Pulmonary Thrombo Embolism Medium sized pulmonary arterty HE


Pulmonary Thrombo. Embolism
 Rt main pulumonary artery")
Medium sized pulmonary arterty (HE stain) Rt main pulumonary artery

Incidence VTE related death in USA : 300, 000/year 7% diagnosed with VTE and treated 34% sudden fatal PE 59% undetectable PE DVT 의 40% 에서 PTE (scan) PTE 의 29% 에서 DVT (US)

Pathophysiology 1. Increased pulmonary vascular resistance : Pulm a. obst. , vasoactive agent by PLT(serotonin) 2. Impaired gas exchange : increase alveolar dead space 3. Alveolar hyperventilation : stimulation of irritant receptor 4. Increased airway resistance : constriction of distal airway 5. Decreased pulmonary compliance : lung edema, hemorrhage, loss of surfactant

Pathophysiology RV dysfunction : usual cause of death pulmonary vascular resistant 증가 RV all tension 상승 RV dilatation & dysfunction diastolic LV impairment Rt coronary a. 압박 underfilling of LV subendocardial perfusion 감소 cardiac output & BP 감소 myocardial ischemia coronary a. perfusion 저하 RV infarction myocardial ischemia death

Mortality

Risk factor Predisposed to venous thrombosis 1. Local trauma to the vessel 2. Hypercoagulability 3. Stasis

Stressors precipitate PTE 1. Surgery, trauma 2. Obesity 3. Oral contraceptives, pregnancy, postpartum, postmenopausal HRT 4. Cancer (sometimes occult) or chemotherapy 5. Immobilization (stroke or ICU patients) 6. Indwelling central catheter

Diagnosis Sx and Signs in DVT 1. Cramp in lower calf : most frequent Sx - persists for several days - more uncomfortable as time progresses 2. mild palpation discomfort in lower calf

Diagnosis Sx and Signs in PE 1. Dyspnea : most frequent Sx 2. Tachypnea : most frequent sign 3. Massive PTE : dyspnea, syncope, hypotension, cyanosis 4. Pleuritic pain, cough, hemoptysis : small embolism located distally near pleura 5. Sometimes, a paradoxical bradycardia

Away from Dx of PTE 1. Absence of risk factor for DVT 2. Recurrent chest pain in same location 3. Pleuritic pain of more than 1 wk that increasing of severity 4. Pleuritic pain with negative finding on CXR 5. Hemoptysis of >5 ml with negative finding on CXR 6. Purulent sputum 7. Pericardial friction rub 8. Spiking fever >39 C lasting more than 1 wk

Differential Diagnosis DVT Ruptured Baker's cyst : sudden, severe calf discomfort Cellulitis : fever and chills Postphlebitic syndrome/venous insufficiency : diffusely edematous leg PE Pneumonia, asthma, chronic obstructive pulmonary disease Congestive heart failure Pericarditis Pleurisy: "viral syndrome, " costochondritis, musculoskeletal discomfort Rib fracture, pneumothorax Acute coronary syndrome Anxiety
,")
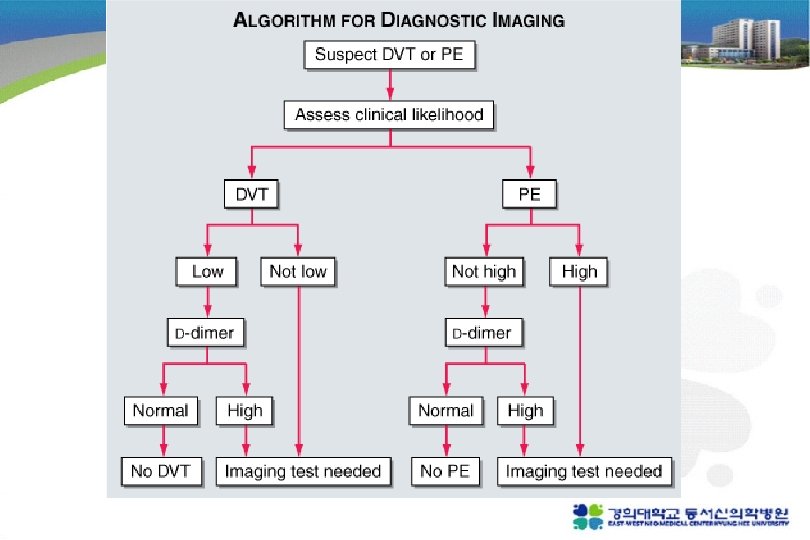
Nonimaging diagnostic modalities 1. Blood tests D-dimer ELISA : sensitive (DVT >80%, PE> 95%), not specific (MI, Pneumonia, sepsis, cancer, postop, preg) “rule-out test” 2. Elevated Cardiac biomarkers - major Complication and mortality Tn-I 증가 : RV microinfarction BNP or NT pro-BNP 증가 : myocardial stretch - predict an increase in major complication & mortality from PE

