PULP PERIAPICAL DISEASES INNERVATION Nerve supply follows distribution

PULP & PERIAPICAL DISEASES

INNERVATION § Nerve supply follows distribution of the blood vessels. § Majority are nonmyelinated & in close association with blood vessels. § Many are sympathetic in nature. § Terminals are on the muscle cells of larger vessels and function in vasoconstriction.

§ Large myelinated fibers mediate the sensation of pain. § Parietal layer of nerves has plexus of Rashkow. § Nerve axons from the parietal layer either terminate at the pulp-predentine border or in the dentinal tubules. § Sensory response in the pulp cannot differentiate between heat, touch, pressure or chemicals.

Neuroanatomy § Sensory nerves supplying the pulp are mixed. § Myelinated axons are classified according to diameter & conduction velocity: - A δ- 1 to 6 µm, slow conducting myelinated, numerous. - A β- 6 to 12 µm , faster conducting myelinated. § Stimulation of these fibers result in fast, sharp pain, localized.

§ Nonmyelinated Nociceptive axons or C fibers most numerous. § Chiefly in the pulp core. § Stimulation produces slow, Dull & diffuse pain.

Pulp testing § Electric pulp tester delivers a current sufficient to overcome enamel & dentine resistance & stimulate sensory A fibers at the pulp-dentine border zone. § Tests activate hydrodynamic forces which excite intradental A fibers. § C fibers are not activated.

DISEASES OF PULP
: 1) Almost totally surrounded by")
Factors that makes the pulp unique (in inflammatory process): 1) Almost totally surrounded by hard tissue (dentin)—limits the area for expansion. 2) Total lack of collateral circulation- limit its ability to cope up with bacteria, necrotic tissue& inflammation. 3) Posses –unique cell- odontoblast, & cells that differentiate into hard tissue secreting cells—form dentin to protect pulp from injury. 4) Biopsy & direct medication is impossible without causing necrosis of entire pulp.

Etiology of pulpal diseases Accor. To Grossman’s v Mechanical v Thermal v Electrical v Chemical v Bacterial

Classification of Pulp diseases Main basis of pulp classification can be § According to duration & inflammation § Whether it involve total or partial pulp § According to direct communication with oral cavity § Whether it is infected or sterile § Clinical classification based on symptoms § Whether it is treatable or untreatable

Grossman According to
 2. Pulp degeneration 1. Reversible Pulpitis a. calcification a. Symptomatic (acute)")
1. Pulpitis (inflammation) 2. Pulp degeneration 1. Reversible Pulpitis a. calcification a. Symptomatic (acute) b. others b. Asymptomatic ( chronic) 3. Necrosis 2. Irreversible pulpitis Acute a. abnormally responsive to cold b. abnormally responsive to heat Chronic a. asymptomatic with pulp exposure b. hyperplastic pulpitis c. internal resorption

ACCORDING TO INGLE 1. INFLAMMATORY CHANGES/ HYPERACTIVE PULPALGIA a. Hypersensitivity b. Hyperemiaacute- decreased flow blood chronic-decreased drainage of venous blood 2. ACUTE PULPALGIAa. incipient b. moderate

3. CHRONIC PULPALGIAa. Hyperplastc pulpitis b. Necrosis of pulp 4. DEGENERATIVE CHANGESa. Atrophic changes b. Calcific pulposis
 § Focal reversible Pulpitis § Acute Pulpitis or")
§ According to Shafer Pulpitis (inflammation) § Focal reversible Pulpitis § Acute Pulpitis or Chronic Pulpitis a. partial b. subtotal c. total According to communication with oral cavity a. open b. closed § Chronic hyperplastic Pulpitis § Gangrenous necrosis of pulp

Reversible pulpitis Pulp hyperemia – § It is mild to moderate inflammatory condition of pulp caused by a noxious stimuli in which the pulp is capable of returning to uninflammed state following removal of stimuli.

Symptoms Ø Sharp , shooting , lancinating pain caused by cold stimuli, lasting for only moments. Ø Pain occurs spontaneously. Ø Pain disappears on removal of stimulus. Ø Tooth responds to stimulation by electric pulp tester at lower level of current than that of adjacent normal teeth Ø Teeth exists usually deep carious lesions or restorations with defective margins

H/p Ø The lesion show predominantly acute inflammatory cell infiltration & inflammation is localized at base of involved tubules. Ø Dilation of pulpal blood vessels with increase in vascular permeability. Ø Edema of tissues. Ø Acute inflammatory cell infiltration. Ø Reparative dentin formation

§ Diagnosis Ø Pain—sharp—brief duration ceasing when irritant is removed. Ø Visual examination-may show caries/traumatic occlusion & undetected fracture. Ø Radiographs- normal Pdl and lamina dura depth of caries or cavity penetration may be evident. Ø Vitality test- responds to cold. Ø Electric pulp test – less current to cause pain

Irreversible pulpitis § It is persistent inflammatory condition of pulp, symptomatic or asymptomatic caused by noxious stimuli. § It has both acute and chronic stages in pulp. § In acute phase usually caused by hot or cold stimulus or pain occurs spontaneously. § Pain persist for several min. to hours , lingering

ØSymptoms Ø Early stage pain is spontaneous , sharp , piercing or shooting. Ø Rapid onset of pain which lingers after removal of stimuli. Ø Pain exacerbates on lying down or bending due to change in intrapulpal pressure. Ø Pain is often continuous , Referred pain. Ø Later stages pain is severe , boring, throbbing which increases with hot stimulus. Ø Patient often kept awake at night due to pain. Ø Pain is increased by heat & relieved by cold, although continued cold may intensify the pain.

Histopathology § Acute Pulpitis § The dilated and engorged capillaries surrounded by many neutrophils are classic microscopic features of acute inflammation; therefore, this is acute pulpitis.

