PULMONARY THROMBOEMBOLISM By Dr TANVEER AHMED ANSARI DEFINITION

PULMONARY THROMBOEMBOLISM By Dr TANVEER AHMED ANSARI

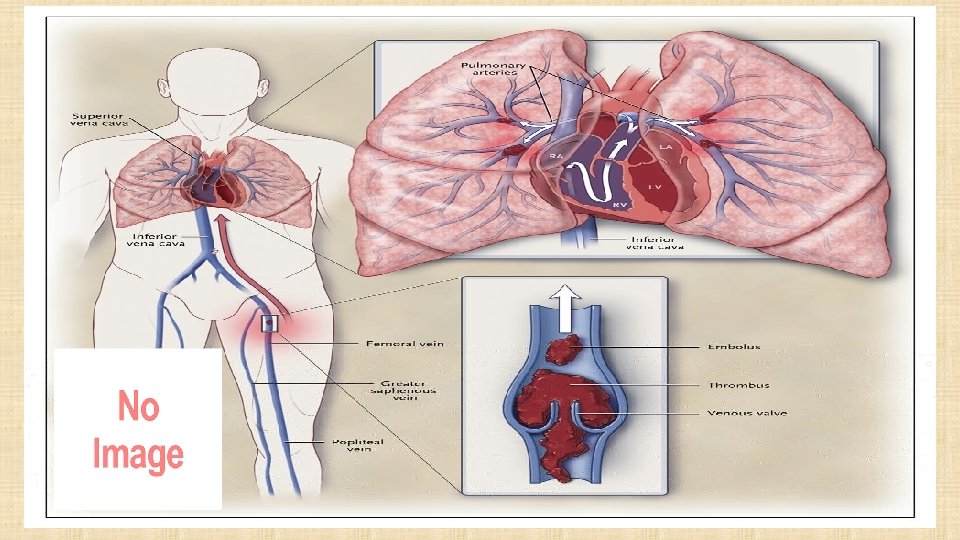
DEFINITION: • Pulmonary Embolism is the blockage of pulmonary arteries by thrombus, fat or air emboli and tumour tissue. • It is the most common complication in hospitalised patients. • An embolus is a clot or plug that is carried by the bloodstream from its point of origin to a smaller blood vessel.

Proportion with PE 65% 30 10%

VIRCHOW’S TRIAD • Venous stasis. • Injury or abnormalities to the vessel wall. • Alterations in coagulation properties.

VENOUS STASIS • Accumlation of activated procoagulants. – Immobilization – Inadequate peripheral pump. • Promotes thrombus formation.

VESSEL WALL INJURY • Acute or chronic injury to vessel endothelium. • Leads to activation of platelets and clotting cascade. • Promotes thrombus formation.

PLATELET ADHESION VESSEL INJURY AGGREGATION
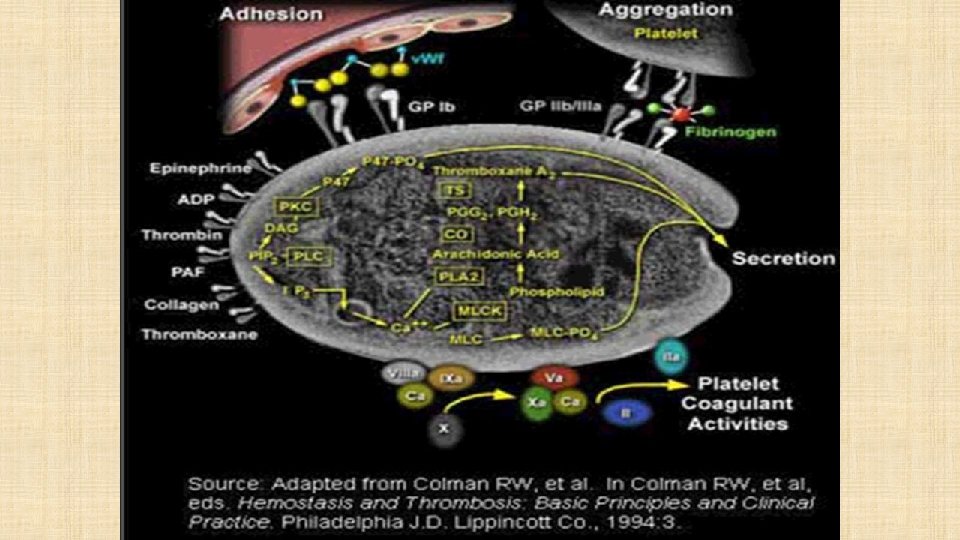

