Pulmonary Alterations Pulmonary Embolism PE Blockage of a

Pulmonary Alterations Pulmonary Embolism

PE • Blockage of a pulmonary artery by an embolus or blood clot that has travelled by another location in the body • May manifest as: • Several tiny clots • One large clot • Multitude of showered clots in the lung
 or clots in other areas • Chronic")
Risk Factors • Deep Vein Thrombosis (DVT) or clots in other areas • Chronic bedrest • Hypercoagulability • Genetic • Cancer • Surgery • Cardiac Conditions • CHF • MI • Obesity • Women on hormone therapy • Contraceptives • Hormone replacement therapy

PE-Pathophysiology • Portion of a thrombus dislodges and travels as an embolus through the venous circulation to the right side of the heart and enters the pulmonary artery and lodges there • You have decreased blood flow to the lung • Two other sources to compensate • Air from the bronchi • Oxygen from the blood flow from the bronchial artery arising from the descending portion of the aorta

Pulmonary infarction • The lack of oxygen to the lung is severe enough to cause an infarction (death of lung tissue)

Saddle embolism • Blockage of the entire main pulmonary artery • May be lethal

Consequence of saddle • Right side of heart unable to pump blood sufficiently • Right side of heart distends • Proximal portion of the pulmonary artery also distends • Portion prior to the obstruction • Not enough blood getting through lungs to the left side of heart • Circulatory failure

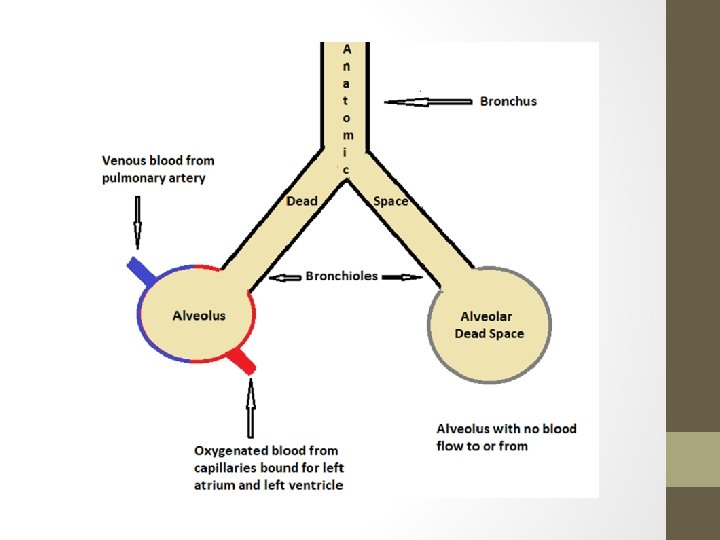
General Results of PE • Ventilation without perfusion • Alters the oxygenation of body tissues • You get increased alveolar dead space • These alveoli are not participating in gas exchange

Complications of PE • • • Pulmonary edema Atelectasis Severe hypoxia Shock Elevated pulmonary circulation pressures

Signs and Symptoms of PE • • Tachypnea Tachycardia Hypotension Sudden acute dyspnea with extreme anxiety Sharp, localized chest or pleuritic pain Abnormal lung sounds Hypoxemia

Signs of severe PE • • Pulmonary hypertension Shock Right heart failure Sudden respiratory arrest

Suspect PE when: • Sudden onset of pleuritic pan coupled with SOB and extreme anxiety • Patients who are covering from: • lower extremity surgery • Childbirth • Major surgery • DVT • Prolonged bedrest

Nursing Assessment • Pain analysis • Type • Location • Does it increase with inspiration • Anxiety level • Skin color • LOC • Respiratory status • Vital signs • Symptoms of DVT • Auscultation of lung sounds

Diagnostics • CXR • May show wedge-shaped density • Atelectasis • Pleural effusion • CT angiogram of chest • Check creatinine level first • VQ scan-Ventilation/Perfusion scan • Radioisotope lung scan • Peripherally blocked areas will show no blood flow • Can’t diagnose an embolus; only gives probability

Labs • D dimer • Fibrin degradation test • Not specific for PE • ABG • Decreased Pa 02 • Decreased Pa. C 02

Additional work-up • ECG • ST-T wave changes • Right axis deviation • Coags • PT & PTT • Baseline for starting anticoagulant therapy • INR • If pt has been on Warfarin to see if it’s therapeutic level

Nursing Management • Medications • Anticoagulants • Heparin • Novel agents • Eliquis, Xarelto • Low molecular weight heparin • Lovenox • Analgesics for pain • Vasopressors if hypotensive • Parenteral fluids if indicated

Nursing Management • Monitor • Rhythm • 02 sats • Vital signs • Pulmonary wedge pressure & cardiac output • Respiratory status • LOC • Skin color • Mental status

Pulmonary Alterations Pulmonary Hypertension

Overview • Elevated pressures in the pulmonary artery • Usually results from pulmonary or cardiac disease • Normal pressure 12 -15 mm. Hg • Resting mean pressure>20 is elevated
 • • Not related to any known cause Higher incidence")
Primary pulmonary hypertension (PPH) • • Not related to any known cause Higher incidence in women 20 -30 years old Highly uncommon Can lead to death in 3 -5 years

Secondary Pulmonary Hypertension • Pulmonary or cardiac disease • Hypoxia • Congenital cardiac disease • Pulmonary Emboli • COPD • Sleep apnea • Mitral stenosis • Left ventricular failure

Cor pulmonale • Results from long-standing pulmonary hypertension • Right ventricular hypertrophy and failure

Pathophysiology • Narrowing of the pulmonary vascular bed from major cardiac or pulmonary diseases • Causes • Vessel destruction • Vasoconstriction or obstruction

Clinical Manifestations • Fatigue • Angina • Dyspnea • Both exertional and resting • Tachypnea • Abnormal breath sounds • What you hear may depend on the underlying condition • Dizziness • Cyanosis

Nursing Assessment • • Symptom analysis of any physical complaints Skin color Signs of edema Vital signs Use of accessory respiratory muscles Breath sounds Heart sounds • The second heart sound is frequently accentuated • Extra heart sounds such as S 3 & S 4 • Murmurs

Diagnostics • CXR • Enlarged right ventricle • Dilated pulmonary arteries • ECG • Right ventricle hypertrophy • Right axis deviation • Right BBB • Echocardiogram • Enlarged right atrium • Decreased wall motion • Decreased EF

Labs • CBC • Polycythemia • d/t chronically low oxygen levels • ABG • Hypoxemia

Medications • Calcium channel blockers • Nifedipine • Diltiazem • Lower pulmonary vascular resistance • Vasodilators • Decrease preload • Sildenafil (Viagra) • Vasodilate pulmonary arteries • ACE inhibitors (the “prils”) • Diuretics

Nursing Management • • Oxygen Fluid restriction Low sodium diet Monitor activity intolerance • Cluster activities • Assist with ADLs Monitor VS, lung sounds, and heart sounds High Fowler’s if needed Encourage coughing and deep-breathing Patient and family education
- Slides: 32