Nonimaging diagnostic modalities 3. Electrocardiogram : 임상적으로 큰 의미는 없다 sinus tachycardia S in I, Q in V 3, inverted T in V 3 (S 1 Q 3 T 3 sign) T inversion in V 4 -6 : most frequent

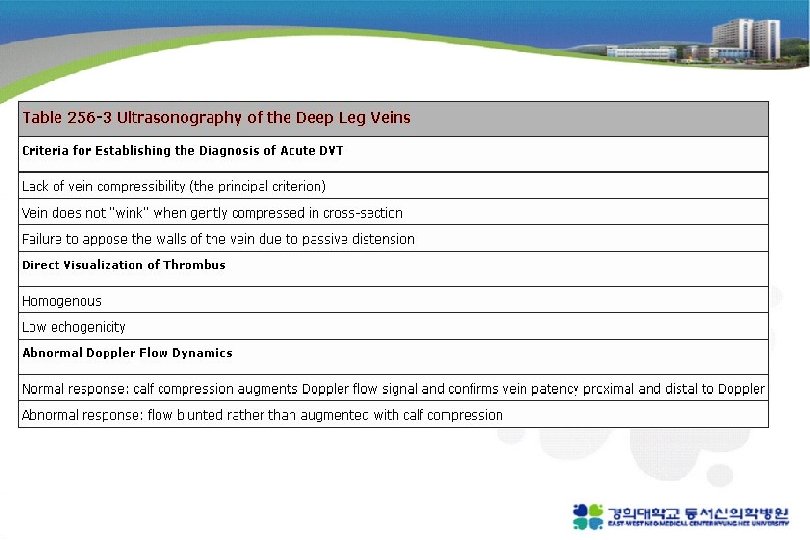
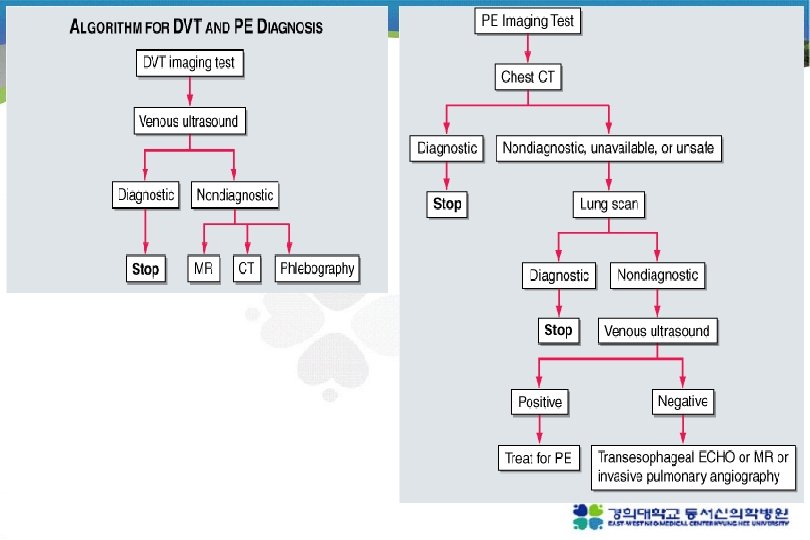
Noninvasive imaging modalities 1. Venous ultrasonography Confirmed DVT loss of “wink” sign 2. Chest reontgenography : normal or near normal Westermark’s sign (focal oligemia ) Hampton's hump (pph wedged-shaped density above diaphragm) Palla’s sign (enlarged Rt. descending pulmonary artery)
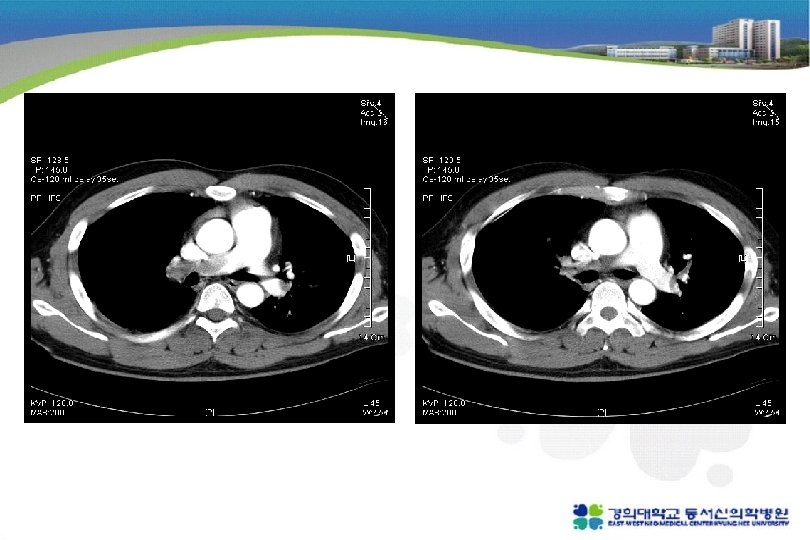
 principle imaging test for Dx. of PTE Multidetector-row spiral CT :")
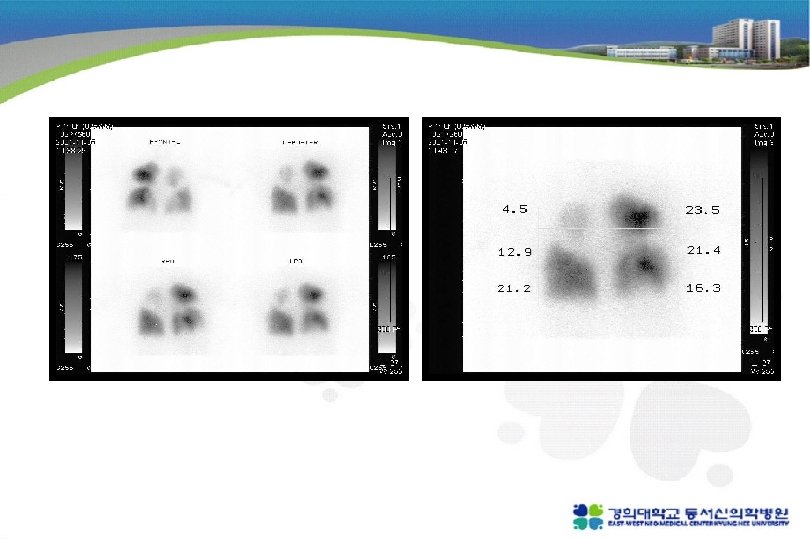
