PULMONARY EMBOLI Kenney Weinmeister M D PULMONARY EMBOLI

PULMONARY EMBOLI Kenney Weinmeister M. D.

PULMONARY EMBOLI Over 500, 000 cases per year. w Results in 200, 000 deaths. w Mortality without treatment is 30%. w With therapy mortality drops to 2 -8%. w

RISK FACTORS FOR THROMBOEMBOLIC DISEASE Obesity has an increased risk factor of 2. 9. w Tobacco use: w • 25 -35 cigarettes/day risk factor is 1. 9. • >35 cigarettes/day risk factor is 3. 3. Hypertension caries a risk factor of 1. 9. w Factor V Leiden mutant is seen in 40% of idiopathic thromboembolic disease. w

Signs And Symptoms w w w Tachypnea 70% Rales 51% Tachycardia 30% S 4 24% Accentuated P 2 23% Dyspnea 73% w Pleuritic Chest Pain 66% w Cough 37% w Hemoptysis 13% w

MASSIVE PE DEFENITION Systolic BP less than 90 mm. Hg w Drop in systolic BP of > 40 mm. Hg from baseline for > 15 minutes, not explained by hypovolemia, sepsis, or a new arrhythmia w Two or more lobar arterial occlusions w Task Force on Pulmonary Embolism, European Society of Cardiology. Eur Heart J 2000

MASSIVE PE PATHOPHYSIOLOGY w Increased afterload on right ventricle • Occlusion of vascular bed • Vasoconstriction w Elevated pulmonary artery pressure • 50% obstruction before mean PAP rises w Right ventricle fails • 75% obstruction of vascular bed w Death

DIAGNOSIS ECG w ABG w CHEST X-RAY w D-dimer: w • ELISA method D-dimer < 500 ng/ml has a negative predictive value of 95 to 99%. • Turbidimetric D-dimer

D-dimer Unidirectional. w A negative quantitative rapid ELISA result is as diagnostically useful as a normal V/Q scan or negative venous dopplers. w Unlikely to be helpful in patients with recent surgery (within three months) or with malignancy. w

ECHOCARDIOGRAPHY RV dysfunction w Mobile cardiac emboli were seen in 18% of 130 patients with massive PE w Prospective study of 317 pts, 27% had RV dysfunction on Echo. Mortality with RV dysfunction 13%, without 0. 9% w • Heart 1997

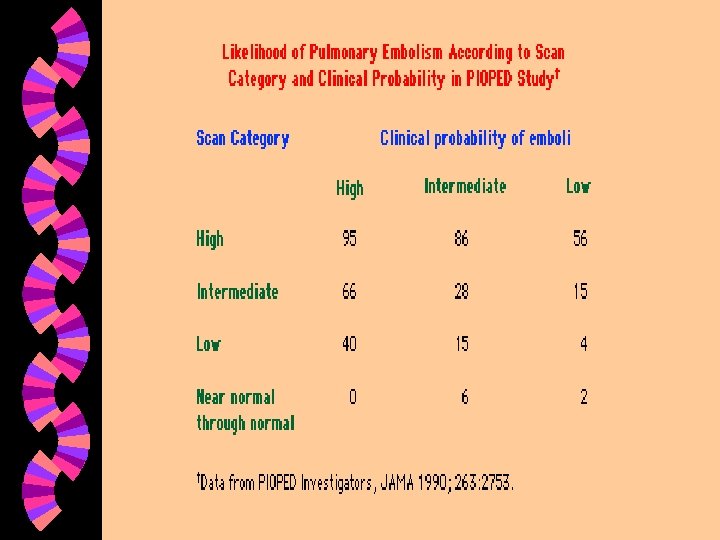
DIAGNOSIS: Ventilation Perfusion Scan w High probability: • > 2 Large segmental defects • > 2 Moderate segmental defects with 1 Large • > 4 Moderate segmental defects w Intermediate probability: not falling into low or high probability.

DIAGNOSIS: Ventilation Perfusion Scan w Low probability: • Nonsegmental perfusion defects. • Single moderate mismatched segmental perfusion defect with normal cxr. • Large or moderate segmental defects with matching defects. • > 3 small segmental perfusion defects. w Normal: no perfusion defects.

Venous Doppler w B-Mode compression ultrasound: • 6 level one studies; • • w Sensitivity 89 - 100% Specificity 86 - 100% Positive Predictive Value 92 - 100% Negative Predictive Value 75 - 100% Duplex US and Color flow doppler US have similar results.

