Pulmonary embolism and anestheisa Presented by R 1

Pulmonary embolism and anestheisa Presented by R 1 李欣融

Pulmonary embolism Pre-operative Considerations -from blood clots, tumor cells, air, amniotic fluid, foreign material -prolonged bed ridden, postpartum state, fracture of long bone, orthopedic surgery with tournique use, carcinoma, heart failure, obesity, OP time>30 mins, hypercoagulability (antithrombin III, protein S, C and plasminogen-activator deficiency)

PATHOPHISIOLOGY Increase the dead space, Pa. CO 2↑, hypoxemia vasoconstriction and reflex PVR increased V/Q mismatch shunt Pulmonary surfactant loss (24 -48 hrs) Pulmonary infarctions Pulmonary hypertension, increased RV afterload, RV failure

Diagnosis Dyspnea, tachypnea, chest pain, hemoptysis, whezzing ABG: hypoxemia with respiratory alkalosis; Arterial to end-tidal CO 2 gradient increase in PE, as an adjunct to unmasking silent pulmonary embolism. The Lancet Ltd, Volume 348(9043), 21/28 December 1996 p 1733 CXR: wedge-shaped density, elevated diaphragm, enlarged pulmonary trunks Cardiac signs: tachycardia, wide splitting S 2, systemic hypotension with increased CVP

Diagnosis EKG: new right axis deviation, RBBB, tall peaked T waves, a finding of an S wave in lead I, a Q wave in lead III or an inverted T wave in lead III, and new T-wave inversion in leads V 1 through V 4 Normal lead 2, rather than to lead 3 Lung scan Pulmonary angiogram
. May 7, 2002. 691 -700")
From: Goldhaber: Ann Intern Med, Volume 136(9). May 7, 2002. 691 -700

Treatments The best treatment for pulmonary embolism is prevention. Heparin 5000 U q 12 h pre-op or immediately post-op in high risk patients Oral; warfarin, aspirin or dextran therapy together High elastic stockings and pneumatic compression

Treatments Heparin-APtt: 1. 5 -2. 4 Low molecular weight heparinsubcutaneous at a fixed dose without monitor Warfarin start with heparin concurrent for 4 -5 days overlap INR: 24 hrs apart Inferior vena cava umbrella filter for bleeding tendency p’ts

Anesthetic Considerations Pre-op management Hx of pulmonary embolism-anticoagulant ; if episode >1 year, the risk of interrupting drugs is low Spinal or epidural anaesthesia->risk of vertebral canal haematoma ↑, permanent paraplegia Reduced by not performing such procedures within 4 hours of the last dose of low dose unfractionated heparin

Anesthetic Considerations LMWH at 8 pm/evening, starting the day before surgery and continuing post-op Today surgery: a neuroaxial block is to be undertaken will be mobile until the block is inserted. Low molecular weight heparin intraop, at least one hour after the procedure, as recommended by Vandermeulen et al. --British Medical Journal 2000. Volume 321(7267) 21 October 2000

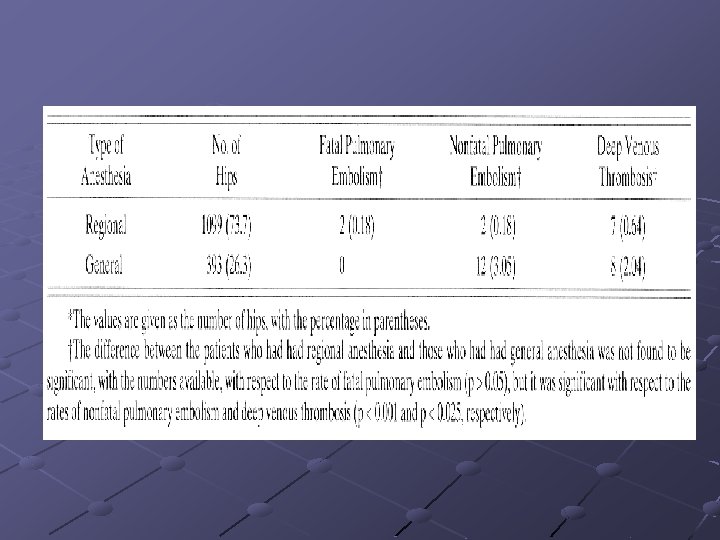
Intraoperative management Vena cava filter placed percutaneously under local anesthesia with sedation Regional anesthesia for hip surgery decrease the post-op deep vein thrombosis and pulmonary embolism Inotropic agent support when embolectomy Opioid, etomidate, ketamine Cardiopulmonary bypass

