Pulmonary Rehabilitation in Rheumatic diseases BY Sally Saber

Pulmonary Rehabilitation in Rheumatic diseases BY: Sally Saber Abdelaziz Ass. lecturer of Physical medicine, Rheumatology and Rehabilitation Ain Shams University

Agenda ü The mechanisms by which lungs are affected in rheumatic diseases. ü What is pulmonary rehabilitation program? ü What are the goals and benefits of pulmonary rehabilitation ? ü What are the components of pulmonary rehabilitation and how it is done ?

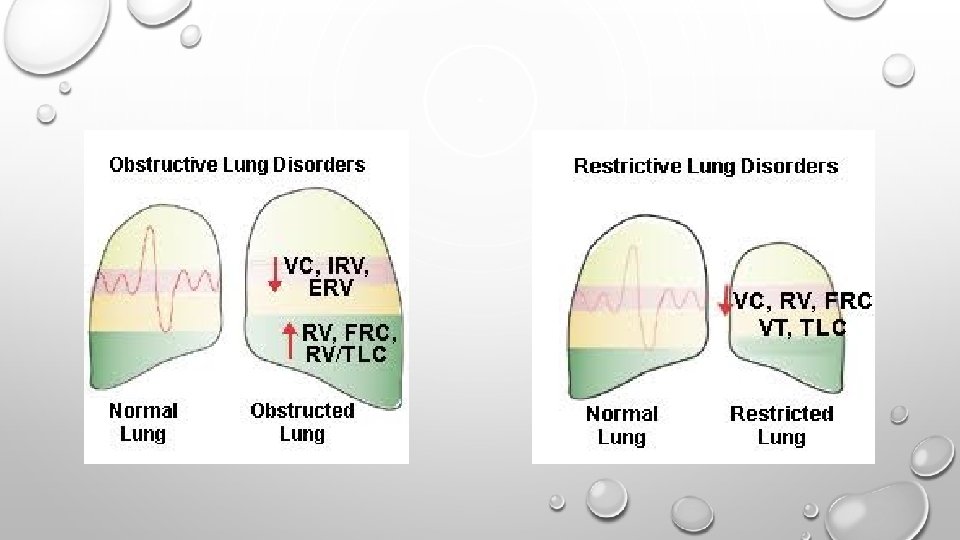
§ Original connective tissue disease affecting the lung. § Drug induced side effects. § secondary infections. § As a complication of the original disease.

Pulmonary manifestations of RA Pleural disease: pleurisy & pleural effusion. Nodules &Caplan syndrome. Interstitial lung disease (ILD) Organizing pneumonia (OP) Airways diseases: Bronchiectasis, emphysema & bronchiolitis obliterans (OB)

Pulmonary manifestations of SLE Pleural disease: pleuritis & pleural effusion. Acute lupus pneumonitis with or without Hge. Chronic Interstitial lung disease (ILD) Pulmonary hypertension. Rare complications: shrinking lung syndrome & cryptogenic organizing pneumonia Secondary infections.
 Interstitial lung disease (ILD) Polymyositis Interstitial lung disease (ILD)")
SSc Pulmonary artery hypertension (PAH) Interstitial lung disease (ILD) Polymyositis Interstitial lung disease (ILD) MCTD Pulmonary artery hypertension (PAH) Interstitial lung disease (ILD) AS Interstitial lung disease (ILD) and lung fibrosis.

e l c Breathing difficulty e h t k Disability r B a e Physical deconditionin g y c inactivity

What is pulmonary rehabilitation? • Pulmonary rehabilitation is a multi factorial program of education, counselling, exercises, breathing training, and other modalities that can increase the functional gain of the patient with greater ease and independence. • It is conducted by a team of specialists that may include ; a pulmonologist, a nurse, a physical therapist , a nutritionist, psychologist, speech & swallowing therapist and sometimes a neurologist. The physiatrist is the maestro of the team. • According to the patient condition, It takes place in a hospital or in an out patient rehabilitation center.

• Patient’s Oxygen level , heart rate and blood pressure must be monitored during the session. And in each visit the staff will ask the patient about symptoms and signs of Pulmonary distress and will review the progress. • Pulmonary rehabilitation typically runs 8 -12 weeks, two days a week for 60 to 90 minutes. • It is a tailored program. • Pulmonary rehabilitation is NOT a cure; nor can it slow the progression of the disease.