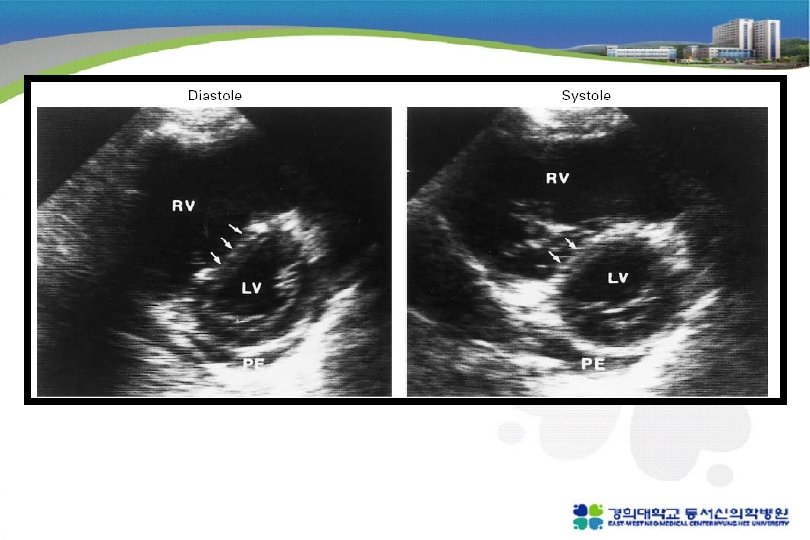
3. Chest CT(enhanced) principle imaging test for Dx. of PTE Multidetector-row spiral CT : small pph emboli RV enlargement : 사망률 5배 증가 다른 폐병변 감별가능 4. Lung scanning second-line test for PTE, 조영제 사용 못하는 환자 high probability : 두개 이상의 segmental perfusion defect 5. Echocardiography for DDx. (AMI, Tampomade, aortic dissection) detection of RV dysfunction
 Ascending aorta (2) Superior vena cava (3) Main pulmonary a. (4) Intravascular defects")
(1) Ascending aorta (2) Superior vena cava (3) Main pulmonary a. (4) Intravascular defects in Rt & left inferior pulmonary aa. (5) Descending thoracic aorta (7) Normal defect of the heart (6) Perfusion defects on scintigrams