§ Acute Pulpitis § Early in the course of disease, PMNLs are confined to localised area & the remenders of the pulp tissue appears relatively normal even at this period, there may be localised destruction of pulp tissue & formation of small abscess § When such abscesses are seen on microscopic examination they are known as "microabscesses. “

§ Chronic Pulpitis § This section reveals a "mixed" inflammatory reaction. The dilated capillaries and neutrophils suggest "acute inflammation, " while lymphocytes and fibroblasts suggest "chronic inflammation. " The lesion is changing from acute to chronic inflammation.

§ Diagnosis Ø Visual examination and history Ø Radiographs shows extent of caries periapical area may be normal. Ø Percussion – tender ( increased intrapulpal pressure)

Vitality test Thermal test – Responds more readily to cold. But, inflammation progresses heat intensifies the response (expansible effect on blood vessels). Electric pulp test- Initial stages– less current required. As tissue becomes necrotic more current required.
 Pain")
DIFFERENTIAL DIAGNOSIS OF REVERSIBLE AND IRREVERSIBLE PULPITIS: FEATURES REVERSIBLE PULPITIS IRREVERSIBLE PULPITIS 1) Pain type Sharp and fleeting pain, ceases after stimulus is removed External stimulus Intense, continous and prolonged 3) Pain at night/ postural No Yes 4) Referred pain Not usually found Common finding 2) Stimulus No external stimulus
 History 6) Percussion/ Occlusion 7) Pulp tests a) EPT b) Cold Any history")
5) History 6) Percussion/ Occlusion 7) Pulp tests a) EPT b) Cold Any history of recent History of caries, dental procedures. trauma, extensive restoration. If due to occlusion If PDL involved percussion test positive otherwise normal. Normal response Exaggerated response c) Heat 8) Color change Normal exaggerated response No Normal to elevated response Pain relieved by cold occasionally Acute pain Yes
 Radiograph Caries, defective or unbased restoration. Caries, defective restorations PDL space enlargement 10)Treatment")
9) Radiograph Caries, defective or unbased restoration. Caries, defective restorations PDL space enlargement 10)Treatment Removal of decay, repair of defect, restoration, ZOE dressing, occlusal adjustment. Pulpectomy, pulpotomy, occlusal adjustment.

§ Treatment Ø Pulpectomy Ø Pulpotomy for posterior tooth as an emergency procedure Ø Extraction of unrestorable tooth § Prognosis- favorable if pulp is removed and proper endodontic therapy and restoration

PULP ABSCESS § If the carious process continues to advance towards the pulp , local destruction will probably increase in the pulp. § When the injury is sufficient great , cause death of the large number of leukocyte , pus is formed. § If the tissue response & vascular supply are good abscess is walled off locally, by the formation of fibrous barrier, to form a local pulpal abscess known as cornual
 § Tooth is hypersensitive to")
§ Patient may complaint of pain. (Slight or intermittent) § Tooth is hypersensitive to thermal stimuli. § Respond normally to vitality test. § mostly seen in pulp horn.

§ H/P - It shows a zone of tissue necrosis & dead leukocyte lying in contact with the tubules involved by caries. § This zone is usually roughly hemispherical in form. § It is surrounded by a zone of heavily infiltrated tissue showing edema & necrosis. § Outside the zone is an area of less damage, in which vessel are dilated , granulation tissue & fibrous tissue formation may be found attempting to wall

Chronic hyperplastic pulpitis pulp polyp § Definition § It is a productive pulpal inflammation due to an extensive carious exposure of young pulp. § There is a development of granulation tissue, covered by epithelium and resulting from long standing , low grade irritation. § Nature of pulp response depends on, - Strength & duration of irritants - Resistance of pulp - Extent of tissue affected


§ Etiology Ø Slow, progressive, carious exposure of pulp. Ø Mechanical irritation and bacterial infection. Ø For its development a large open cavity, young resistant pulp, chronic low grade stimulus is necessary. § Symptoms § Asymptomatic , except during mastication when pressure of food bolus may cause discomfort. § Bleeds easily on probing, common in

§Histopathology Ø pulp polyp is a complex of new capillaries, proliferating growth of inflammed connective tissue, fibroblasts & inflammatory cells Ø Sensory nerve elements almost totally absent near the surface Ø As tissue expands it may acquire cover of stratified squamous epithelium Ø The tissue in the pulp chamber transformed in to granulation tissue.

§ Diagnosis Ø Seen in children and young adults. Ø Pain usually absent. Ø Fleshy , reddish pulpal mass fills most of the pulp chamber or cavity or extends beyond confines of tooth. Bleeds easily on probing. § Vitality tests: The tooth may respond feebly/ not at all to thermal tests. § Electric Pulp tests: More current than normal is required. § Differential diagnosis-proliferating gingival tissue Treatment complete removal of pulp followed by restoration

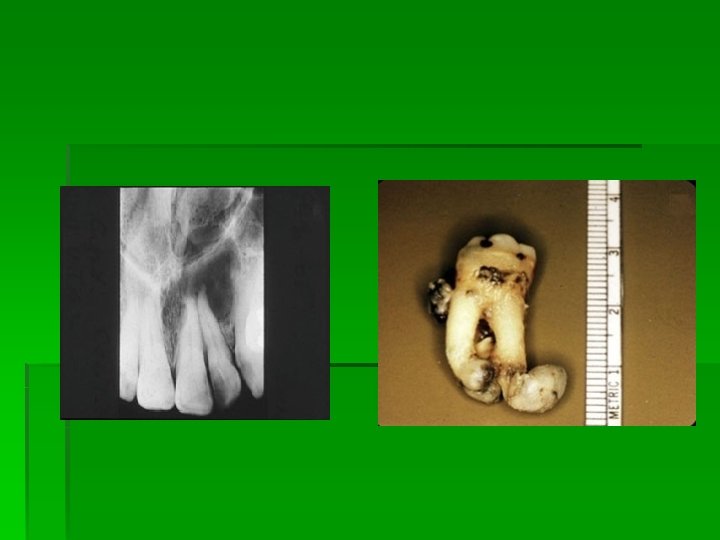
Internal resorption Odontoclastoma/ Pink tooth of mummery/ § Definition It is an idiopathic slow or fast progressive resorptive process occurring in the dentin of the pulp chamber or root canal of teeth. § Etiology § Unknown. § history of trauma. ( either a blow or restorative procedures. )

§ Mechanism of resorption Pulp inflammation due to infection Alteration or loss of predentin layer and odontoblast Undifferentiated mesenchymal cells come in contact with mineralized dentin Differentiate into dentinoclast Resorption results

Symptoms: ØClinically asymptomatic. ØIn crown reddish area can be seen which is called pink spot. ØThis reddish area represents the granulation tissue showing through the resorbed area of the crown.