What are the benefits of pulmonary rehabilitation ? • Reduces the symptoms. • Improves exercise capacity and endurance. • Reduces hospitalization. • Improves survival. • Improves health related quality of life. • Reduces anxiety and depression. • Improves psychological wellbeing.

• All patients with lung problems are candidates for pulmonary rehabilitation. But, Smoking is a relative contraindication to start a rehabilitation program. • Smoking cessation program must be initiated before or simultaneously. • Many rehabilitation centers will not cover pulmonary rehabilitation program unless the patient stop smoking for at least three months.

Patient education Breathing training Componen ts of PR Exercise therapy Psychological support

Pre- rehabilitation assessment: § Full detailed medical history. § Functional assessment including: Active and passive ROM. Muscle power. Mobility assessment. § Gait analysis. § Special tests : Time up and go test. Six minute walk test. § Special scores: Modified Borg (dyspnea) scale. RPE (rating of perceived exertion) § Special investigations: Pulmonary function tests.

Time up and go test Purpose: To assess mobility Equipment: A stopwatch Directions: Patients wear their regular footwear and can use a walking aid, if needed. Begin by having the patient sit back in a standard arm chair and identify a line 3 meters. When I say “Go, ” I want you to: 1. Stand up from the chair. 2. Walk to the line on the floor at your normal pace. 3. Turn. 4. Walk back to the chair at your normal pace. 5. Sit down again. An older adult who takes ≥ 12 seconds to complete the TUG is at risk for falling.

six minute walk test • 30 meters straight flat path of walk. • Maximum of 6 minutes. • Dyspnea and fatigue are assessed before and after. AIM • • To determine the initial distance covered by the patient, for prognosis and to be compared after the CPR program. To estimate the intensity of exercise needed.

Modified Borg dyspnea scale Instructions § Use this scale to rate the difficulty of your breathing. § It starts at number 0 where your breathing is causing you no difficulty at all and progresses through to number 10 where your breathing difficulty is maximal. How much difficulty is your breathing causing you right now?

Rating of Perceived Exertion Scale After every exercise we ask the patient to give a score about the difficulty of the performed exercise.

I. Patient education covers many important points such as: • Smoking cessation • Medication and oxygen use. • Strategies for managing disease symptoms. • Weight reduction. • Nutritional status. • Life style modification. • The importance of the rehabilitation program.

II. Psychological § support Breathing difficulty leads to anxiety and fatigue. § Patient may suffer from depression and social deprivation. § So during the rehabilitation program, presence of psychologist or psychiatrist is very important that provides emotional support and stress reduction techniques § Group therapy helps the patient to counter act the feeling of being alone accompanied disabling illness. § Help patients to deal with their symptoms of the disease and stress. The approach must be tailored for each patient

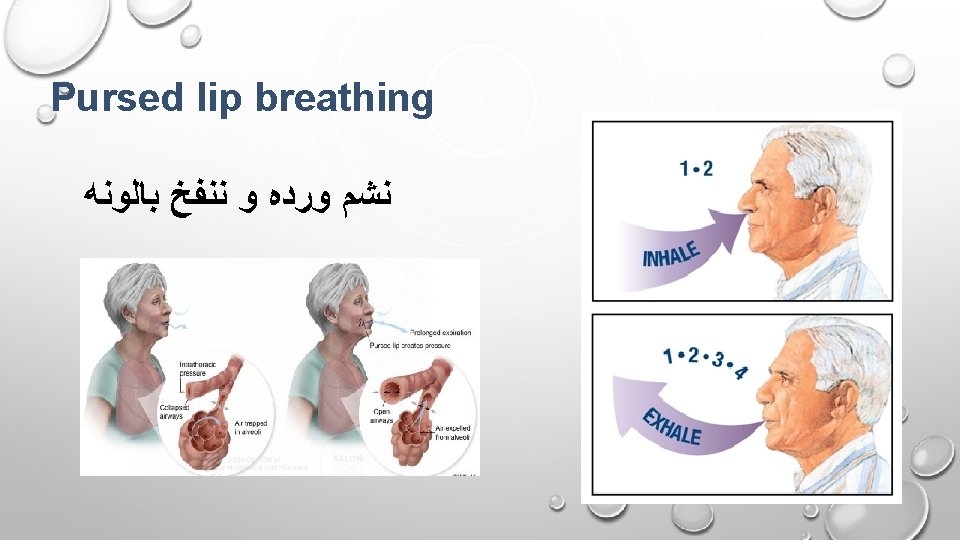
III. Breathing training § Patients with pulmonary illness breath rapid, shallow and short. § No enough time for gas exchange and transfer O 2 to body muscles. § Patient has to use accessory muscles and do excess effort to meet the demand. § Patient become distressed and avoids to do exercise. § Patient suffers from fatigue of respiratory and peripheral muscles. The corner stone in pulmonary rehabilitation is useful and effective breathing