ALTERATIONS IN COAGULATION • Increase in procoagulant factors. – By trauma to vascular wall or extravascular tissues. – Releases tissue thromboplastin and phospholipid. – Leads to formation of prothrombin activator. – Prothrombin Thrombin • Decrease in anticoagulant factors. – Thrombomodulin – Antithrombin III – Alpha 2 -Macroglobulin – Plasmin PROTIEN C AND S DEFIENCY, FACTOR V LEIDEN Leads to hypercoagulable state by formation of thrombin.

CLINICAL SYMPTOMS • TACHYCARDIA ↑HR • TACHYOPNEA ↑ RR • HAEMOPTYPSIS – LUNG INFARCT • PULMONARY HTN SIGNS • ↑LFTs , ↑P 2 , RV dysfunction

CLINICAL SIGNS • Pleuritic chest pain and haemoptysis are late presentation indicating a pulmonary infarct. • A syncope without any other obvious signs- CAN be a massive PE. • Signs of RV dysfunction- like raised jugular venous pressure, parasternal heave and loud P 2. • Massive PE- hypotension, pale mottled skin and peripheral or even central cyanosis.

DIAGNOSIS

CHEST X-RAY −MORE IMPORTANT FOR ALTERNATE DIAGNOSIS.

S 1 Q 3� 3 AND T WAVE CHANGES

ECG: Less sensitive but more specific. P PULMONALE Important to rule out other diagnosis- eg: MI

DIAGNOSIS • D-Dimer – BIPRODUCT of Fibrin degradation product – ELISA tests are highly sensitive (>95%) – Non specific (~40%): cancer, sepsis, inflammation increase d-dimer levels • To rule out- rather than rule in. – Negative result excludes PE safely in PE-unlikely patients (using Clinical probability scores)

ULTRASOUND & DOPPLER– LOWER EXTREMITIES

USG Important when CT contraindicated. • Compression USG scan of deep veins. • 90% of thrombus originate from DVT. • If completely below knee- unlikely to cause PE.

2 D ECHO – TO KNOW THE SEVERITY RVH PAH TR TRICUSPID JET – VERY HIGH

2 D ECHO • Especially important in critically ill patient. • Most commonly as- RV dilation, RV hypokinesia, , paradoxical interventricular septal motion towards LV, TR. • RV hypokinesia with apical sparing is pathognomic of PTE.