§ Histopathology Ø Osteoclastic activities seen in lacuna, which may be filled in by osteoid tissue. Ø Granulation tissue seen. Ø Multinucleated giant cells or dentinoclast present—(identical to osteoclasts). Ø Lost predentin & dentin are replaced by chronic inflammatory tissue. Ø Metaplasia of pulp tissue by deposition of hard tissue looks like a bone or cementum.

§ Diagnosis Ø Clinically – pink spot seen later. Ø Radiaographic changes radiolucent enlargement of wall of pulp chamber and root canal outline is distorted. Ø Pulp test-positive if apical pulp is vital. § Treatment Ø Pulp extirpation Ø Root canal treatment Ø If root perforation occurs

§ Prognosis Best before root perforation. If root and crown perforation occurs then guarded depending upon formation of calcific barrier or access to perforation that permits surgical repair.

PULP DEGENERATION: n n Degeneration is generally present in the teeth of older people The specific types of pulp degeneration are: CALCIFIC DEGENERATION –in this part of the pulp tissue is replaced by calcific material. Types: 1. Dystrophic calcifications ( in dead & degenerated tissue) 2. 3. Diffuse Calcifications( generally observed in root canals) Denticles / Pulp stones ( usually seen in pulp
 free 2) embedded 3)")
Denticles / Pulp stones Classification : According to location: 1) free 2) embedded 3) Attached According to structure: 1) true 2) false
 Atrophic Degeneration n 2) Fibrous")
PULP DEGENERATION ACCORDING TO HISTOPATHOLOGICAL DIAGNOSIS IS FOLLOWS: 1) Atrophic Degeneration n 2) Fibrous Degeneration n

Atrophic degeneration Ø Seen histopathologicaly in older people. Ø Fewer spindle shape cells seen. Ø Intercellular fluid increases. Ø collagen fibers/unit area increased leading to fibrosis. Ø Pulp is less sensitive than normal.

Fibrous degeneration Ø Characterized by replacement of cellular elements by fibrous connective tissue. Ø On removal of pulp from the canal such pulp has a characteristic appearance of a leathery fiber. Ø It is asymptomatic condition.

Pulp necrosis § Definition Necrosis is death of pulp. May be partial or total, depending on extent of pulp tissue involvement. § Types Ø Coagulation necrosis – the soluble portion of tissue is precipitated or is converted into solid material. Ø Liquefaction necrosis — when proteolytic enzymes convert the tissue into a softened mass , a liquid or amorphous debris.

§ Etiology Can be caused by any noxious insult , injury to pulp such as bacteria, trauma or chemical irritation. § Symptoms Ø Tooth might be asymptomatic. Ø Discoloration of tooth-- first indication of pulp death. Ø Dull or opaque appearance of the crown.

§ Diagnosis Ø Pain: absent in complete necrosis. Ø History of patient: Past trauma or past H/O of severe pain lasting for few mins to few hours followed by sudden and complete cessation of pain. Ø Radiographs show large cavity or filling. an approach to root canal. Ø Vitality tests ; negative. -multirooted teeth may show mixed response. -Teeth with liquefaction necrosis– may show

§ Histopathology: necrotic pulp tissues, cellular debris, microorganisms seen in pulp cavity. liquefaction necrosis (microabscess) in response to carious exposure

Treatment Preparation and obturation of root canal Prognosis Favorable with proper endodontic therapy

PERIAPICAL DISEASES

Diseases of the periradicular tissue According to Grossman § Acute periradicular diseases Acute alveolar abscess Acute apical periodontitis a. vital b. nonvital § Chronic periradicular diseases Chronic alveolar abscess Chronic apical periodontitis( Granuloma) Radicular Cyst (periapical cyst) § Chronic periradicular disease with condensation § Miscellaneous External root resorption Periradicular disease of non-odontogenic origin
 Acute apical periodontitis Chronic apical periodontitis( Granuloma) Apical")
Diseases of the periapical tissues (Shafer) Acute apical periodontitis Chronic apical periodontitis( Granuloma) Apical periodontal cyst Residual cyst Periapical abscess Osteomyelitis

Sequela of pulpitits

ACUTE APICAL ABSCESS ACUTE ALVEOLAR ABSCESS ACUTE PERIAPICAL ABSCESS ACUTE RADICULAR ABSCESS DENTO ALVEOLAR ABSCESS

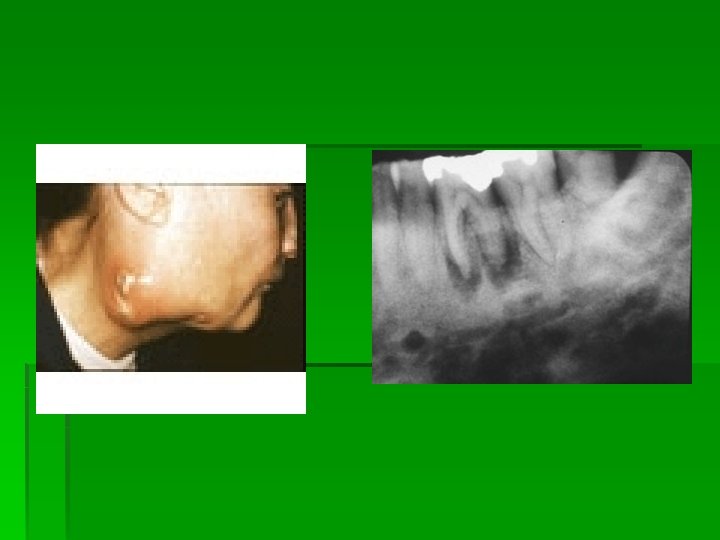
ACUTE ALVEOLAR ABSCESS § An acute alveolar abscess is a localized collection of pus in the alveolar bone at a root apex of the tooth following death of the pulp. § It is a continuance of the disease process beginning in the pulp and progressing to the periradicular tissue.

