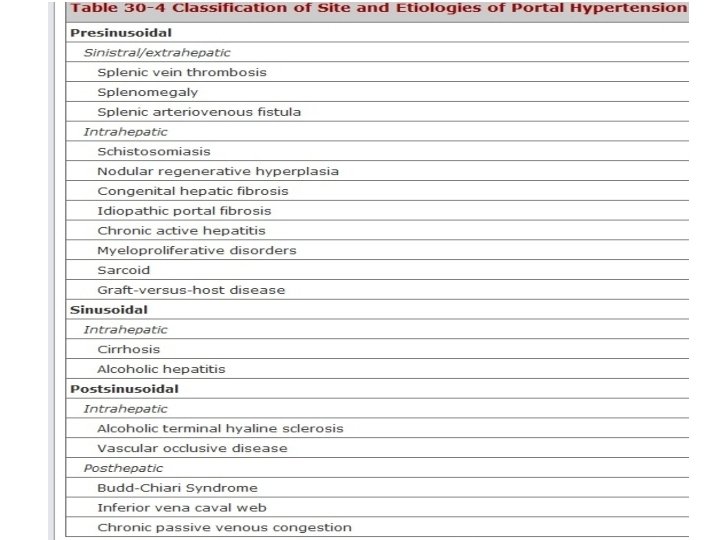
ETIOLOGY OF PORTAL HYPERTENSION
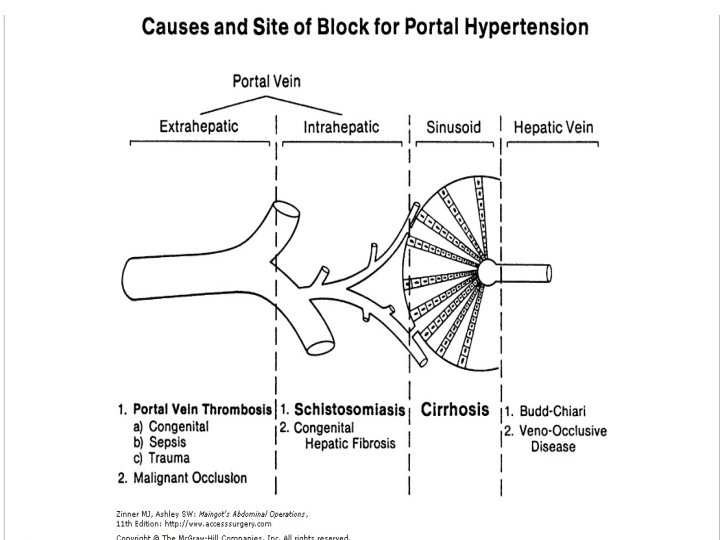

Portal Vein Thrombosis • Most common cause of Pre hepatic portal hypertension • Can be -Congenital - Sepsis - Trauma Accounts for almost 50% of cases of portal hypertension in childern

Contd… • When portal vein is thrombosed in the absence of liver disease, hepatopetal portal collaterals develop to restore portal perfusion • This combination is termed as cavernomatous transformation of the portal vein

Schistosomiasis • Schistosomiasis (also known as bilharzia caused by several species of trematodes (platyhelminth infection, or "flukes"), a parasitic worm of the genus Schistosoma hematobium. • Snails serve as the intermediary agent between mammalian hosts. • Individuals within developing countries who cannot afford proper water and sanitation facilities are often exposed to contaminated water containing the infected snails.

• After penetration of the skin, the schistosomulum travels to the lungs • It undergoes further developmental changes necessary for subsequent migration to the liver. • Eight to ten days after penetration of the skin, the parasite migrates to the liver sinusoids. • During this period that the parasite begins to feed on red blood cells. • Once fully formed they cause the congestion of the sinusoids leading to portal hypertension

Budd Chiari Syndrome • Budd-Chiari syndrome is a rare cause of postsinusoidal liver failure and cirrhosis, • The pathophysiology is related to thrombosis of the three major hepatic veins at the level of the inferior vena cava. • There may also be an associated web in the vena cava.