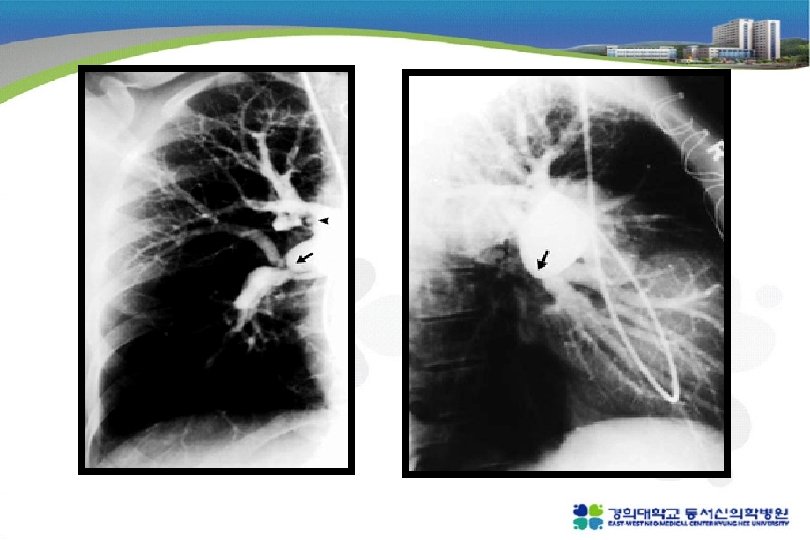
Invasive diagnostic modalities 1. Pulmonary angiograpy 진단 검사로는 chest CT 가 대체 CT 로 충분하지 않거나 intervention이 필요한 경우 시행 (catheter-directed thrombolysis or embolectomy) one projection 이상에서 filling defect abrupt occulusion(“cut-off”) of vessels, segmental oligemia or avascularity, prolonged arterial phase with slow filling, tortuous, tapering peripheral vessels 2. Contrast phlebograpy Venous ultrasonography 가 대체