§ Symptom§ First symptom may be mere tenderness of the teeth that may be relieved by continued slight pressure on the extruded tooth § Later severe and throbbing pain , with swelling of the overlying soft tissues. § Tooth becomes more painful , elongated and mobile. § Regional lymphadenitis , fever present.

Chronic periapical abscess § Chronic periapical abscess present no clinical feature , well circumscribed area of suppuration that show little tendency to spread from the local area. § Radiographically slight thickening of the periodontal ligament. § Chronic abscess shows ill defined borders. § Because of pulp tissue is solidly enclosed , no drainage is possible & the infection continues to extend in the direction of

§ H/P – The area of suppuration is composed of central area of disintegrating PMN surrounded by leukocyte , lymphocyte , cellular debris , necrotic material and bacterial colonies. There is dilatation of blood vessels in pdl and marrow of the bone. Treatment Ø Drainage & antibiotics Ø Root canal treatment

§ Note the radiolucency at the apices of the central and lateral incisors and that the tooth with the root canal filling has no periapical radiolucency. It is the radiolucent lesion that gave rise to the abscess in the labial vestibule

§ Periapical Abscess § This blood and pus-filled lesion represents extension of acute periapical inflammation onto a nearby surface. § There is a "bump" on the gingiva and is a drainage outlet from periapical inflammation around this non-vital mandibular cuspid; it is known as a "parulis" or "gum boil. "

§ ACUTE APICAL PERIODONTITIS § Acute apical periodontitis is a painful inflammation of the periodontium as a result of trauma , irritation, infection. Causes – § Occlusal trauma § Over filling § Bacterial infection Symptom§ Pain and tenderness of teeth. § Slightly sore § Extruded tooth from socket.

Bacteriology - Pulp may be sterile , if periodontitis is due to a blow , a occlusal trauma , chemical irritation during endodontic treatment. Bacteria grow beyond the apical foramen may irritate the apical periodontal tissue. § H/P§ An inflammatory reaction occur in the apical periodontal ligament. § The blood vessel are dilated , PMN are present. § Serous exudate distends the periodontal

§ Differential diagnosis Acute alveolar abscess. § Treatment § Removal of the cause.
 § Chronic apical periodontitis is a")
§ CHRONIC APICAL PERIODONTITIS ( PERIAPICAL GRANULOMA ) § Chronic apical periodontitis is a low grade infection & one of the most common of all sequelae of pulpitis. § If the acute process is left untreated , it is incompletely resolved & becomes chronic. § It is essentially a localized mass of chronic granulation tissue formed in response to the infection.

LYMPHOCYTES 70

Macrophages 71

Epithelioid cells 72

Giant cells 73

fibroblast 74

Necrosis ± 75

76

§ A granuloma is an organized collection of macrophages, surrounded by lymphocytes, epithelioid cells & fibroblasts with or without necrosis. § The goal of granuloma formation is to destroy an antigen or isolate foreign body. 77

§ C/F § Involve nonvital teeth. § Slightly tender to percussion may produces a dull sound because of granulation tissue around root apex. § Patient may complain about mild pain on biting or chewing on solid food. § Tooth feels slightly elongated in its socket. § Sensitivity is due to hyperemia edema, inflammation of the apical periodontal ligament.

§ Asymptomatic , there is no perforation of overlying bone. § Radiographically – - Thickening of ligament at root apex seen. - Granuloma appear as a well circumscribed radiolucent lesion at the root apex is seen.

§ H/P – § There is proliferation of fibroblast and endothelial cells and formation of more tiny vascular channel, with infiltration of chronic inflammatory cells. § The lesion is consist of macrophages , lymphocytes and plasma cells. § Many of plasma cells contain eosinophilic globules of gamma globulin( Russell bodies). § Macrophages are the hallmark of granulation tissue

§ Large number of phagocytes will ingest lipid material and become collected in groups , called as foam cells. § Deposits of cholesterol as well as hemosiderin present. § Multinucleated giant cell of foreign body type also seen. § Also the presence of epithelial cells seen.

cholesterol crystals § Browne postulated that the main source of cholesterol was from disintegrating red blood cells in a form that readily crystallises in the tissues. § Cholesterol from this source and also from serum accumulates in the tissues because of the relative inaccessibility of normal lymphatic drainage.
 suggested that accumulation of cholesterol could occur through degeneration")
§ Trott et al. (1973) suggested that accumulation of cholesterol could occur through degeneration and disintegration of lymphocytes, plasma cells and macrophages taking part in the inflammatory process, with consequent release of cholesterol from their walls. § The possibility that circulating plasma lipids were a further source of cholesterol in cysts, as they were in atherosclerosis, must also be considered.

§ Bateriologic features. Strepooccus viridans , hemolyticus , nonhemolytic stretococci , Staphylococcus aureus , albus E. coli, are seen. § § § Treatment RCT Extraction of hopeless tooth.

§ § APICAL PERIODONTAL CYST RADICULAR CYST PERIAPICAL CYST ROOT END CYST

§ The apical periodontal cyst is the most common cyst. § It is a true cyst since the lesion consist of a pathological cavity that is lined by epithelium and often fluid filled. § The epithelium lining is derived from the epithelial rest of malassez which proliferate as a result of inflammatory stimulus in a preexisting granuloma.

§ Epithelium may be derived from – § Respiratory epithelium of the maxillary sinus when the periapical region communicates with the sinus wall. § Oral epithelium from fistula tract. § Oral epithelium proliferating apically from a periodontal pocket.

Pathogenesis Chapter 11. pdf

§ Pathogenesis § Periodontal cyst exhibit a lumen that is lined by stratified squamous epithelium, while the wall is made-up of condensed connective tissue. § Initial reaction leading to the cyst formation is a proliferation of epithelial rest in the periapical area involved by a granuloma. § Proliferation of epithelium is induced by keratinocytes growth factors elaborated by peiodontal stroma cells or inflammatory stimulus.