• The disease is more common in women and is associated with a variety of hypercoagulable states: ü protein C, S, or antithrombin III deficiency; polycythemia vera; ü estrogen exposure; ü myeloproliferative disorders.
Acute Form – Nausea, vomiting, severe pain in right")
Budd Chiari Syndrome CLINICAL PRESENTATION 1)Acute Form – Nausea, vomiting, severe pain in right hypochondrium, rapid enlargement of liver 2)Less sudden form – Rapid development of ascites, hepatic insufficiency, pedal edema 3)Chronic Type – Hepatic cirrhosis, ascites, oesophageal varices, infection- hepatic failure

• Transcutaneous Doppler-flow ultrasound will show thrombosed hepatic veins and may demonstrate large collaterals into the inferior vena cava. • CT findings include striking caudate lobe hypertrophy and inhomogeneous contrast enhancement. • Anticoagulation is the standard immediate therapy. • Liver transplantation is appropriate for patients with advanced liver disease, but is plagued by potential failure resulting from the underlying disorder

• Most common cause of portal hypertension in children – Portal vein thrombosis (PVT) • In PVT- Blood flow to liver maintained by collateral blood vessels ( cavernomatous transformation of portal vein

LEFT SIDED PORTAL HYPERTENSION : • Etiology : Due to isolated splenic vein thrombosis (secondary to pancreatic inflammation or neoplasm) • Clinical Features- Gastric varices • Cure can be achieved by a splenectomy

EVALUATION • Based on : ü Assessment of the liver disease ü Assessment of the portal circulation ü Upper gastro-intestinal endoscopy

HISTORY • Alcoholism • Hepatitis • Chronic biliary disease EXAMINATION • Jaundice • Ascites • Encephalopathy • Malnutrition • splenomegaly

Multidisciplinary Approach • • Hepatologists Gastroenterologists / Endoscopists Surgeons Radiologists Pathologists Critical Care Staff / Anaesthetists Nurse Clinicians / Support Team

INVESTIGATIONS AIM: a. To find cause of portal hypertension. b. To identify hepatic reserve. c. To define vascular anatomy. d. To find cause for GI hemorrhage

LABORATORY TESTS Liver function test : ü Hypoalbuminemia indicates chronic liver disease. ü Increased aspartate aminotransferase, alanine aminotransferase indicates ongoing hepatocellular necrosis. ü Increased alkaline phosphatase indicates intra/extra hepatic cholestasis. ü Increased PT and Bilirubin indicates hepatic decompensation. ü Serology for hepatitis B and C virus.
 Hypokalemia, 2)Hyponatremia and 3)Metabolic alkalosis secondary to diarrhoea")
• Serum electrolytes : 1) Hypokalemia, 2)Hyponatremia and 3)Metabolic alkalosis secondary to diarrhoea and recurrent emesis. Consequences: Impairs tissue oxygen delivery Converts NH 4 cl to NH 3 - Hepatic encephalopathy

The two main scoring systems for liver disease severity are: • Child Pugh Score • Model for End Stage Liver Disease(MELD)

CHILD- PUGH CLASSIFICATION Measure Serum bilirubin Serum albumin PT prolongatio n Ascites Neurologic disorder 1 2 <2 2 -3 >3. 5 1 -3 sec. 2. 8 -3. 5 4 -6 sec. 3 >3 <2. 8 >6 sec. None Slight Moderate None Minimal Advanced
 + 0. 378 x")
• MELD Score = 0. 957 x loge creatinine(mg/dl) + 0. 378 x loge bilirubin (mg/dl) + 1. 120 loge INR

Class determined on the basis of total points scored: 5 to 6 points - class A 7 to 9 points - class B 10 to 15 points - class C MELD Score Good Risk Patient <10 Indeterminate patient 10 to 16 End Stage Liver Disease >16

IMAGING • • Ultrasound CT/MRI Doppler ultrasound Liver Biopsy

CT Angiogram Portal venous anatomy

Hepatic Venous Pressure Gradient • Portal pressure is measured indirectly from hepatic veins • Difference between wedged & free hepatic vein pressures = HVPG • Done with a balloon occlusion technique similar to Swan Ganz measurement in pulmonary circulation • Normal HVPG= 6 to 8 mm. Hg

ESOPHAGEAL VARICES

Haemorrhage Fundal varices with Portalgastropathy

VARICEAL HAEMORRHAGE • Life threatening complication of portal hypertension • 30% of patients with cirrhosis develop portal hypertension • 30% of patients with portal hypertension will bleed from varices within 2 years

PATHOPHYSIOLOGY • Laplace’s Law The tension on the wall of a sphere = Pressure X Radius of the chamber and the tension is inversely related to the thickness of the wall. • Application – Variceal wall tension is directly related to transmural pressure and varix radius and inversely related to variceal wall thickness, thus combining all three of these variables

