Puede ser la inmunoterapia el tratamiento esperado en


: Survival 1. 0")








, n (%) SD ≥ 24")









 Check. Mate 143: Ph I/III study of")

 Nivolumab 1")
, years Age, years, n (%) <65")
 Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10)")

a Complete response Partial")
 Nivolumab 1 mg/kg + Ipilimumab")
 Nivolumab 1 mg/kg + Ipilimumab")

 ACT IV: Ph III study investigating the addition")
 Randomized Portion (n=70) Re. ACT: Ph II study")





- Slides: 39
¿Puede ser la inmunoterapia el tratamiento esperado en Glioblastoma? Juan M Sepúlveda Sánchez Unidad Multidisciplinar de Neurooncología Hospital 12 de Octubre
Glioblastoma: Sin avances Terapéuticos desde 2005 ESTUDIO AVAGLIO
Ipilimumab, gp 100, or Both in Advanced Melanoma (MDX 010 -20): Survival 1. 0 0. 9 0. 8 Proportion Alive Ipilimumab + gp 100 (A) Ipilimumab alone (B) gp 100 alone (C) Comparison HR P Value Arms A vs C 0. 68 . 0004 Arms B vs C 0. 66 . 0026 0. 7 0. 6 OS, % Ipi + gp 100 (n = 403) Ipi + Placebo (n = 137) gp 100 + Placebo (n = 136) 0. 5 Year 1 44 46 25 0. 4 Year 2 22 24 14 0. 3 0. 2 0. 1 0 0 1 Hodi FS, et al. N Engl J Med. 2010; 363: 711 -723. 2 Yrs 3 4
Ipilimumab: Pooled Survival Analysis from Phase II/III Trials in Advanced Melanoma 1. 0 0. 9 N = 1861 Median OS (95% CI): 11. 4 mo (10. 7 -12. 1) 3 -year OS Rate (95% CI): 22% (20% to 24%) Proportion Alive 0. 8 0. 7 0. 6 0. 5 0. 4 0. 3 0. 2 0. 1 Ipilimumab CENSORED 0. 0 0 Patients at Risk Ipilimumab 1861 12 24 36 48 60 72 84 96 108 120 26 15 5 0 Months 839 370 254 192 170 Schadendorf D, Hodi FS, Robert C, et al. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J Clin Oncol 2015; 33: 1889 -94.
Tumor Immunology: Overview perforin granzyme cytokines Resting T cell Activated T cell TUMOR Tumor antigen LYMPH NODE T cell clonal expansion TCR MHC B 7 Dendritic cell CD 28
Tumor-Derived Immune Suppression Tumors go to great lengths to evade the immune response Systematic studies have identified multiple mechanisms cancers employ to defeat the immune response ◦ Immunosuppressive cytokines: TGF-β, IL-4, -6, -10 ◦ Immunosuppressive immune cells: T-regs, macrophage ◦ Disruption of immune activation signaling: loss of MHC receptor, PDL 1, 2 expression Goal: therapy strategies that “liberate” underlying anticancer immune responses Immune checkpoints not even in the picture in 2008! Weiner LM. N Engl J Med. 2008; 358: 2664 -2665.
Noninflamed Tumor Phenotype Poor effector cell trafficking due to: Endothelial cells Macrophage Poor migration X Cytotoxic T cell Chemokines Tumor Fibroblasts Gajewski TF, et al. Curr Opin Immunol. 2011; 23: 286 -292. ◦ High expression of vascular markers, macrophages, fibroblasts ◦ Low inflammation and chemokine expression, few lymphocytes
Inflamed Tumor Phenotype T cell recruitment Migration ◦ High levels of innate immune signals PD-L 1 ◦ Chemokine expression Tumor Cytotoxic T cell Chemokines Nevertheless, negative immune regulators dominate ◦ Inhibitory receptors Anergy T T reg ◦ Suppressive cells ◦ Suppressive enzymes T MDSC Gajewski TF, et al. Curr Opin Immunol. 2011; 23: 286 -292. Spranger S, Gajewski T. J Immunother Cancer. 2013; 1: 16.
Inflamed Tumor Phenotype T cell recruitment ◦ High levels of innate immune signals Migration PD-L 1 ◦ Chemokine expression Tumor Cytotoxic T cell Chemokines Nevertheless, negative immune regulators dominate Blocking PD 1: PD-L 1 binding might activate immunity within the tumor microenvironment PD 1 Anergy T T reg T MDSC Gajewski TF, et al. Curr Opin Immunol. 2011; 23: 286 -292. Spranger S, Gajewski T. J Immunother cancer. 2013; 1: 16.
PD-1 Adaptive Resistance to Immunotherapy Anti–PD-1 Anti–PD-L 1 Tumor cell -1 -L 1 D P PD R TC C H M Interferons PD-L 1 can be expressed on tumor cells either endogenously or induced by association with T cells (adaptive immune resistance)[1, 2] ◦ PD-1: PD-L 1 interaction results in T cell suppression (anergy, exhaustion, death) In RCC, melanoma, and other tumors, PD-L 1 expression has been shown to be associated with adverse clinical/pathologic features, eg, more aggressive disease and shorter survival [3] 1. Topalian SL, et al. Curr Opin Immunol. 2012; 24: 207 -212. 2. Taube JM, et al. Sci Transl Med. 2012; 4: 127 ra 37. 3. Thompson RH, et al. Proc Natl Acad Sci USA. 2004; 101: 17174 -17179.