Nonthrombotic pulmonary embolism 1. Fat embolism : after long bone Fx. , within 3 days unexplained dyspnea, tachypnea, hypoxemia - endothelial injury caused by fatty acid unexplained confusion or cerebral dysfunction sign - direct brain injury, hypoxemia petechiae over upper half of body - reason is not known Tx - supportive Px - mortality <10%

2. Cement and bony fragment embolism : after total hip or knee repacement 3. Amniotic fluid embolism : fetal membrane leak or tear at placental margin 다산부, supportive care 4. Tumor embolism 5. Air embolism

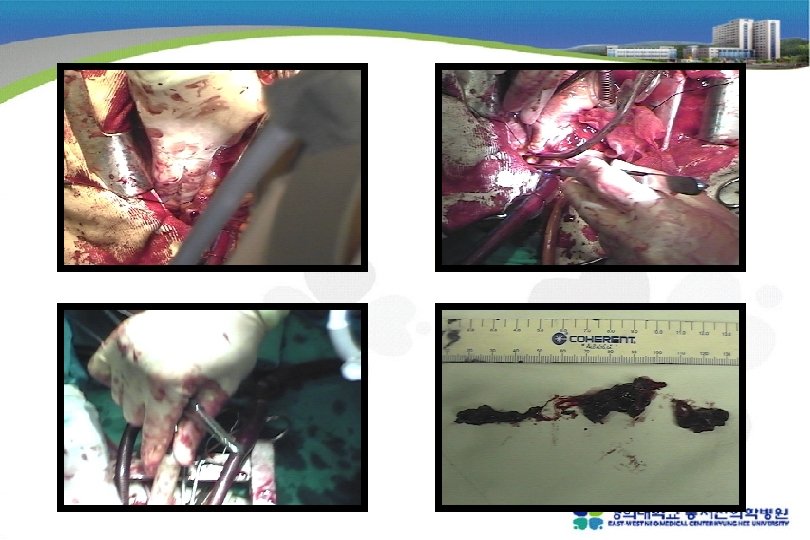
Treatment Primary therapy - high risk of death from Rt heart failure 1. thrombolysis : clot dissolution 2. embolectomy : removal of PTE Secondary prevention of recurrent PE anticoagulation with heparin and wafarin inferior vena caval filter

Risk stratify Normotension Plus normal RV Normotension Plus RV hypokinesis Hypotension Secondary prevention Individualize therapy Primary therapy Anticoagulation alone IVC filter Anticoagulation Plus thrombolysis Embolectomy: Catheter/surgical