Staging Systems • Italian Endoscopic Staging • Japanese Staging • Sarins Staging

Italian Endoscopic Staging • Grade 1 – Minimal varices without luminal prolapse <30% • Grade 2 – Large varices with luminal prolapse & with moderate obscuring of OG junction 3060% • Grade 3 – Very large varices, with luminal prolapse & with complete obscuring or OG junction >60%
The extent(distance")
Japanese Staging • In this classification the oesophageal varices are described by 1)The extent(distance of from GE in cms) 2)Size (F 0 -no varices, F 1 small & non tortuous, F 2 - tortuous but less than 50% radius, F 3 large & tortuous 3)Color (blue or white) 4)Presence of red signs (red wale markings, cherry red spots, hematocystic spots)

Sarins Classification GOV 1 – Gastro-oesophageal varices extending down the lesser curvature, more or less straight GOV 2 – Gastro-esophageal varices extending into the fundus of stomach, long & tortuous IGV 1 - Isolated gastric varices in the fundus IGV 2 - Isolated ectopic varices at other sites in stomach & duodenum

MANAGEMENT The therapies available for treating variceal bleeding are: • Pharmacotherapy • Endoscopic therapy • Decompressive shunts – radiologic or surgical • Devascularisation operations • Liver transplantation

PHARMACOTHERAPY • It plays an important role in: ü ü ü Preventing the initial bleed Managing the acute variceal bleed As first line treatment in preventing rebleeding

PHARMACOTHERAPY • • Beta blockers- Inderal, Nadolol Vasopressin Octereotide Terlipressin Nitrates Serotonin antagonists Calcium channel blockers

PHARMACOTHERAPY • • Beta blockers- Inderal, Nadolol Used since 1980’s in prophylaxis Also used as intial therapy in rebleeding Patients with moderate to large sized varices should be placed on these Dose • Inderal- 20 mg/12 hrs • Nadolol- 10 mg/day

PHARMACOTHERAPY • Vasopressin was the 1 st drug used in acute variceal bleeding– 20 units in 100 ml 5% glucose Iv over 10 mins, repeated 3 to 4 times at hourly intervals • Somatostatin & its analogues- 250 microgram as bolus followed by 250 microgram/hr for 2 to 5 days • Octreotide (50 ug/hr) • Terlipressin- 2 mg IV 6 th hrly till bleeding stops, 1 mg 6 th hourly for further 24 hrs

• Patients who have more than >20% reduction in their Hepatic Venous Pressure Gradient or Who reduce their Hepatic Venous Pressure Gradient to <12 mm. Hg will not bleed

Endoscopic Therapy • Most commonly used therapy, controls bleeding in 85% of patients Methods Sclerotherapy Band ligation

Sclerotherapy • Sclerosants used: ü Sodium tetradecyl sulphate, ü Polidocanol, ü Sodium morrhuate, ü Ethanolamine oleate, ü Absolute alcohol ü Cyanoacrylate glue for gastric varices • Technique : Intravariceal ligation Paravariceal ligation Combined
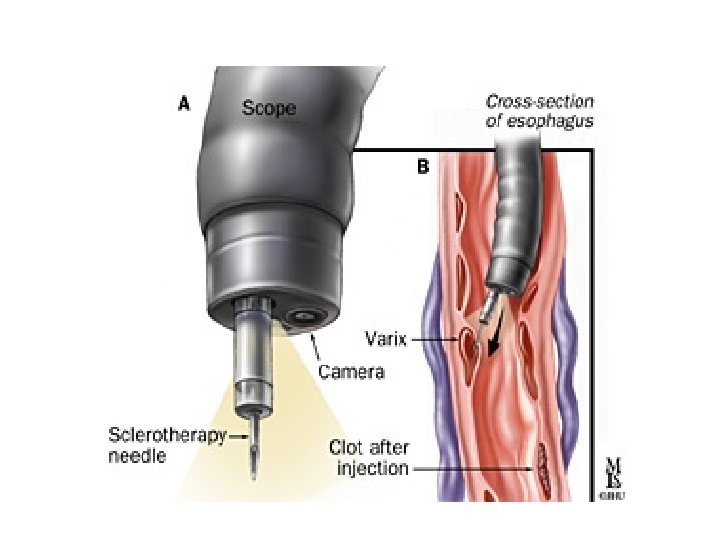