§ Activated T cells in the periapical granulomas produce lymphokines that may act on the rest of malassez causing proliferation & altered differentiation leading to cyst formation. § This epithelial proliferation follows an irregular pattern of growth. § The cyst increases in its size by osmosis local fibrinolysis & continued epithelial proliferation.

EPITHELIAL PROLIFERATION MECHANISM OF CYST EXPANSION #1 EPITHELIAL PROLIFERATION • THE PROLIFERATION OF THE CYSTIC EPITHELIUM CAUSES EXPANSION OF CYST. • THE DIFFERENCE IN RATE OF PROLIFERATION IN DIFFERENT AREAS Ø CAUSES ‘MURAL’ FORMATION • THE INCREASED RATE OF PROLIFERATION IS INDICATED BY: Ø INCREASED MITOTIC INDEX OF BASAL CELLS. Ø INCREASED DNA CONTENT (PHOTOCYTOMETRY). Ø INCREASED MEAN MARKING INDEX OSMOLALITY OF CYSTIC FLUID #3. OSMOLALITY OF INTRACYSTIC FLUID • INCREASED IN OSMOLALITY OF CYSTIC FLUID GREATER THAN OSMOLALITY OF SERUM: - Ø RELEASE OF CERTAIN PRODUCTS BY DEGENERATING CELLS INTO THE CYSTIC FLUID. • THE PRESSURE INSIDE THE CYSTIC LUMEN PRODUCES A NET OUTWARD FORCE WHICH CAUSES CYST EXPANSION. • Factors contributing for increased osmolality: Ø HYALURONIC ACID. Ø CHONDROTIN-4 -SULPHATE. Ø HEPARIN SULPHATE. Ø GLUCOSAMINOGLYCANS (GAG) & PROTEOGLYCANS CONNECTIVE TISSUE #2 CONNECTIVE TISSUE • Passive expansion of the connective tissue (unlikely) • Active growth of the connective tissue wall. • Enzymatic degradation of the connective tissue Collagenase – PMN collagenase Lucin aminopeptidase(? ) #4 BONE RESORPTION Hormonal or local enzyme mediated. Cells responsible for resorption – osteoclasts. The space produced by the resorption is used by expanding cyst. The factors involved are: -Prostaglandins – C 2, E 3, 12, F 2 -- Leukotrienes – C 4, D 4 - Interleukns. BONE RESORPTION

§ § § C/f Condition is asymptomatic. Seen between the age of 20 -60 years. More in permanent dentition Involve teeth are maxillary anteriors. Mostly seen in non vital teeth , deep carious teeth. § It is a lesion that represents a chronic inflammatory process & develop over a long period of time.

§ Radiographically it is identical to granuloma or cyst may be of greater size than the granuloma. § Hp§ Epithelial lining is stratified squamous in type. § Epithelial thickness is uneven and show hyperplasia. § Actual rete peg formation sometimes occurs. § The epithelial lining many times is discontinuous. § Rushton body or hyaline body is present.
 are found in epithelial")
§ In approximately 10% of radicular cysts, hyaline Bodies(Rushton’s bodies) are found in epithelial linings § first described by Dewey in 1918 § The bodies measure up to about 0. 1 mm and are linear, straight or curved or of hairpin shape and sometimes they are concentrically laminated. § They are brittle and frequently fracture. Circular or polycyclic bodies are also seen with a clear outer layer surrounding a central granular body.
 believed that the hyaline bodies resembled, in appearance and the liability")
§ Rushton (1955) believed that the hyaline bodies resembled, in appearance and the liability to fracture, the keratinized secondary enamel cuticle of Gottlieb. § Special stains and histochemical studies (Shear, 1961 b) indicated that they contained cystine and the author suggested that they were of odontogenic epithelial origin and probably a form of keratin. § Wertheimer et al. (1962) and Wertheimer (1966) also found histochemical similarities to keratin but pointed out that the correspondence was not complete. They supported the view that the bodies were a secretory product of odontogenic epithelial cells formed in the same way as the secondary enamel cuticle.
 and Sedano and Gorlin (1968) believed that hyaline bodies")
§ Bouyssou and Guilhem (1965) and Sedano and Gorlin (1968) believed that hyaline bodies were of haematogenous origin, and were derived from thrombi in venules of the connective tissue that had become varicose and strangled by epithelial cuffs which encircled them, and that they reacted histochemically as haemoglobin.

§ Connective tissue composed of parallel bundle of collagen fibers that often appear compressed. § Variable number of fibroblasts small blood vessel also seen.

§ A characteristic feature is the almost universal occurrence of an inflammatory infiltrate in the connective tissue immediately adjacent to the epithelium. (lymphocytes , plasma cells admixed polymorph). § Dystrophic calcification & collection of cholesterol slits with associated multinucleated giant cells are seen. § Collection of lipid filled macrophages are present.

§ Content of cyst lumen are watery, straw colored, blood tinged fluid to semisolid material , with low concentration of protein , cholesterol. § Differential diagnosis Granuloma § Treatment § Curettage § RCT § Extraction of hopeless tooth.

§ OSTEOMYELITIS § It is usually defined as inflammation of bone & bone marrow contents , changes in calcified tissue are secondary to inflammation of soft tissue component of the bone.