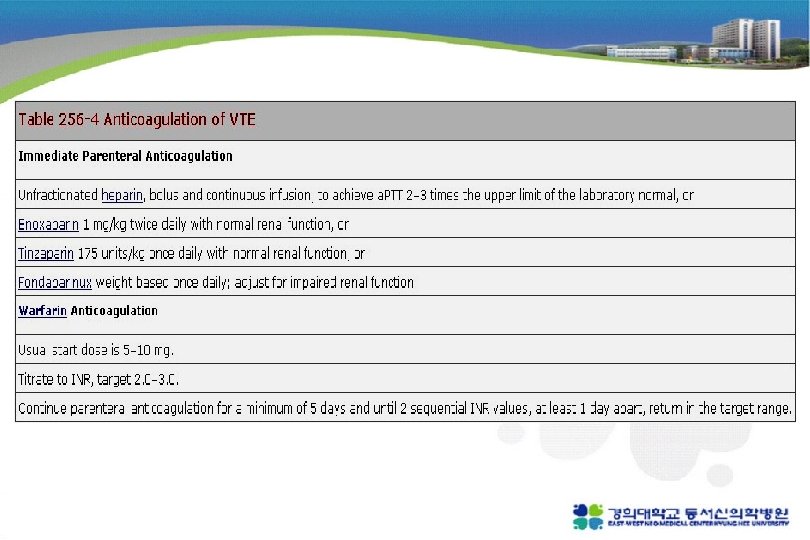
Heparin : 5000 -10000 u bolus 1000 -1500/hr infusion a. PTT는 적어도 2 -3 배 - bind to and accelerate activity of antithrombin III prevents additional thrombus formation permits endogenous fibrinolytic mech. to lyse clot - do not directly dissolve thrombus
 Advantage - short half-life anticoagulant effect abates after several hours - useful in")
1) Advantage - short half-life anticoagulant effect abates after several hours - useful in pt will undergo an invasive procedure (surgical embolectomy) 2) Disadvantage - achieving target a. PTT can be difficult - repeated blood sampling and dose adjustment every 4– 6 h - at risk of developing heparin-induced thrombocytopenia
 Complications - hemorrhage : most important antidote (protamine sulfate) : life threatening or")
3) Complications - hemorrhage : most important antidote (protamine sulfate) : life threatening or intracranial hemorrhage - thrombocytopenia : 50% 이하(<10만) 로 감소하면 stop - osteoporosis - pathologic bone fracture - heparin associated elevation in transaminase levels
 1) less bind to plasma proteins and endothelial cell")
LMWH (low molecular weight heparin) 1) less bind to plasma proteins and endothelial cell 2) greater bioavailability 3) more predictable dose response 4) longer half life 5) not need laboratory monitoring or dose adjustment - Enoxaparin 1 mg/kg bid, tinzaparin 175 units/kg once daily - must be adjusted downward in renal insufficiency
 anti-Xa pentasaccharide 2) administered by once-daily subcutaneous injection 3) no laboratory monitoring")
Fondaparinux 1) anti-Xa pentasaccharide 2) administered by once-daily subcutaneous injection 3) no laboratory monitoring is required 4) <50 kg receive 5 mg, 50– 100 kg receive 7. 5 mg >100 kg receive 10 mg 5) adjust for impaired renal function

Warfarin : initiated in a dose of 5 -10 mg, target INR 2. 5(2. 0 -3. 0) 1) vitamin K antagonist 2) prevents carboxylation activation of factors II, VII, IX, X 3) full effect of warfarin requires at least 5 days 4) Overlapping UFH, LMWH, fondaparinux for at least 5 days - monotherapy during an acute thrombotic illness paradoxical exacerbation of hypercoagulability increase likelihood of thrombosis rather than prevent it
 Complications - bleeding : antidote - Vitamin K, FFP, cryoprecipitate - warfarin induced")
5) Complications - bleeding : antidote - Vitamin K, FFP, cryoprecipitate - warfarin induced skin necrosis - warfarin embryopathy → should be avoided during pregnancy !! (출산 후나 수유 시는 가능)