Intravariceal injection of esophageal varices

Paravariceal injection

Combined intra and paravariceal ligation

Complications : -Esophageal ulceration -Esophageal perforation, -Worsening of variceal haemorrhage

Band ligation • More effective • Fewer complicati ons

Steps Varix drawn into ligator by suction

Band applied

Balloon Tamponade • Sengstaken-Blakemore tube Minnesota tube § Consists of 3 tubes & 2 baloons • Disadv 1)Frequent recurrent haemorrhagege • 2)Discomfort to patient 3)Oesophageal perforation 4)Ischaemic necrosis of oesophagus

Modified Sengstaken Blakemore tube
 Indications : 1) Short term bridge to liver transplantation in")
Transjugular Intrahepatic Portosystemic Shunt(TIPS) Indications : 1) Short term bridge to liver transplantation in patients with recurrent bleeding , poor liver function. 2)As definitive therapy in acute bleeding not controlled by less invasive treatment. Disadvantages • It is a non-selective shunt • Shunt stenosis or occlusion develops in 50% of patients with in one year

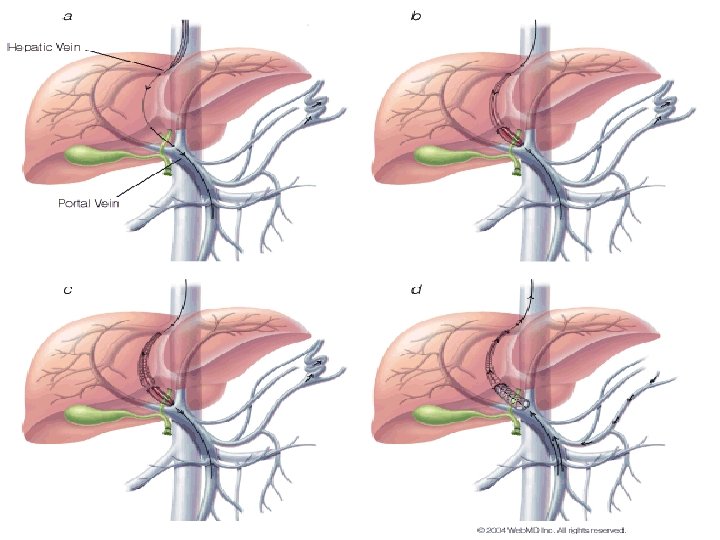
TIPS - Steps
Done under LA and sedation 2)A guide wire is inserted via Right Internal Jugular")
1)Done under LA and sedation 2)A guide wire is inserted via Right Internal Jugular vein, Superior Venecava and into a hepatic vein
The needle is punctured through hepatic parenchyma to enter the main Right portal vein")
3)The needle is punctured through hepatic parenchyma to enter the main Right portal vein
This parenchymal tract is then dilated with a baloon catheter placed over guide wire")
4)This parenchymal tract is then dilated with a baloon catheter placed over guide wire
Finally metallic stent is placed in dilated parenchymal tract thus creating the shunt")
5)Finally metallic stent is placed in dilated parenchymal tract thus creating the shunt

TIPS as seen on an angiographic study after stent placement

Complications • Restenosis • Thrombosis • Early Thrombosis – Bile duct puncture • Late stenosis – Most commonly occurs at the hepatic vein end

DECOMPRESSIVE SHUNTS • This mode of management has changed dramatically over last 2 decades. • Considered as second line treatment • Reserved for patients who rebleed through endoscopic banding & beta blockers or whose varices remain “high risk”

SHUNT PROCEDURES • MOA Decompress portal venous system by shunting portal blood into low pressure systemic circulation • Complications : Portosystemic encephalopathy Accelerated hepatic failure

Porto systemic shunts Depending on whether they completely decompress, compartmentalize or partially decompress- v. Non selective (Total) v. Selective v. Partial

Non selective shunts
 § Portal vein divided close to liver §")
End to Side Anastomosis (Eck Fistula) § Portal vein divided close to liver § Lower end anastomosed to side of IVC § Decompresses portal hypertension § Does not relieve ascites

Side to side anastomosis • Portal vein and IVC are connected in side to side fashion • Shunts – 12 to 15 mm • Intact upper end of the portal vein Indication -To relieve ascites -Prevent recurrent variceal bleed

Interpositional shunts • Synthetic graft or autologous vein is interposed between portal and systemic venous circulation • Three types Portocaval Mesorenal