Classification § According to intensitya. Acute b. Sub acute c. Chronic

§ According to nature of reaction. Suppurative 1. acute 2. chronic- specific 3. Chronic non-specific Sclerosing 1. Focal 2. Diffuse Garre’s Osteomyelitis

OSTEOMYLITIS Acute suppurative Hematological Chronic suppurative Local Suppurative Primary Abscess Granuloma Radiation Focal sclerosing Diffuse sclerosing Florid osseous dysplasia Sclerotic cemental masses Garre’s osteomyelitis secondary
 Acute form (suppurative or non suppurative) a) Focus contiguous factor")
§ Hudson classification a) Acute form (suppurative or non suppurative) a) Focus contiguous factor b) Trauma c) Odontogenic infection - Progressive factor - Haematogenous b) Chronic form a) Recurrent multifocal Developing skeleton b) Garre’s Osteomyelitis c) Proliferative periostitis d) Suppurative or Non- suppurative
 Treatment non proper systemic compromise - Refractive - Diffuse Osteomyelitis - Host parasitic")
c) Treatment non proper systemic compromise - Refractive - Diffuse Osteomyelitis - Host parasitic compromise

Staging of Osteomyelitis Stage I – Medullary OML – It involved medullary bone without Compact Bone Stage II – Superficial OML- Less than 2 cm of bony defect without involving cancellous bone Stage III - Localized OML – Less than 2 cm of bony defect does not involve cortices Stage IV -Diffuse OML - The defect is greater than 2 cm pathological fracture infection & non union of the fracture.

§ ACUTE SUPPURATIVE OSTEOMYELITIS § Acute suppurative osteomyelitis of the jaw is a serious sequela of periapical infection § That often result in a diffuse spread of infection throughout the medullary spaces, with subsequent necrosis of a variable amount of bone.
 § Fracture")
§ Causes – § Dental infection. ( periapical infection , granuloma ) § Fracture or surgery. § Polymicrobial infection. § Tuberculosis, syphilis, actinomycosis. § § C/FMay involve maxilla or mandible. In maxilla lesion will be localized In mandible lesion will be diffuse.

§ Seen at any age. § Also called as neonatal maxillitis of infants and young children. § This osteomyelitis of infants is of hematogenous. § Patient complaints of severe pain , trismus parasthesia of the lips. § Elevation of temp with regional

§ Teeth in the area of involvement are loose sore so that eating is difficult. § WBC count is raised. § Pus may exude from gingival margin. § Until periostitis develops , there is no swelling or reddening of the skin or mucosa. § Radiographically Individual trabeculae become fuzzy & indistinct , involved area shows ill-defined margins with moth eaten appearance.

§ Pathology – § Infection causes acute inflammation of the marrow tissue & the resultant inflammatory exudates spreads through the marrow spaces. § This lead to compression of blood vessel in the bone , leads to thrombosis & obstruction of the blood flow resulting in necrosis of the bone. § Liquefaction of the necrotic tissue , dead & dying inflammatory cells & bacteria form the pus , & this may fill the marrow spaces.

§ This suppurative reaction extend through the cortical bone to involve the periosteum causing lifting of the periosteum, which further leads to compromise in the blood supply to the underlying bone resulting in further necrosis. § By osteolytic activity the necrozed bone known as sequestrum, is separated from the surrounding vital bone & exfoliate through the sinus.

§ H/P § The medullary spaces are filled with inflammatory exudates. § Inflammatory cells are neutrophils , plasma cells , lymphocytes. § Increased osteoclastic resorption &reduced osteoblastic activity in bony trabeculae. § T/t. Antibiotics Drainage Sequestrectomy.

§ CHRONIC SUPPURATIVE OSTEOMYELITIS § It may develop in inadequately treated acute osteomyelitis or may arise from a dental infection without a preceding acute stage. § Rarely may occur as a complication of radiation therapy. § Compare to acute osteomyelitis all sign & symptoms are milder.

§ Acute exacerbations of the chronic stage may occur periodically & these present all features of acute suppurative osteomyelitis. § The suppuration may perforate the bone & overlying skin or mucosa to form a fistula tract & empty on the surface.

§ § C/F – Mandible molar area > maxilla Pain with variable intensity. Swelling of the jaw , loose teeth &sinus tract are seen. § Radiographically appear as radiolucent lesion which show focal zones of opacification. Lesion may be very extensive & margin are indistinct.

§ H/P § Sequestrum may be present as evidenced by both necrotic marrow & necrotic osteocytes. § Reversal lines reflects the waves of deposition & resorption of the bone. § Inflammatory cells are numerous in fibrous marrow & osteoclastic activity are more prominent.
 § It is")
§ CHRONIC FOCAL SCLEROSING OSTEOMYELITIS ( CONDENSING OSTEITIS , BONY SCAR) § It is an focal reaction of bone to infection ; a reaction to mild bacterial infection entering the bone through a carious tooth in persons who have the high degree of tissue resistance & tissue reactivity.

§ The tissue react to the infection by proliferation rather than destruction , since the infection act as a stimulus rather than an irritant. § C/f – § Most commonly seen in children & young adult. § Most commonly involved teeth are mandibular 1 st molar , which present a large carious lesion. § Asymptomatic condition, Mild pain associated with an infected pulp.

§ Radiographically a well circumscribed radiopaque mass of sclerotic bone surrounding may have lucency at the apex of one or both roots. § PDL space is widened.

§ H/P- Dense mass of bony trabeculae with little interstitial marrow tissue. -Osteocytic lacunae appear empty. -The bony trabeculae exhibit many reversal & resting lines giving pagetoid appearance. § T/t Antibiotics Drainage

§ CHRONIC DIFFUSE SCLEROSING OSTEOMYLITIS § It is a condition analogous to the focal form of the disease & represent a proliferative inflammatory reaction of the bone to a low grade infection. § Pathosis is grouped under three major categories§ Diffuse sclerosing osteomyelitis § Chronic tendoperiostitis § SAPHO syndrome

§ Diffuse sclerosing osteomyelitis § Mostly seen in middle aged black women. § It shows no clinical indication of its presence. § There is an acute exacerbation of the dormant chronic infection & results in vague pain , unpleasant taste & mild suppuration. § Radiographically a diffuse patchy , sclerosis of the bone with ill defined margins. § This radiopaque lesion may be extensive


§ H/P§ Lesion shows dense , irregular trabeculae of bone , which are bordered by an active layer of osteoblasts. § Focal area of osteoclastic activity are seen. § The bone show a pronounced mosaic pattern. § The soft tissue between the individual trabeculae is fibrous & shows proliferating fibroblast. § Small capillary as well as small focal collection lymphocytes & plasma cells. § Sclerotic mass are composed of dense bone , with reversal line.

