PULMONARY FUNCTION TESTS Dr Kalpana B Specific Learning

� PULMONARY FUNCTION TESTS Dr Kalpana. B

Specific Learning objectives • 1. 2. 3. At the end of class students should be able to: Explain a spirogram and various static and dynamic lung volumes and capacities Explain FRC alongwith experiments to measure it Differentiate between obstructive and restrictive lung diseases

FPulmonary function tests are useful in assessing the functional status of the respiratory system both in physiological and pathological conditions

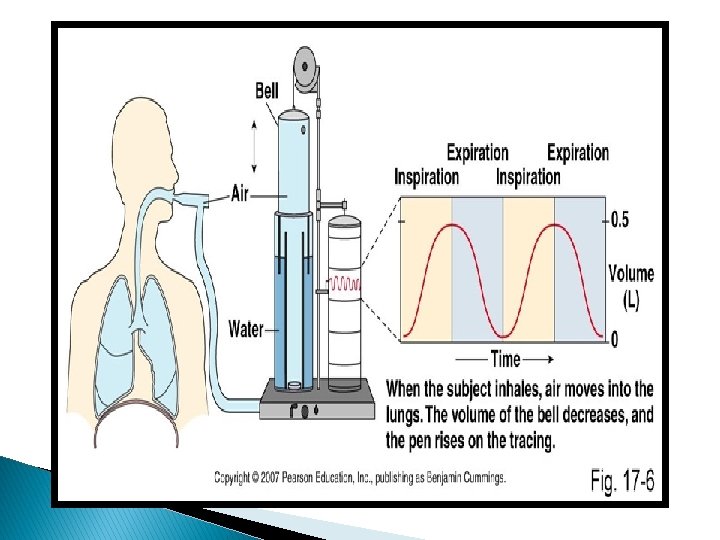
Lung Volumes – Volume of air breathed by an individual during the altered pattern of respiration Lung Capacities – Two or more lung volumes together Ø Method of study by – Spirometry Ø Apparatus used – Spirometer (Spirograph) Ø Record obtained -- Spirogram
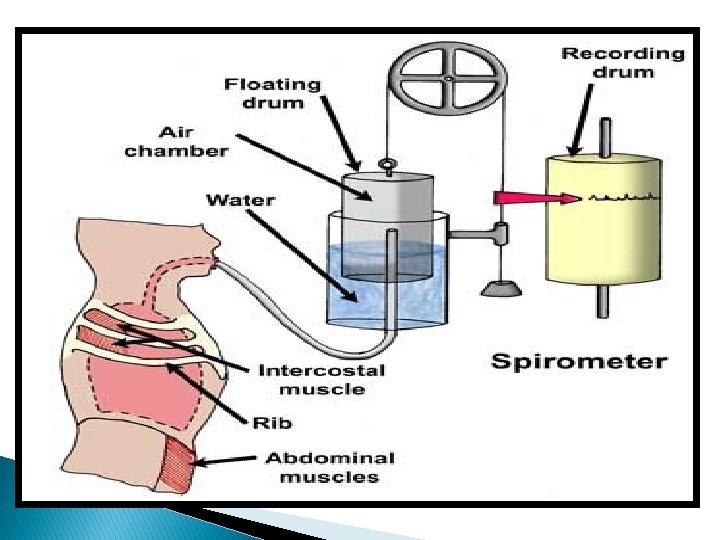

FSpirometer can be used only for single breath FRepeated cycles of respiration cannot be recorded

F Cause ØThe carbon dioxide accumulated in the spirometer cannot be removed ØOxygen or fresh air cannot be provided to the subject