PULMONARY ANGIOGRAPHY Gold standard. w Mortality 0. 2 - 0. 5% w Morbidity 1 - 4% w

SPIRAL COMPUTED TOMOGRAPHY Greatest sensitivity for emboli in the main, lobar or segmental pulmonary arteries. w Only level 2 studies which show: w • Sensitivity 60 -100% • Specificity 78 - 97%

Spiral Computed Tomography w 1041 patients, anticoagulation withheld for negative CTA and dopplers. 360 (34%) dx with PE. 55 had + dopplers and negative CTA. 76 pts high probability PE but negative CTA & dopplers 4 had + V/Q or PAG. 507 not treated, 9 (1. 8%) had TED at f/u. Lancet 2002 Dec 14; 360(9349): 1914 -1920

Spiral Computed Tomography w 548 pts negative or low probability V/Q or negative CTA. PE found in 2 (1%) of 198 pts with neg CTA, 0 pts of 188 with neg V/Q, and five (3%) of 162 pts with low prob V/Q. Radiology 2000 May; 215(2): 535 -42

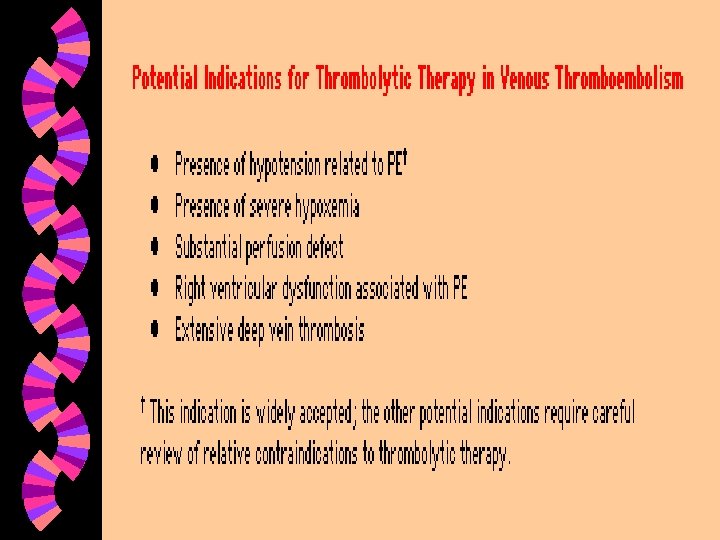
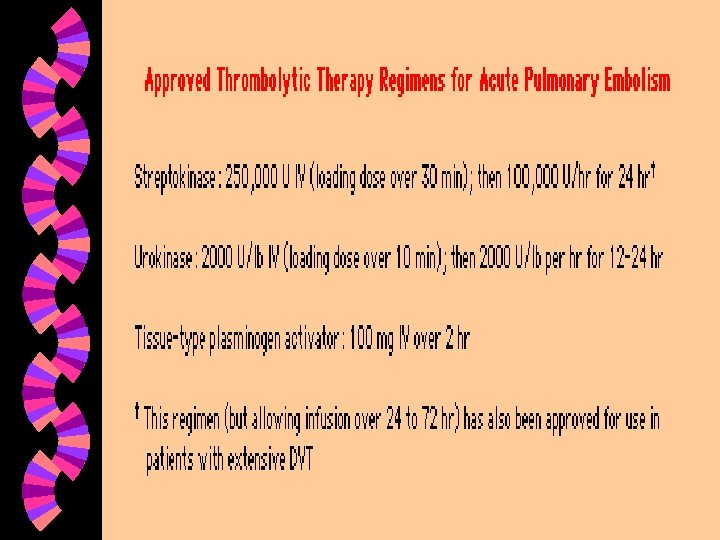
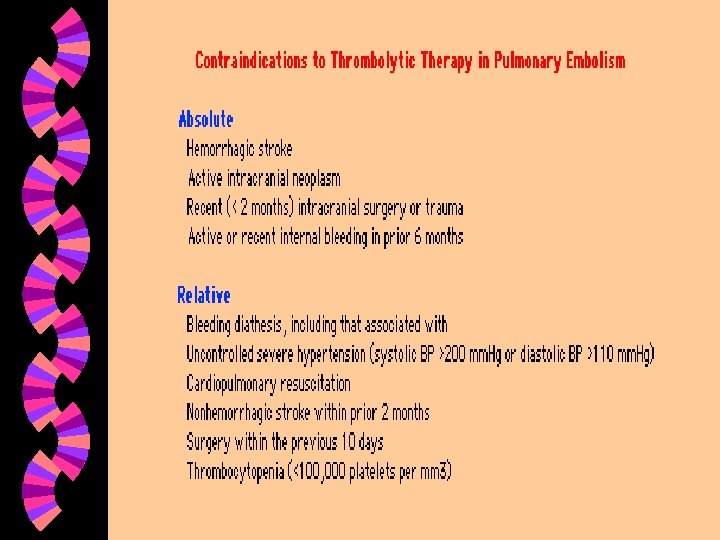
TREATMENT Anticoagulation w Thrombolitics w IVC filter w Thrombectomy w • Catheter • Surgery