§ § § T/t Antibiotics Decortication Low dose corticosteroid Hyperbaric oxygen therapy

Chronic tendoperiostitis § It represents a reactive hyperplasia of bone that is initiated & exacerbated by chronic overuse of the masticatory muscle , parafunctional muscle habits.

§ § § C/F Mean age -40 yr No sex predilection. Recurrent pain , swelling of cheek , trismus. Suppuration are not found. Cultures are negative , with the lesions failing to respond appropriate antibiotics. § Sclerosis is limited to a single quadrant. § Relatively radiolucent zones are apparent within the areas of radiodensity , but histopathologic

§ Examination reveals only dense bone, formation of reactive bone , & relatively few signs of inflammation. § H/p – It shows sclerosis & remodeling of the cortical & subcortical bone with a resultant increase in blood volume. T/t – Muscular relaxation instruction Rotation exercise Occlusal therapy. MR drugs.

SAPHO syndrome § It is a complex clinical presentation includes— § Synovitis § Acne § Pustulosis § Hyperostosis § Osteitis Cause is unknown. It is thought to arise in genetically predisposed individuals who develop an autoimmune disturbances secondary to exposure to Dermatologic bacteria

C/F – Seen below the age of 60 yrs. Suffer from chronic multifocal osteomyelitis that is typically associated with negative microbiologic cultures& is non responsive to antibiotic therapy The osteolytic areas are scattered randomly within areas of sclerotic bone. Periosteal new bone formation is common not related to cortical bone perforation.

§ Involvement of multiple sites in anterior chest wall, sternum, clavicles, ribs. § In early gnathic lesions diffuse osteolytic zones are more prominent than sclerosis the affected bone is enlarged because of production of periosteal new bone. § External bone resorption & deformity of the are characteristic in older lesion.

§ H/p § It shows active bone remodeling rather than signs of infection , such as abscess formation & bone necrosis. § T/T – Anti-inflammatory drugs long term antibiotic therapy Decortication.

§ CHRONIC OSTEOMYELITIS WITH PROLIFERATIVE PERIOSTITIS § ( GARRES CHRONIC NONSUPPURATIVE SCLEROSING OSTEITIS , PERIOSTITIS OSSIFICANS )

§ It is a type of chronic osteomyelitis in which there is focal thickening of the periosteum with peripheral reactive bone formation resulting from mild irritation or infection. § C/f§ It is seen in young person before age of 25 yrs. § Most frequently involved the anterior surface of the tibia.

§ The condition in the jaw occur mainly in the posterior mandible in the children and young adult. § Most cases occur in the bicuspid & molar region. § The maxilla is seldom affected & the reason for this is not clear. § The patient usually complaint of § --a toothache or pain in the jaw. § -- a bony hard swelling of the outer surface of the jaw. § -- with normal appearing overlying skin or mucosa.

§ The reactive periostitis may develop not as a result of a central dental infection of jaw, that perforates outward but as a result of an overlying soft tissue infection or cellulitis, that subsequently involves the deeper periosteum. § Radiographically a carious tooth opposite the hard bony mass. § Focal overgrowth of bone on the outer surface of the cortex , which may be described as duplication of the cortical layer of bone. § Centrally mottled, expanded cortex with parallel opaque layers like onion skin

§ H/P – § Supracortical but subperiosteal mass is composed of much reactive new bone & osteoid tissue with osteoblasts bordering many of the trabeculae. § This trabeculae are oriented perpendicular to cortex & parallel to each other. § The connective tissue between the bony trabeculae is fibrous & shows a diffuse or patchy sprinkling of lymphocyte & plasma cells.

CHRONIC OSTEOMYELITIS Most infectious Variable Lucent or pain, drain mottled , swelling CHRONIC OSTEOMYELITIS with proliferative Sequela of tooth abscess, extraction Seen in lower molar (children) pulpitis asymptom Opaque mass treat atic at root apex offending tooth periostitis Diffuse sclerosing OSTEOMYELITIS Focal sclerosing OSTEOMYELITIS antibiotics Sequestre ctomy. Tooth removal antibiotics Lucent or mottled with concentric periosteal opacity Low grade pain, drain Opacification antibiotics infection, pulpit , swelling, through out is, periodontal In jaw diseases mandible

External root resorption § It is a lytic process occurring in the cementum or cementum & dentin of the roots of teeth. § Cause – Due to the peri radicular inflammation due to trauma , excessive force , cyst , central jaw tumors, replantation of teeth, systemic condition.

§ It is a asymptomatic condition. § When the root is completely resorbed the tooth become mobile. § If the external root resorption extend into the crown it will give the appearance of pink tooth. § Radiographically resorption appear as concave or ragged area on root surface or blunting of the root surface. § Area of replacement resorption or ankylosis have a resorb root with no Pdl space & with bone replacing the defect.

§ H/P – § It is the result of osteoclastic activity on the root surface of involve teeth. § Small area of cementum resorption replaced by connective tissue or repaired by new cementum , to large are of resorption replaced by osseous tissue to scooped out area of resorption replaced by inflammatory tissue. § T/t§ According to cause & amount of resorption

OTHER PERIRADICULAR DISEASES

§ In addition to the commonly encountered periapical granulomas and cysts of the jaws, there are many other lesions that may appear at the apices of teeth. § These other lesions, which range from nonodontogenic cysts to malignancies, must receive due consideration in the diagnosis of periapical disease because of their potential impact on patient treatment and outcome.

§ In distinguishing between periapical inflammatory disease and periapical neoplastic disease, a definitive diagnosis based on clinical and radiographic parameters can never be absolute because of the many overlapping signs and symptoms.

§ This makes differential diagnosis for a periapical lesion as important as it is for any other lesion of bone or soft tissue. Unless the clinician is thinking in broad rather than narrow terms, serious conditions may go undiagnosed and untreated for an inappropriate period of time.