Duration of Anticoagulation Complications PE following surgery or trauma : low rate of recurrence after 3– 6 months DVT isolated to an upper extremity or calf : by surgery or trauma, 3 months suffices provoked proximal leg DVT or PE : 6 months is sufficient "idiopathic, " unprovoked DVT or PE : recurrence rate is surprisingly high after cessation (VTE that occurs during long-haul air travel is unprovoked) indefinite duration with a target INR between 2. 0 and 3. 0
 active bleeding 2) recurrent venous thrombosis despite intensive anticoagulation")
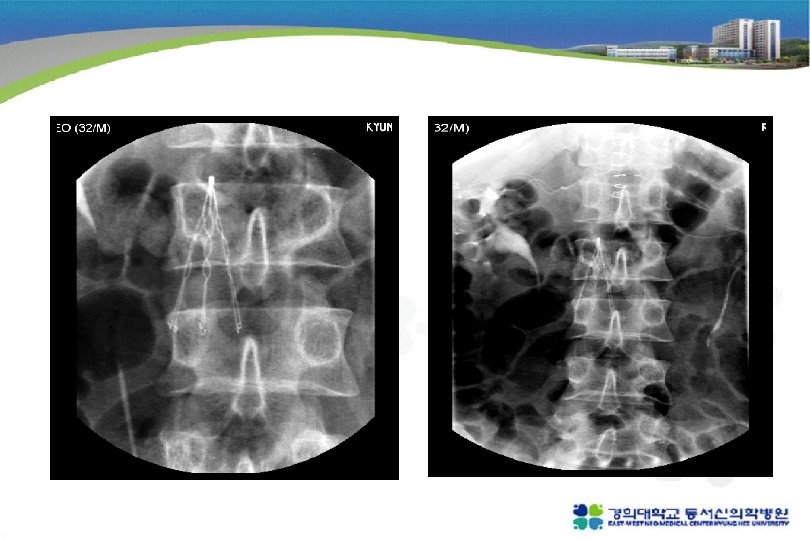
Inferior Vena Caval Filters 1) active bleeding 2) recurrent venous thrombosis despite intensive anticoagulation 3) prevention of recurrent PTE in Rt heart failure (not candidates for thrombolysis) 4) prophylaxis of extremely high risk patients - contraindication to anticoagulation - significant bleeding complications during anticoagulation

Thrombolysis - rapidly reverse Rt. heart failure and lead to lower rate of death and recurrence Indication : Angiographycally proven massive pulmonary embolism with hemodynamic instability Contraindication - Active or recent internal bleeding - Hx. of hemorrhagic stroke - Recent cranial surgery or head injury

Pulmonary Thromboembolectomy - massive pulmonary emboli with 1. Hypotension and end-organ dysfunction despite maximal medical support and 2. Absolute contraindication to thrombolytic therapy or full-dose thrombolytic therapy proved ineffective

Prevention of postphlebitic synrome vascular compression stockings - only therapy to prevent postphlebitic syndrome - daily use of below-knee 30 -40 mm. Hg - halve the rate of developing postphlebitic syndrome - should be prescribed as soon as DVT is diagnosed, should be fitted carefully

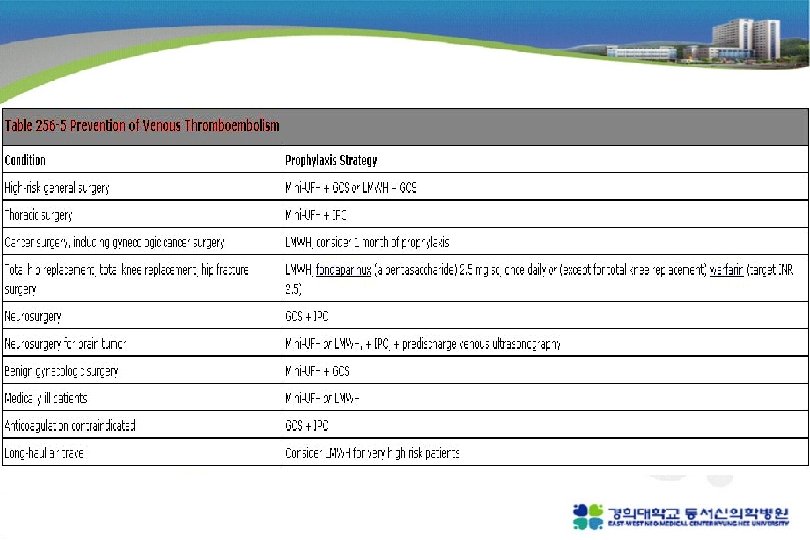
Prevention of VTE graduated compression stockings intermittent Pneumatic compression devices mini-dose unfractionated heparin (5000 u SC 2 or 3 daily) low molecular weight heparin (enoxaparin 40 mg once daily) Fondaparinux (2. 5 mg daily)
- Slides: 50