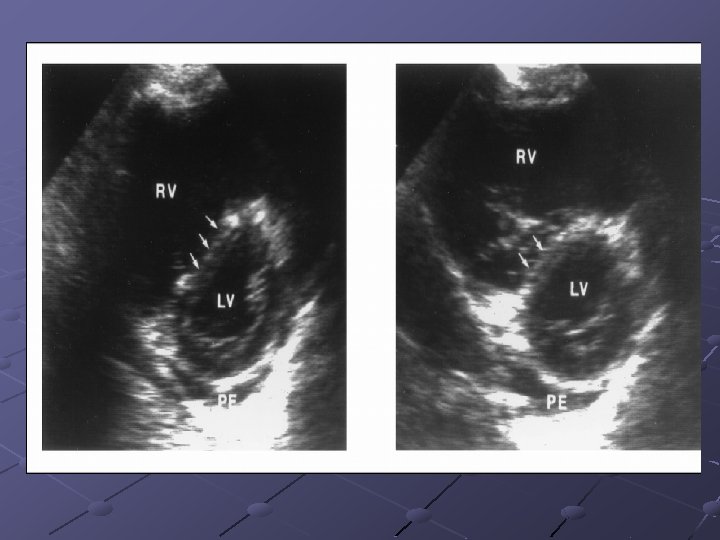
Transesophageal Echocardiography The RPA branches to the right lobar pulmonary arteries can be followed. The LPA interposition of the left main bronchus interferes with the ultrasound beam in the middle portion of the left pulmonary artery. Therefore, thromboembolism is more difficult to detect in the LPA.

Transesophageal Echocardiography

During Total Knee Arthroplasty with Cement 1998 by The Journal of Bone and Joint Surgery, Incorporated Volume 80 -A(3) Medullary canal penetration during endoprosthetic procedures and intramedullary stabilization of fractures of the long bones bone marrow into the circulatory system Healy et al. , little fat and no polymethylmethacrylate monomer activation of the clotting system Venous stasis and intimal damage hypercoaguable state thrombus formation.
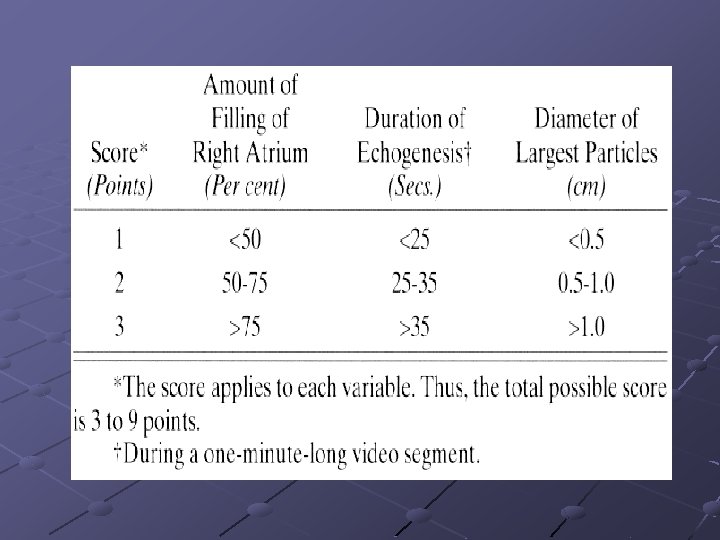

Discussion The intensity of the echogenic showers ≠the intraoperative hemodynamic changes. Embolic score , hemodynamic changes ≠ cement insert Duration of tourniquet ≠ the intensity of the embolic showers Embolic particles > 0. 5 cm in maximum diameter PVR ↑, as a critical variable morbidity and mortality All-or-none effect of the tournique

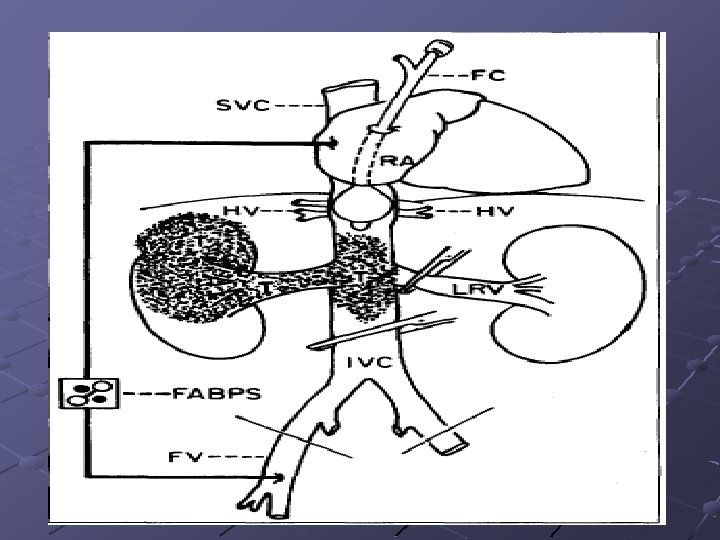
RCC involved IVC Transesophageal Echocardiography and Basket Catheter Can Prevent Tumor Embolism in a Patient with Renal Cell Carcinoma--1998 American Society of Anesthesiologists, Inc. Easily available Easily pushed out and removed from the incision of the inferior vena cava. Effectively to prevent massive tumor embolism Minor pulmonary embolism could not be prevented Further investigation would be needed to clarify the effectiveness of the basket catheter for the prevention of pulmonary embolism.