Periapical Diseases Classified According to Biologic Behavior 1. Inflammatory § Periapical Granuloma and/or scar § Periapical cyst § Periapical Abscess § Actinomycosis § scar
 §")
2. Benign § Traumatic bone cyst § Nasopalatine duct cyst (incisive canal cyst) § Langerhans cell disease § Adenomatoid odontogenic tumor* § Periapical cemento-osseous dysplasia* § Ossifying/cementifying fibroma* § Vascular malformation

3. Benign Aggressive § Odontogenic Keratocyst § Central giant cell granuloma § Myxoma § Ameloblastoma § Calcifying odontogenic cyst* § Calcifying epithelial odontogenic tumor* 4. Malignant § Metastatic disease § Lymphoma/leukemia § Multiple myeloma

Inflammatory periapical lesions

§ A periapical or dental granuloma represents a focus of granulation tissue and inflammatory cells that have replaced apical bone. § Occasionally, when there is cortical perforation by the inflammatory process, osteogenesis may not occur, and the lesion remains as a fibrous scar even in the presence of an adequate root canal filling. § Also, if there is open communication between the tooth apex and oral cavity (e. g. , through a carious lesion), the microaerophilic bacterium actinomyces, found in the oral flora, can colonize in the inflamed periapical tissues § This variation of periapical granuloma can result in an actinomycotic infection of the jaw.

§ Periapical Granuloma and/or scar § Periapical cyst § D/D done by clinical examinations, radiograph & by histopathological examination, mostly non -vital tooth § Periapical Abscess § Actinomycosis § scar § In actinomycosis there is external sinus with sulpher granuels § In scar pt gives previous history of dental tt

Benign & benign aggressive lesions § A periapical cyst can be defined simply as a pathologic space lined by epithelium at the apex of a nonvital tooth. § The epithelial proliferation can be regarded as a defense mechanism that protects surrounding bone from the irritants of the necrotic dental pulp. § It is generally agreed that once a periapical granuloma becomes well-epithelialized, complete bony healing is unlikely with root canal therapy alone.

§ Whether a partially epithelialized periapical granuloma can heal following root canal therapy is still unknown. § Probably most of the endodontically treated teeth in which the periapical lesions persist (approximately 10 percent to 20 percent of cases) will be related to cystic change of a periapical granuloma.

§ Traumatic bone cyst § Nasopalatine duct cyst § Langerhans cell disease § Mostly teenagers, sometimes H/o trauma § Symmetrical swelling in midpalate, radiograph § Mainly in children, many bones are involved, loosening of teeth in area affected, gingival tissue often inflamed, submucosal nodule/ ulcers

§ Adenomatoid odontogenic tumor* § Periapical cementoosseous dysplasia* § In teenager, ant. jaw, females, crown of impacted tooth § Vital teeth, anti. mandible no symptoms, middle age § Ossifying/cementifyin g fibroma* § 3 -4 th decay, more in mandible, well circumscribed, continuous growth § Vascular malformation § Abnormal bl. Vessel development, poorly circumscribed, may affect bone, may produce bruit, grow with pt.

§ Central giant cell granuloma § May associated with basal nevoid syndrome, aggrasive, 2 -3 decay, mand > max, posterior § F>M, <30 yr, mand > max, anterior region § Myxoma § 10 -30 yrs, mand=max § Odontogenic Keratocyst

§ Adult, mandi. molar region, asymptomatic, tooth movement or malocclusion § No distinctive age, § Calcifying gender or odontogenic cyst* location, mainly in maxilla § Calcifying epithelial § 30 -40 yrs, mandibular posterior, peripheral odontogenic tumor* lesion, § Ameloblastoma

Malignant lesions of periradicular tissue - Paresthesia or atypical pain; - A lesion that appears to have no radiographic relationship to the apical periodontal ligament and lamina dura; - Large lesions and lesions with ill-defined margins; and - A lesion-associated tooth that is intact and of positive or equivocal vitality.

§ Metastatic disease § Lymphoma/leukemia § Multiple myeloma § Old age, mandibular posterior, bone pain, loose teeth, lip parasthesia, bone swelling, gingival mass § Bleeding, fatigue, in chronic leukemia lymphadenopathy, splenomegaly, boggy gingiva § >30 yrs, male, pain, swelling, anemia, bleeding, punched out skeletal lesions

§ § § § § References Ten Cate’s Oral Histology-6 th edition Berkovitz 3 rd edition Orbans oral histology Oral and Maxillofacial Pathology-II Edition. Neville Oral Pathology-Clinical Pathologic Correlation. Regezi Oral Pathology-Shafers Thoma 3 rd edition Text book of oral &maxillofacial surgery Nilima Malik. Endodontic practice 11 th edition Grossman

§ How Subodontoblastic capillary exchange occurs § Diffusion of O 2 and CO 2 between the blood and the pulpal cells is directly dependent upon the concentration gradient and inversely proportional to the diffusion distance.
 is determined by the Hydrostatic and Oncotic")
§ Fluid movement across SC (Subodontoblastic capillaries) is determined by the Hydrostatic and Oncotic pressures of blood vessels. § The total fluid reabsorbed by the venules and lymph equivalent to the fluid filtered from the blood

§ The human dental pulp plays a role in both tooth formation and maintenance. § Pulpal inflammation can occur from microbial, mechanical, or chemical irritants. § The pulp may be exposed to microorganisms suddenly due to trauma or more slowly by an advancing carious lesion. § The bacteria present in a carious lesion cause pulpal effects long before they physically invade the pulp proper. § Bacterial byproducts, diffusing through the dentinal tubules into the pulp, cause the local infiltration of chronic inflammatory cells.

§ As bacteria actually invade the pulp, pulpal inflammation becomes acute with polymorphonuclear leukocytes the dominant inflammatory cell. § Depending upon the severity of the pulpal insult, the pulp may exhibit a transient inflammation (reversible pulpitis). § The local response of the pulpal microvasculature allows the pulp to avoid self strangulation from the collapse of apical vessels. § If pulpal protective mechanisms are overwhelmed, a irreversible pulpitis will occur which will proceed to total necrosis. .

Pulpal pathophysiology
- Slides: 170