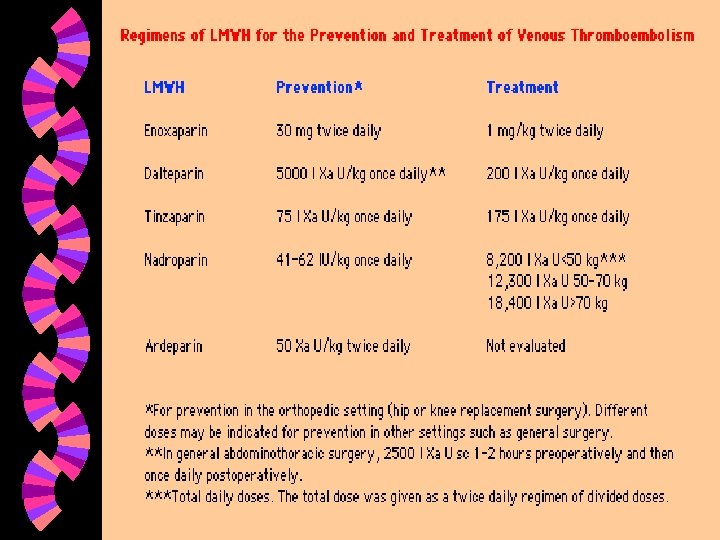
ANTICOAGULANTS w w w Heparin Low molecular weight heparin Direct thrombin inhibitors Factor Xa inhibitors Coumadin
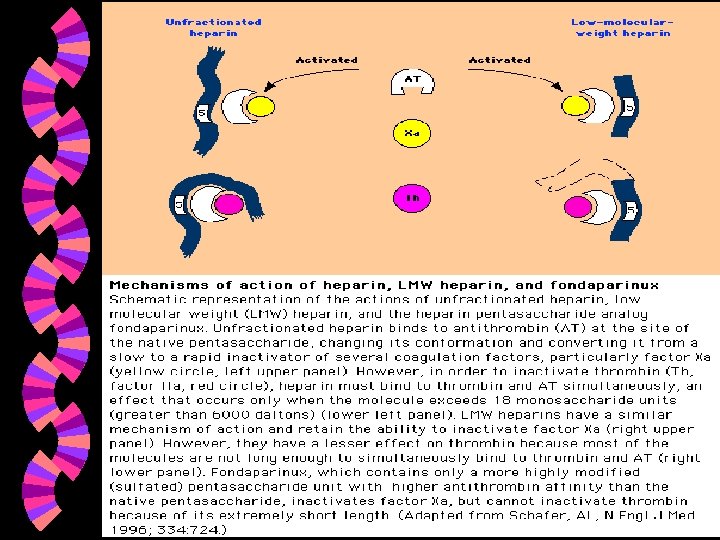

HEPARINS w Heparin • dose on weight base w LMWH • Some trials illustrate safety and efficacy of outpatient therapy or initiation of in hospital use and discharge on coumadin and LMWH.

Direct Thrombin Inhibitors w w w Hirudin Lepirudin Argatroban Ximelagatran Bivalirudin

Factor Xa Inhibitors Fondaparinux w Razaxaban w

DURATION OF THERAPY BY RISK FOR RECURRENCE First event, age < 60 w 3 -6 months w First event, age > 60 or w 6 -12 months idiopathic disease w Recurrent event or first w 12 months to lifetime event with a nonreversible risk factor w

INFERIOR VENA CAVA FILTER No large studies have been performed to evaluate the impact on recurrence of PE. w No large prospective studies have been performed with regards to safety and efficacy. w Mortality 0. 1 to 0. 2% w Morbidity up to 18% risk of thrombosed IVC. w

CONCLUSION The diagnosis of PE is difficult and cannot be made on clinical criteria. w Large clinical trials are needed to evaluate the new imaging techniques as well as new diagnostic tests. w Failure to diagnose continues to be one of the largest causes of malpractice claims. w
- Slides: 33