Malignant RCC extending to IVC The American Journal of surgery, volume 176 August 1998 5 y/o survival rate: 48% to 68% after completely resected, aggressive approach (IVC thrombus remove) means Diagnosis: ultrasound, CT (can’t accurate at superior margin), MRI, venography, Current technology of gradient recall Acquisition in steady state (GRASS), color doppler
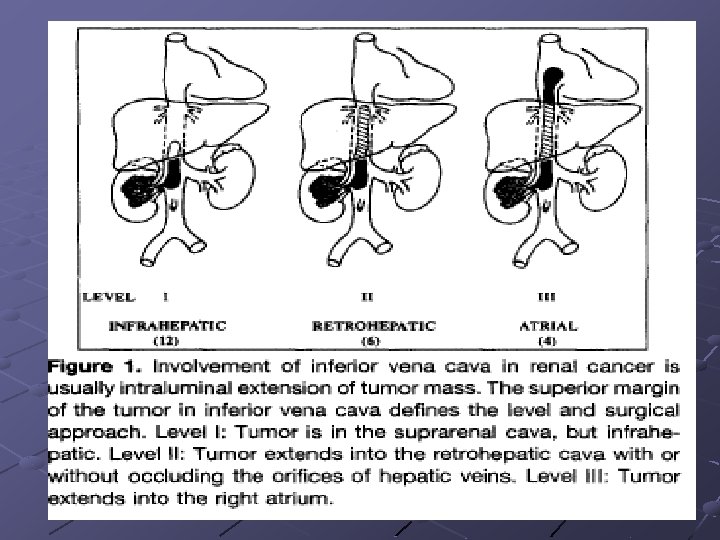

Intra-Op considerations Prevention of tumor embolism control Prevention of tumor embolism IVC above and below tumor by filter Minimal blood loss vascular isolation Minimal blood loss from IVC Maintance the hemodynamic stability by ensure the venous return Centrifual flow ensure the venous return shunt, cardiopulmonary bypass Reduce ischemic time of vital organ

Anesthetic considerations Pre-OP evaluation of tumor extent Intra-OP monitor : TEE, entidal CO 2, CVP, Swan-Guanz, EKG, pulse oximeter Prepare for cardiopulmonary bypass and deep hypothermic cardiac arrest Extracorporeal venous shunting ※ J. Clin. Anesth, vol 13, December, 2001

