PULMONARY TUBERCULOSIS AISHA M SIDDIQUI PULMONARY TB n

PULMONARY TUBERCULOSIS AISHA M SIDDIQUI

PULMONARY TB n n n FACTS HISTORY DEFINITION EPIDEMIOLOGY PATHOLOGY CLINICAL FEATURES DIAGNOSIS COMPLICATIONS PREVENTION CHEMOTHERAPY REFERNCES

FACTS “If you know TB, you know medicine” Sir William Osler. n 1/3 world population is infected. n 8, 000 die/day, 2 -3 million/year. >AIDS& malaria. n Accounts for 1/3 AIDS deathes. n HIV patients 30 times more likely to get sick with TB once infected. n

HISTORY n n n n 1882 Robert Koch identified the tubercle bacillus. 1895 “Roentgen” x-rays. 1921 BCG vaccine (France). 1940 PPD (USA). 1944 Streptomycin. 1946 PAS. 1952 INH. 1966 Rifampicin.
 Do Nothing Era. n Sanatorium Era. n Collapse therapy. n Chemotherapy")
HISTORY (cont. ) Do Nothing Era. n Sanatorium Era. n Collapse therapy. n Chemotherapy Era. n Drug resistance. n

Definition Acid fast, aerobic bacilli: Mycobacterium. Tuberculosis. n Granuloma, central caseation, Langhan’s giant cells. n
 Extremes of age. n Contacts with open TB. n Over crowded populations.")
EPIDEMIOLOGY(HIGH RISK) Extremes of age. n Contacts with open TB. n Over crowded populations. n Health workers. n Low immunity. n

PATHOLOGY PRIMARY INFECTION: Primary complex. P. M. N+ macrophages->>> T- cells->>> increase cell mediated immunity (3 -8/52)->>> +PPD. Caseating granuloma, Langhan’s giant cells, lymphocytes & fibrosis------ healing &calcification. 20% contain remaining bacilli, activate if low immunity( decr host defences) POST PRIMARY T. B.

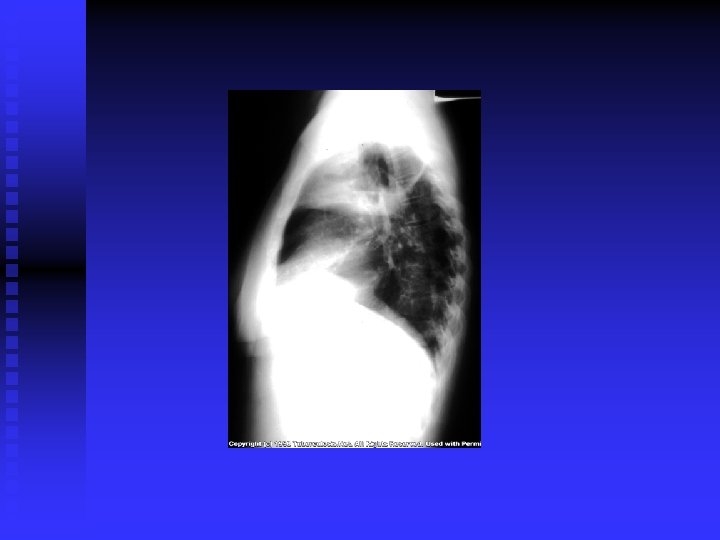
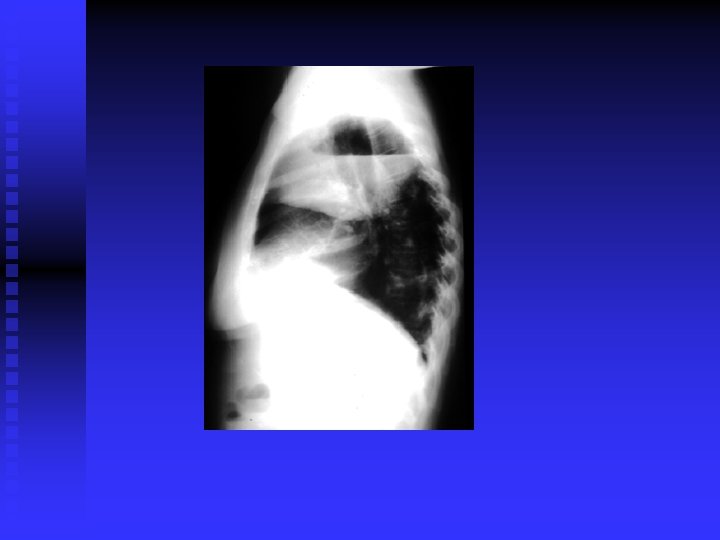
CLINICAL FEATURES Prim TB: Symptomless usually. n Miliary TB: Acute, diffuse, disseminated by blood. Old people. Difficult diagnosis. Fatal if not treated. Ill health, decrease wt. , fever. (gradual)>>> meningitis, hepatosplenomegaly, choroidal tubercles. CXR miliary, may be normal. PPD+/Transbronchial biopsy. CT scan. Liver & bone marrow biopsy& culture. n
 Post primary TB: Vague ill health, fever, decr. Wt. , sweating,")
CLINICAL FEATURES (cont’d) Post primary TB: Vague ill health, fever, decr. Wt. , sweating, cough, haemoptysis. Pneumonia/ pleural effusion. Abnormal CXR. CBC, sputum, biopsy. n
 FLUORESCENT 50% sensitivity. NAA")
DIAGNOSIS CXR / CT. n PPD? n Sputum: AFB( Z-N) FLUORESCENT 50% sensitivity. NAA (DNA/ RNA), 6 hours, expensive, other specimens also. . Culture: LJ BACTEC 7 -10 days NIACIN test ++ • Biopsy • Bronchoscopy / Lavage n
 CBC n U/E n ESR n LFT n")
INVESTIGATIONS (other) CBC n U/E n ESR n LFT n

COMPLICATIONS Extrapulmonary n Adrenal n SIADH n

PREVENTION BCG 70% immunity n Contact tracing n INH n

CHEMOTHERAPY Standard 6 -9/12 n Inexpensive 12/12 n Resistant n

Treatment Ethambutol>> n Pyrazinamide>> n INH>>>>>> n Rifampicin >>>>>> n Pyridoxine>>>>>> n n STEROIDS? ? ? 2/12 6/12
 n Cheaper: * Streptomycin INH 2/12 daily then 2/wk…… 10/ * INH")
TREATMENT (cont’d) n Cheaper: * Streptomycin INH 2/12 daily then 2/wk…… 10/ * INH 300 Thiacetazone 150 12/12 daily.
 n Resistant: PAS 15 gms 12 hrly PO Ethionamide 0. 75 -1 gm")
TREATMENT(cont’d) n Resistant: PAS 15 gms 12 hrly PO Ethionamide 0. 75 -1 gm PO Capreomycin 0. 75 - 1 gm IM Cycloserine 0. 75 -1 gm PO Ciprofluxacin

NEW DOTS n ICL enzyme. n

REFERENCES Scientific American Medicine n Davidson’s Principles and practice of Medicine n WHO report on TB n










- Slides: 32