Breathing training § Diaphragmatic breathing. § Pursed lip breathing. § Glossopharyngeal breathing. § Segmental breathing. a) Apical breathing b) Lateral costal breathing c) Posterior basal brathing

Diaphragmatic breathing Breath in deeply and breath out slowly. ﻧﺸﻢ ﻭﺭﺩﻩ ﻭ ﻧﻄﻔﻰ ﺷﻤﻌﻪ
 § Neuromuscular disorders. § GUP. § Increase the inspiratory capacity and")
Glossopharyngeal breathing (GPB) § Neuromuscular disorders. § GUP. § Increase the inspiratory capacity and also cough. § Start gradually 10 -15 in row then increase up to 30.

Segmental breathing

Incentive respirometer

Inspiratory muscle training § Damaged airways and lung tissue are NOT the only causes of difficult breathing for those patients. Another contributing factor is fatigued respiratory muscles. § The respiratory muscles become fatigued because they have to work harder when patient breath. § In addition, the diaphragm (the main inspiratory muscle) is less effective when it’s position is altered. Inspiratory muscle training aims to strengthen these muscles. It’s like weight lifting for breathing muscles.
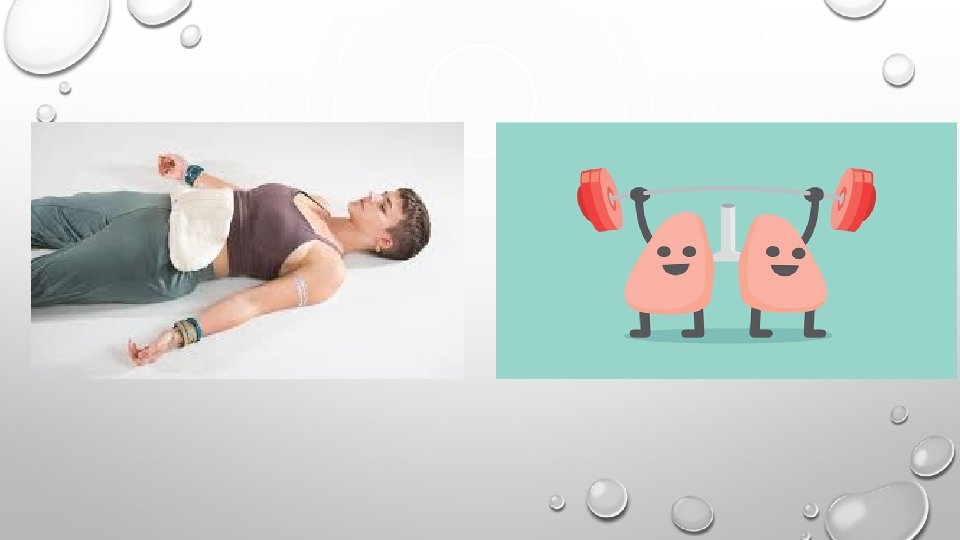

Inspiratory muscle training The device provides resistance to patient’s breathing efforts. Adding inspiratory muscle training improves strength and endurance more than exercise alone.