All pulmonary volumes and capacities are about 20 to 25 percent less in women than in men. Greater in large and athletic people than in small and asthenic people.
 Inspiratory reserve volume (IRV) Expiratory reserve volume (ERV) Residual")
Lung Volumes Tidal volume (TV) Inspiratory reserve volume (IRV) Expiratory reserve volume (ERV) Residual volume (RV)
 – 500 ml Volume of air breathed in or out")
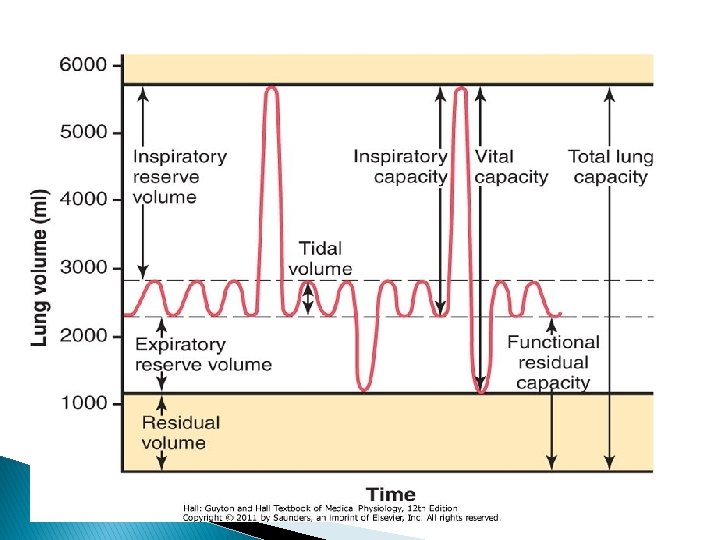
Tidal volume (TV) – 500 ml Volume of air breathed in or out of the lungs in a single normal quiet respiration. Inspiratory reserve volume (IRV) – 3300 ml It is the maximal volume of air which can be inspired after completing a normal tidal inspiration Expiratory reserve volume (ERV) – 1000 ml It is the maximal volume of air which an be expired after a normal tidal expiration
 – 1200 ml It is the volume of the gas")
Residual volume (RV) – 1200 ml It is the volume of the gas which remains in the lungs after maximal expiration 1. It helps to aerate the blood in between breathing and during expiration 2. It maintains the contour of lungs
 =IRV + TV =3800 ml It is the maximum")
Lung Capacities Inspiratory capacity (IC) =IRV + TV =3800 ml It is the maximum volume of air that is inspired from the end expiratory position Expiratory capacity (EC) =ERV + TV =1500 ml It is the maximum volume of air that is expired from the end inspiratory position Functional residual capacity (FRC) or Functional residual volume (FRV) RV + ERV = 2200 ml It is the normal amount of air present in the lungs after normal expiration
 = IRV + TV + ERV =4800 ml It is")
Vital capacity (VC) = IRV + TV + ERV =4800 ml It is the maximum amount of air that is expelled out forcefully after a maximal (deep ) inspiration Total lung capacity (TLC) IRV + TV + ERV + RV = 6000 ml (6 liters) The amount of air present in the lungs after maximal deep inspiration

Variations All lung volumes & Capacities Varies depend upon sex, size & body build of the individual It increases proportionate to size About 20 to 25% less in female than male More in athletic & large persons

Limitation of spirometry ØWith spirometry – the volumes & capacities that can be expired out only can measure ØHence, the volume which cannot be measured by spirometry are– ØResidual volume (as it cannot expired out) ØSo, also, FRC & TLC (as these include RV)
 Closed circuit method (Helium")
Measurement of FRC Open circuit method (Nitrogen washed out method) Closed circuit method (Helium dilution technique) By Body Plethysmograph method

VITAL CAPACITY It is the maximum amount of air that is expelled out forcefully after a maximal or deep inspiration IRV + TV + ERV =4800 ml

PHYSIOLOGIAL VARIATIONS FSex FBody build FPosture FAthletes

PATHOLOGICAL VARIATIONS FAsthma FEmphysema FParalysis or weakness of respiratory muscles FPneumonia FPulmonary edema FPulmonary tuberculosis