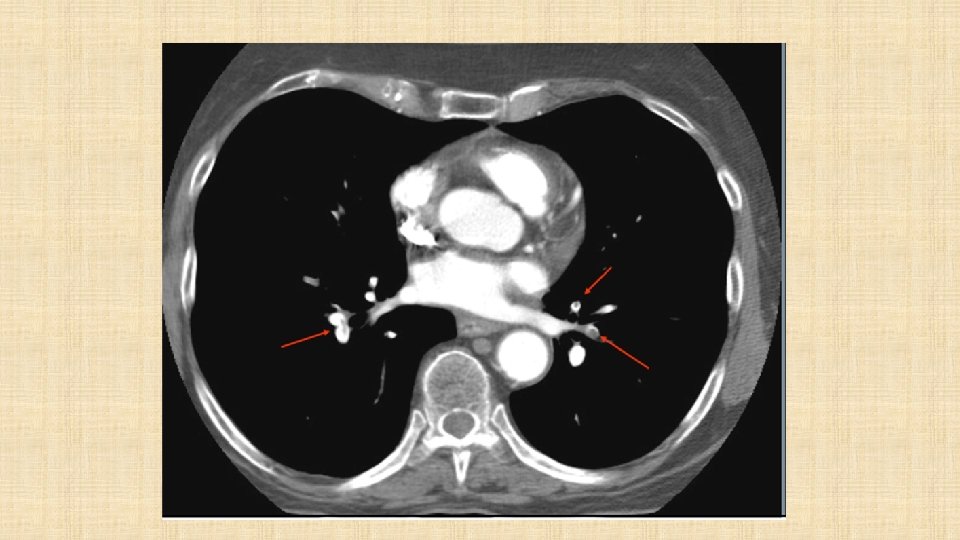
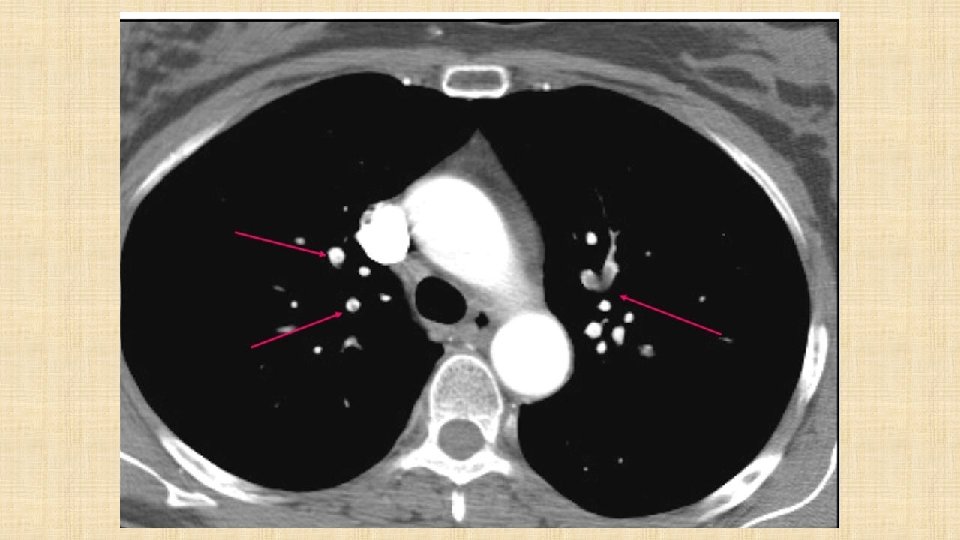
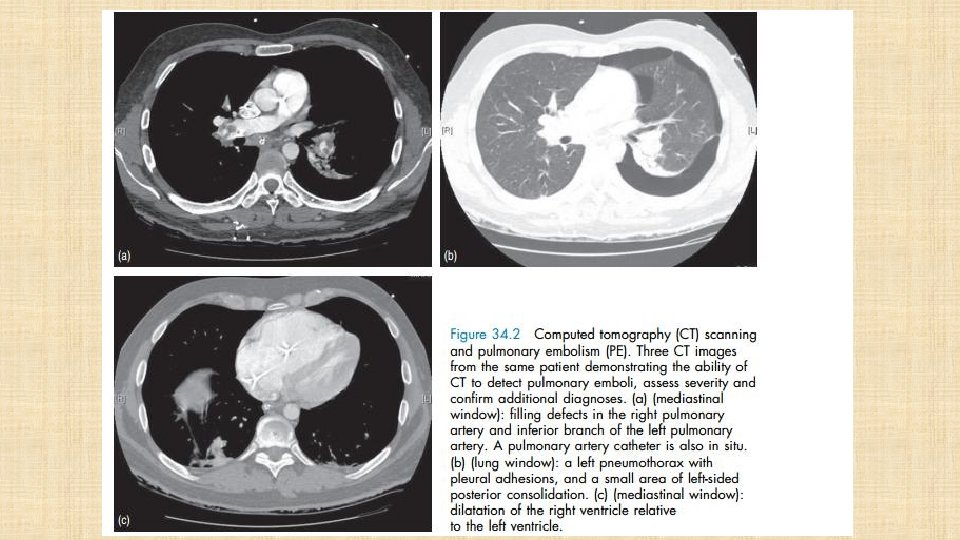
SPIRAL CT • Direct visualization of emboli. • Both parenchymal and mediastinal structures can be evaluated. • Offers differential diagnosis in 2/3 of cases with a negative scan. BUT… • Dye load and large radiation dose • Optimally used when incorporated into a validated diagnostic decision tree
 1. 3% This algorithm allowed")
3 month VTE rate 0. 5% (all non fatal) 1. 3% This algorithm allowed for a management decision in 98% of patients presenting with symptoms suggestive of PE

ADVANCED DIAGNOSTICS • Pulmonary scintigraphy • Pulmonary angiography. PULMONARY SCINTIGRAPHY • Noninvasive • Aids in diagnosis of PTE but not definitive. • Two types- ventilation and perfusion scans.