Anesthesia intervention Thoracic, but Not Lumbar, Epidural Anesthesia Improves Cardiopulmonary Function in Ovine Pulmonary Embolism --2001 by International Anesthesia Research Society. Klinik und Poliklinik für Anästhesiologie und Operative Intensivmedizin, Universitätsklinikum Münster, Germany Epidural anesthesia-induced sympathetic blockade, ( thoracic and lumbar levels), (I) 6 m. L bupivacaine 0. 175% (Thoracic Epidural Anesthesia [TEA] group), 6 m. L saline 0. 9% (TEA-Control group), respectively, via an epidural catheter (T 3 level). (II) 2. 8 m. L bupivacaine 0. 375% (Lumbar Epidural Anesthesia [LEA] group), 2. 8 m. L saline 0. 9% (LEAControl group) epidurally (L 4 level). Embolization : IV injection of au- tologous blood clots (Experiment 1, 0. 75 m. L/kg; Experiment 2, 0. 625 m. L/kg).
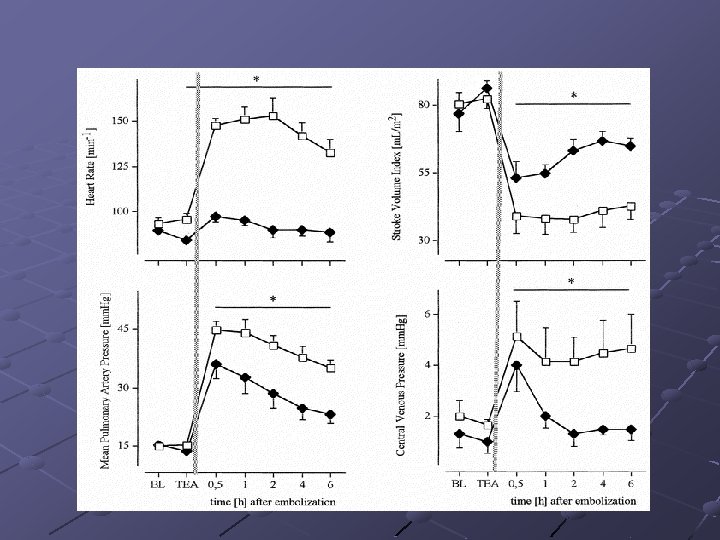
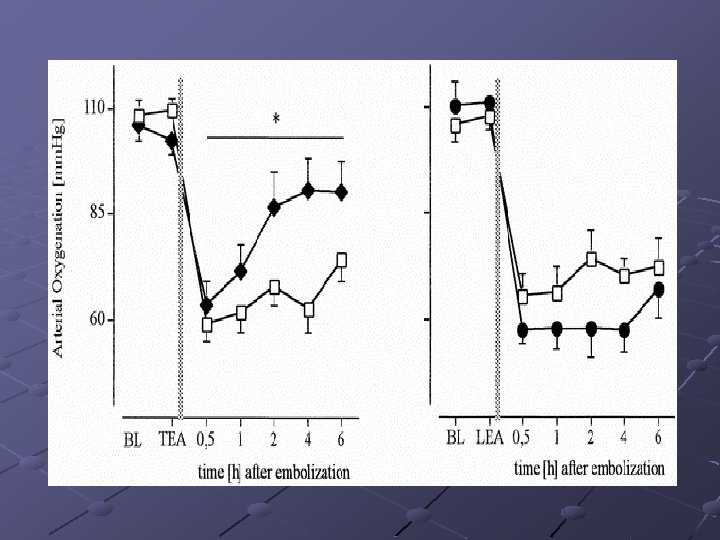
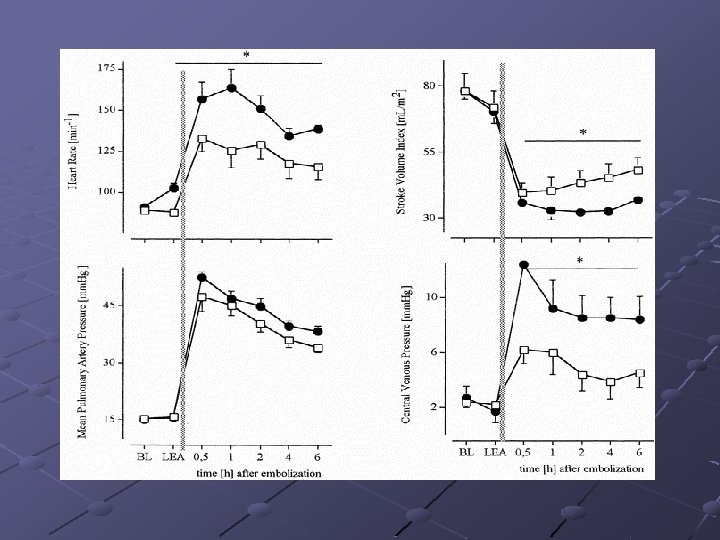
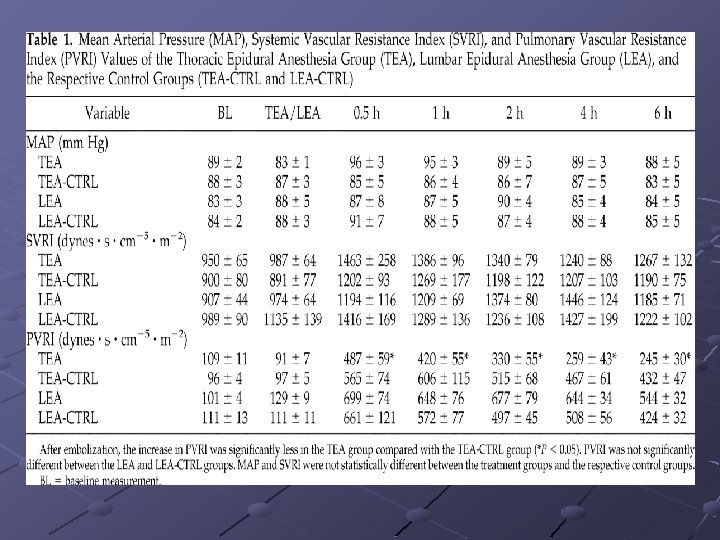

Anesthesia intervention Results: TEA was associated with significantly heart rates, decreased mean pulmonary artery pressures and central venous pressures, and significantly higher stroke volume index and oxygenation in comparison with the TEA-Control group. TEA significantly reduced, and LEA significantly increased, hemodynamic deterioration, suggesting beneficial effects of TEA on cardiopulmonary function during pulmonary thromboembolism.
- Slides: 33