Contd… ADVANTAGE-Easy to reconstruct -Hepatic hilum avoided -Easily occluded if intractable post shunt encephalopathy develops DISADVANTAGEHigh graft thrombosis rate

CONVENTIONAL SPLENORENAL SHUNT • Anastomosis of proximal splenic vein to left renal vein after performing splenectomy • Adv – Hypersplenism avoided • Disadv Shunt thrombosis common (small prox. vein)
 • Left Gastric Venecaval shunt (Inokuchi")
Selective shunts • Distal splenorenal shunt (Warren’s shunt) • Left Gastric Venecaval shunt (Inokuchi shunt)

Distal Spleno Renal Shunt • Separate splenic vein from posterior surface of pancreas, • Interrupt all major collaterals • Splenic vein is ligated at junction with portal vein portal end ligated • Distal splenic end anastomosed to left renal vein

ü Selectively decompresses the gastroesophageal varices ü Most Commonly used in Child’s Class A & B ü Results in separation of portal venous circulation into a decompressed gastrosplenic venous circuit & high pressure superior mesentric venous system continues to perfuse the liver

• Contraindications for Warren shunt ü Presence of ascites ü Splenic vein diameter <7 mm ü Prior splenectomy • Warren shunt becomes non selective in patients with alcoholic cirrhosis due to pancreatic collateral network which can be avoided by splenopancreatic disconnection

Partial shunts • Objectives -Preserve blood flow to liver -Produce effective decompression of varices -Preservation of some residual portal hypertension
 prosthetic graft placed between IVC and Portal")
Partial shunt Small diameter (8 -10 mm) prosthetic graft placed between IVC and Portal vein

DEVASCULARISATION PROCEDURES • Aim : To disconnect venous drainage of stomach and oesophagus from liver and intestinal vessels • It prevents variceal bleeding by interrupting inflow into the varices • Portal flow to the cirrhotic liver is maintained • Most effective procedure : Sugiura procedure

• Originally a combined abdominal & thoracic procedure • Now mainly done as an abdominal procedure • Devascularisation -Whole of greater curvature of stomach -Atleast 7 cm of distal oesophagus -Upper 2/3 rd of lesser curvature of stomach

Sugiura procedure Oesophageal transection, esophagogastric devascularisation, splenectomy and either SV with pyloroplasty or HSV without pyloroplasty

Sugiura procedure • Useful when patients have extensive portal & splenic vein thrombosis & no other operative or radiologic options are available

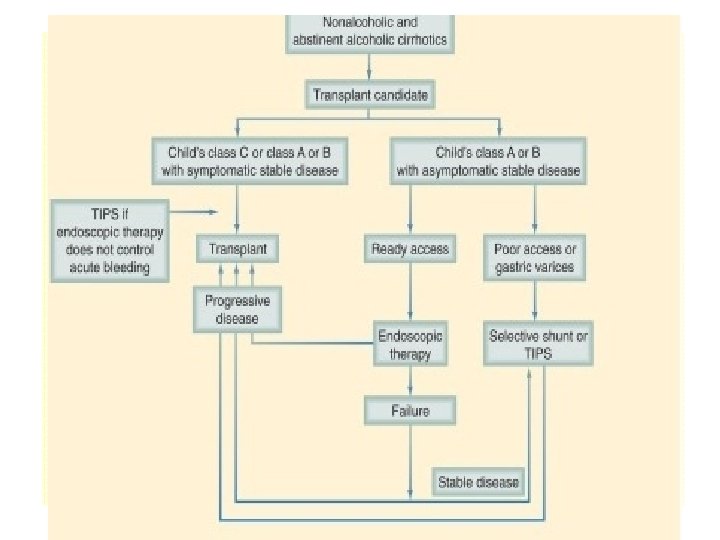
Hepatic transplantation • Indication : Non alcoholic cirrhotic patients and abstinent alcoholic cirrhotic patients with either limited hepatic reserve (Child’s class B and C) or a poor quality of life secondary to their disease after controlling acute hemorrhage

Management Stratergies • Prophylaxis • Acute Variceal Bleed • Prevention of Rebleeding

PROPHYLAXIS -Beta blockers should be used - Bleeding is reduced from 30% to 18 -20%

• ACUTE VARICEAL BLEED Overall managementü Airway protection ü Appropriate fluid resuscitation ü Adequate monitoring ü Antibiotic prophylaxis ü Transfusion of blood for bleeding ü Blood products for coagulopathy