Factors that influence vital capacity FRespiratory muscle power FAirway patency FCompliance of the lung FElasticity and viscosity of the lungs
 or Forced Vital Capacity in unit time (FVC) or Forced")
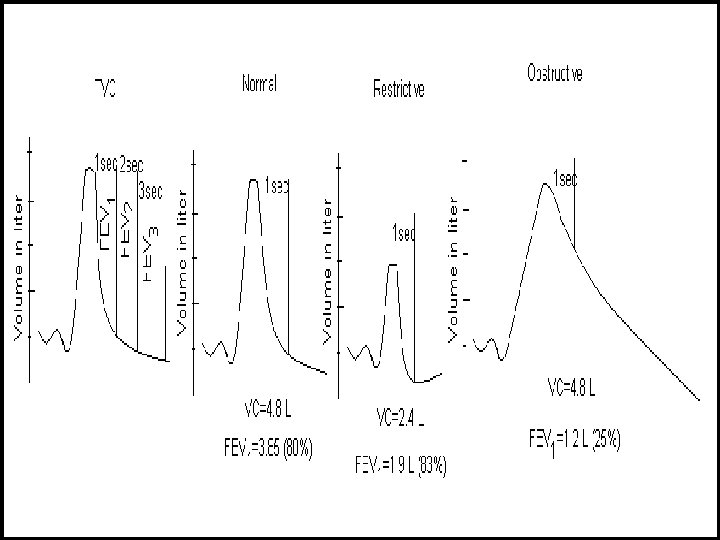
Timed Vital Capacity (TVC) or Forced Vital Capacity in unit time (FVC) or Forced expiratory volumes (FEV) vital capacity measured at each unit time (second). Accordingly, volume expired each unit time is measured and expressed as % of TVC

The amount of air which can expired in given unit time is called forced expiratory volume FEV 1 – 80 to 85% (1 st second) FEV 2 – 90 to 95% (2 nd second) FEV 3 -- >97% (3 rd second) After 3 rd second = 100% of total vital capacity

n Helps to differentiate Restrictive with Obstructive type of respiratory diseases. n Restrictive disorders -- VC decreased; FEV 1 normal (Pulmonary fibrosis; Kyphoscoliosis; spondylitis) n Obstructive diseases --–VC normal & FEV 1 decreased (Bronchial asthma; Emphysema)
 The amount of air moved in and out of the")
Respiratory minute volume (RMV) The amount of air moved in and out of the lungs every minute TV X RR = RMV 500 X 12 = 6000 ml (6 litres)
 or Maximum Breathing capacity (MBC) The maximum amount of air")
Maximum Voluntary Ventilation (MVV) or Maximum Breathing capacity (MBC) The maximum amount of air which can be breathed in and out of the lungs by means of forceful respiration (hyperventilation) per minute

§ Determination –With maximum voluntary effort breath as deep & as quick as possible for 15 sec. The amount of air inspired and expired is measured from spirogram. From this MBC is calculated for one minute MBC in 15 sec = n litres n/15 x 60 litre Hyperventilation causes CO 2 washout and leads to respiratory depression may produce fainting therefore, voluntarily it should carried out for 15 sec.

§ Normal value: In healthy adult male it is 150 -170 litres/min and in females it is 80 – 100 litres/min § Varies with age, sex & body size § Also depend on – muscular force available, compliance of thoracic wall & lungs, air way resistance.
 rate The maximum rate at which the air an")
PEFR (Peak expiratory flow rate) rate The maximum rate at which the air an expired after deep inspiration Ø >400 L/min (respiratory Muscle endurance) Ø Useful for assessing the respiratory diseases especially to differentiate the obstructive and restrictive diseases. Ø

Dead Space � The part of the respiratory tract where the gaseous exchange does not take place � Function – Purification, Humidification & Airconditioning � Types – 2 ü Anatomical dead space volume– volume Volume of gas in respiratory tract ( nose - terminal bronchiole). ü Normal value – 150 ml ü Physiological dead space volume - Total dead space volume Anatomical DSV + Volume of air in the alveoli which does not take part in the exchange of gas Normal healthy person – Physiological DSV = Anatomical DSV

Variation Sex: more in males Age : DS increases with age , because inflated lungs pull the air ways thereby increase the airway diameter. Body weight: DS increase in proportion with increase in body weight. Emphysema : loss of elasticity decreases the elastic recoil this causes hyperinflation

Alveolar ventilation It indicates the volume of air which is utilized for gaseous exchange every minute (TV – DSV) X RR (500 – 150) x 12 = 4, 200 ml/min

THANK YOU
- Slides: 35