PERFUSION SCAN • Performed first. • Normal study VENTILATION/PERFUSI ON COMBO • With PTE the ventilation scan would be normal and the perfusion scan abnormal. rules out PTE. • Radionuclide- labelled, macroaggregated albumin in peripheral vein. • Suggestive of PTE. F • Picture from WWW. bschsys. org/Diagnositc. Imagi ng/nucmd/htm

NORMAL HUMAN PERFUSION SCAN ABNORMAL HUMAN PERFUSION SCAN

PULMONARY ANGIOGRAPHY-”GOLD STANDARD” • Performed if definitive diagnosis or exclusion of PTE is required. • Requires sedation or general anesthesia. • Greater risks. • Intraluminal filling defect and sharp cutoff are diagnostic for PTE. • Arrow indicates abrupt termination of a pulmonary artery.

DIAGNOSIS- SUMMARY In haemodynamic stable patient: CTPA- If clots present- confirms diagnosis To perform 2 D-echo for---raised RV/LV ratio, clot in proximal arteries, raised troponin, BNP, NT-pro-BNP. if CTPA contraindicated V/Q scan , MRA, USG. Negative does not rule out PTE, but if patient stable, even without anticoagulation, outcomes wont be poor. In haemodynamically unstable patient: Echocardiography is of prime importance- transeosophageal more preferable. If dilated RV with thrombus visualized- confirmed. If negative- The search for alternate diagnosis is priority before working up further for PTE. If echocardiograph not available- CTPA to be done clinically judging the feasibility.

TREATMENT AND MONITORING • Oxygen therapy. • HEPARINISATION • Streptokinase or TPA. • Mechanical ventilation. • Long term- warfarin therapy. • Clotting times- want to maintain PTT at 1. 5 -2. 5 times normal or and ACT at 1. 2 -1. 4 times normal. • Serial arterial blood gas analysis. • Respiratory rate. • Central venous pressure. • All other basic monitoring.

TREATMENT ANTICOAGULATION • HEPARIN PRODUCTS • 80 U/KG IV BOLUS • 18 U/KG IV ON FLOW • PTT 60 -90 • ↑HITS ↑CLOTS IF OCCURS STOP ALL HEPARIN PRODUCTS • ENOXAPARIN • 1 MG/KG Q 12 H IF GFR>30 • IF LESS THAT Q 24 H • ↓↓HITS Xa inhibitors(PO) DABIGATRAN, RIVAROXABAN, APIXABAN (LESS CHANCES OF BLEEDING), OR EDOXABAN OVER VITAMIN K ANTAGONIST (VKA) THERAPY.

CONTRA-INDICATIONS TO THROMBOLYSIS Absolute contraindications: • include any prior intracranial hemorrhage known structural intracranial cerebrovascular disease (eg, arteriovenous malformation) • known malignant intracranial neoplasm RELATIVE CONTRAINDICATIONS: • ischemic stroke within 3 months • age >75 years • suspected aortic dissection • current use of anticoagulation • active bleeding or bleeding diathesis • Pregnancy or within 1 week post partum recent significant closed-head or facial trauma with • Non compressible vascular radiographic evidence of bony fracture or brain injury within punctures last 3 weeks. • traumatic or prolonged Recent G. I bleeding within last 1 month. cardiopulmonary resuscitation severe uncontrolled hypertension on presentation (systolic blood pressure >180 mm Hg or diastolic blood pressure >110 (>10 minutes) mm Hg) • history of chronic, severe, and dementia and poorly controlled hypertension • recent surgery encroaching on the spinal canal or brain. • • • major surgery within 3 weeks

MASSIVE PTE: - PTE WITH HAEMODYNAMIC INSTABILITY AND RV DYSFUNCTION SUB-MASSIVE PTE: - PTE WITH AEMODYNAMIC STABILITY BUT RV DYSFUNCTION MILD PTE: PTE WITHOUT RV DYSFUNCTION AND HAEMODYNAMICALLY STABLE.

IVC FILTERS • May provide lifelong protection against PE • Unclear effect on overall survival • Complications: • DVT (20%) • Post thrombotic syndrome (40%) • IVC thrombosis (30%) • Risk/benefit ratio difficult to determine since no RCT • Use when there absolute contraindications to anticoagulation and a high risk of VTE recurrence • Consider in pregnant women with extensive thrombosis • Optimal duration of retrievable filters is unclear

U O • Y K N A TH
- Slides: 43