• Pharmacologic therapy with octreotide • Early endoscopy • Baloon tamponade in patients who cant undergo banding • Emergency TIPS is rarely used

Prevention of rebleeding • Variceal banding + pharmacotherpy – 1 st line • Banding should be performed within 1 st 4 to 5 days of acute bleed • Good risk patient(Child A or MELD <10) • Indeterminate patient(Child’s B or MELD 1016) • End stage liver disease(Childs C or MELD >16)

Acute Variceal Bleed

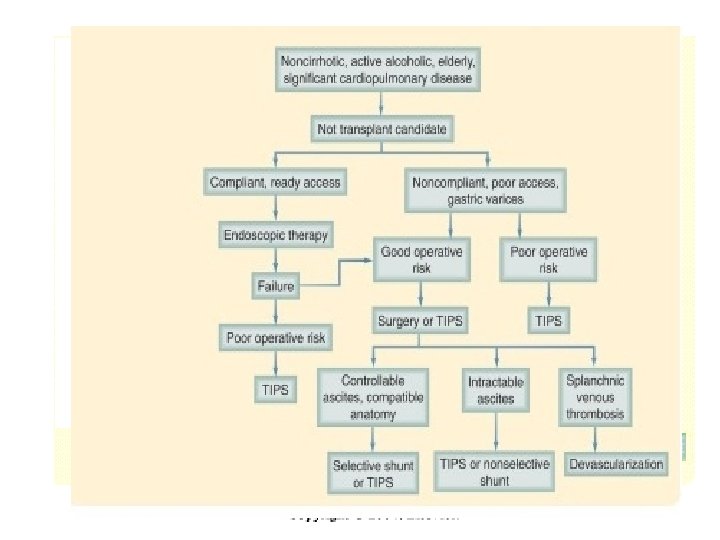
Algorithm for definitive therapy of variceal hemorrhage

Ascites

Ascites • Pathogenesis : Altered hepatic and splanchnic hemodynamics cause transudation of fluid into interstitial space When the rate of interstitial fluid formation exceeds the lymph drainage capacity, ascites accumulates • Indicator of Advanced liver disease
 + Spironolactone 100 -400 mg/day) –")
Ascites-Treatment • Salt restriction (20 -30 m. Eq/day) + Spironolactone 100 -400 mg/day) – First line of treatment • Loop diuretics can be added if above regimen fails. • Intermittent abdominal paracentesis +/- colloid infusion also effective. • Refractory cases – Surgery • Peritoneovenous shunt – rarely used because of increased morbidity • Side to side portocaval shunt or TIPS can be done

Encephalopathy • Portosystemic encephalopathy may have a variety of manifestations, including ü alterations in the level of consciousness, ü intellectual deterioration, ü personality changes, and ü neurologic findings such as the flapping tremor, asterixis. • They occur in patients with either significant hepatocellular dysfunction or portosystemic shunting.

• Pathogenesis of encephalopathy are based on circulating cerebral toxins that are intestinally absorbed and bypass the liver by means of shunts or fail to be inactivated by the liver's decreased metabolic capacity. • Cerebral toxins include ammonia, mercaptans, and γ-aminobutyric acid. • These substances are normally derived from the intestine & detoxified in the liver

• Key to the management of encephalopathy is identifying and then eliminating whatever precipitating factors are responsible. • Dietary protein is restricted, • Infections are treated, • All sedatives are discontinued, and • Intestinal catharsis is accomplished

Treatment • Treatment or removal of precipitating cause • Correct electrolyte imbalance • Eliminate dietary protiens to suppress production of neurotoxins by the bacteria in the bowel

Treatment • The only drugs with proven effectiveness are neomycin, a poorly absorbed antibiotic that suppresses urease-containing bacteria, and • Lactulose, a nonabsorbable disaccharide that acidifies colonic contents and also has a cathartic effect. • A likely mechanism of action of both of these drugs is a decrease in the amount of intestinal ammonia and inhibition of its absorption. • Neomycin is administered orally in a dose of 1. 5 g every 6 hours. • In the acute setting, lactulose is given in a dose of 30 g every 1 or 2 hours until a cathartic effect is noted. .

CONCLUSION q. Surgical intervention becoming a rarity except in those with end stage liver disease q. With the advent of TIPS indications for surgical shunts decreasing q. Choice of a surgical procedure depends most importantly on expertise of surgeon

- Slides: 122