Air way clearing techniques Percussion and vibration. Contraindications


Postural drainage

Flutter
")
Oscillatory post expiratory pressure device (Acapella)

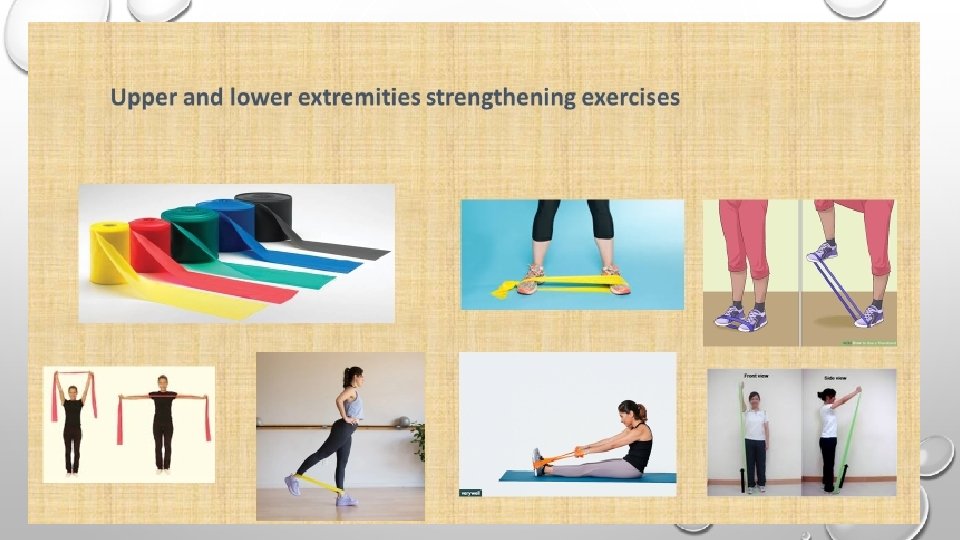
VI. Exercise therapy • Everyone in pulmonary rehabilitation gets aerobic exercise therapy under supervision of a health care professional. • The purpose of aerobic exercise is to increase endurance and strengthen peripheral muscles to lessen the symptoms and improve the tolerance for activity. • Exercise therapy is not standard for every patients but it is tailored according to patient condition. • It is ranged from bed exercises till outdoors activities. • During rehabilitation, sustained periods of intense exercise lasting 20 -45 minutes are usually executed, but some patients perform periods of exercise

• Start exercise very gradually. • Before starting exercise BP, HR, RR, O 2 sat must be measured. and during the exercise HR, O 2 sat must be monitored. • If the patient start to desaturated during the exercise , stop and rest the patient and then resume the exercise. • If O 2 saturation become 85% or HR more than 130 b/min. you have to stop the exercise immediately. • During any exercise, breathing exercise must be performed. • After every exercise, the patient is asked to rate the difficulty RPE.

In bed exercise:

Bicycling Upper extremity ergometer Upper and lower extremity biking Lower extremity biking

Stairs • Start gradually 10 steps for the right leg and then 10 to the left one. • On the coming visit increase 5 steps for each leg.

Leg Press • Start with 10 leg presses then increase gradually. • It is both strengthening and stretching to a highly important group of muscles.

Treadmill • Start by 10 minutes. • The first 2 minutes just walking on slow speed. • The following 2 minutes increase the inclination gradually with no increase in the speed. • Then ask the patient to do jogging for 2 minutes while it is on slow speed with no inclination. • The remaining 4 minutes just walking with slow speed.

Take home message: • Pulmonary rehabilitation is a multifactorial program. • Although it does not affect the ongoing disease, it has a very important role in the overall wellbeing of the patient. • It is not a standardized program but it is tailored for each patient according to it’s condition.

References: • Bohannon RW. Reference values for the Timed Up and Go Test: A Descriptive Meta-Analysis. Journal of Geriatric Physical Therapy, 2006; 29(2): 64 -8. • Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the timed up & go test. Phys Ther. 2000; 80: 896 -903. • Kristensen MT, Foss NB, Kehlet H. Timed "Up and Go" Test as a predictor of falls within 6 months after hip fracture surgery. Phys Ther. 2007. 87(1): 24 -30. • American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR) http: //www. aacvpr. org/Resources/Searchable. Program. Directory/tabid/113/Default. aspx https: //www. aacvpr. org/Resources-for-Patients/Pulmonary-Rehab-Patient-Resources • Vanfleteren, L. E. , Franssen, F. M. , Uszko-Lencer, N. H. , Spruit, M. A. , Celis, M. , Gorgels, A. P. et al. (2011) Frequency and relevance of ischemic electrocardiographic findings in patients with chronic obstructive pulmonary disease. Am J Cardiol 108: 1669– 1674

- Slides: 46