Clinical Development of Inhibitors of PD-1 Immune Checkpoint Target PD-1 PD-L 1 Antibody Molecule Development stage Nivolumab (BMS-936558) Fully human Ig. G 4 Phase III multiple tumors (melanoma, RCC, NSCLCa, HNSCC) Pembrolizumab (MK-3475) Humanized Ig. G 4 Phase I-II multiple tumors Phase III NSCLC/melanoma Pidilizumab (CT-011) Humanized Ig. G 1 Phase II multiple tumors MEDI-4736 Engineered human Ig. G 1 Phase I-II multiple tumors MPDL-3280 A Engineered human Ig. G 1 Phase I-II multiple tumors Phase III NSCLC MSB 0010718 C Fully human Ig. G 1 Phase I solid tumors
Nivolumab: Clinical Activity Tumor Type Dose, mg/kg ORR (CR/PR), n (%) SD ≥ 24 Wks, n (%) Median PFS, Median OS, Mos 1 yr, % 2 yr, % MEL (n = 107) 0. 1 -10 32 (34) 7 (7) 3. 7 17. 3 68 48 NSCLC (n = 129) 1 -10 22 (17) 13 (10) 2. 3 9. 9 42 24 RCC (n = 34) 1 or 10 10 (29) 9 (27) 7. 3 > 22 70 50 28 responses (16 MEL, 6 RCC, and 6 NSCLC) lasted ≥ 1 yr among 54 patients with treatment initiation ≥ 1 yr before data analysis 13 patients (4 MEL, 6 NSCLC, 3 RCC) demonstrated nonconventional patterns of response but were not included as responders Topalian SL, et al. N Engl J Med. 2012; 366: 2443 -2454. Hodi FS, et al. ASCO 2014. Abstract 9002. Brahmer JR, et al. ASCO 2014. Abstract 8112.
Nivolumab: Durability of ORR in Pts With Advanced NSCLC, MEL and RCC 65 of 306 pts had ORR (CR/PR): Squamous NSCLC Nonsquamous Maximum treatment duration 30 of 65 (46%) responses were evident at first tumor evaluation (8 wks) 42 of 65 (65%) pts had responses lasting > 1 yr MEL Ongoing response Time to response 35 of 65 (54%) responses were ongoing at time of data analysis Responses persisted off drug RCC 0 72 120 144 24 96 48 Wks since treatment initiation Topalian SL, et al. ASCO 2013. Abstract 3002. 168
MPDL 3280 A: Tumor Burden Over Time in Urothelial Bladder Cancer • Median time to first response was 42 days (range, 38 to 85 days) • Median duration of response has not been reached – 0. 1+ to 30. 3+ weeks IHC (IC) 2 or 3 and 0. 1+ to 6. 0+ weeks for IHC (IC) 0 or 1 Best response is not known for 7 patients. Patients dosed by Nov 20, 2013 (≥ 6 wk follow-up) with measurable disease at baseline and at least 1 post-baseline measurement. Clinical data cutoff was Jan 1, 2014. Powles T, et al. ASCO 2014. Abstract 5011.
Immune Privilege in the Brain: Old Paradigm Historical belief was that “immune privilege” in the brain was equivalent to “immune isolation”[1 -3] ◦ Presence of BBB ◦ Absence of lymphatic drainage system ◦ Ability to tolerate foreign antigens without eliciting an inflammatory response ◦ Low baseline levels of MHC expression ◦ Altered expression of T-cell costimulatory molecules BBB, blood-brain barrier; MHC, major histocompatibility complex. 1. Jackson CM et al. Clin Cancer Res. 2014; 20(14): 3651 -3659. 2. Heimberger AB, Sampson JH. Neuro Oncol. 2011; 13(1): 3 -13. 3. Carson MJ et al. Immunol Rev. 2006; 213: 48 -65. 15
The BBB is Not an Absolute Barrier to Immune Response Component Effect / Impact on the BBB Glioblastoma cells[1] • Release factors that disrupt endothelial tight junctions Glioblastomaassociated vasculature[1 -4] • Display abnormal structural features, including loss or abnormal morphology of tight junctions, as well as increased permeability Activated T cells[5, 6] • High levels of Very Late Antigen-4 (VLA-4) and leukocytefunction-associated antigen (LFA-1) allow movement across BBB • Can patrol the CNS for antigens in an unrestricted manner Peripheral immune system activation[6] • BBB leakiness and movement of activated macrophages and dendritic cells across BBB, blood-brain barrier; CNS, central nervous system; LFA-1, leukocyte-function-associated antigen-1; VLA-4, very late antigen-4. 1. Schneider SW et al. Acta Neuropathol. 2004; 107(3): 272 -276. 2. Rascher G et al. Acta Neuropathol. 2002; 104(1): 85 -91. 3. Abbott NJ et al. Neurobiol Dis. 2010; 37(1): 13 -25. 4. Wolburg H et al. Acta Neuropathol. 2003; 105(6): 586 -592. 5. Ransohoff RM et al. Nat Rev Immunol. 2003; 3(7): 569 -581. 6. Carson MJ et al. Immunol Rev. 2006; 213: 48 -65. 16
“Immune privilege” is being redefined: Communication between the CNS and immune system exists Microglia, macrophages, astrocytes, and dendritic cells are found within the CNS and may have roles in immune surveillance[2 -6] Functional lymphatic vessels have been observed in the CNS[7] CNS antigens drain through CSF Cervical lymph node CNS antigens are circulated to cervical lymph nodes[1] Glioblastoma microenvironment Activated T cells: [2, 3] • Cross the BBB • Patrol the CNS in an unrestricted manner • Return to systemic circulation BBB, blood-brain barrier; CNS, central nervous system; CSF, cerebrospinal fluid. 1. Jackson CM et al. Clin Cancer Res. 2014; 20(14): 3651 -3659. 2. Heimberger AB, Sampson JH. Neuro Oncol. 2011; 13(1): 3 -13. 3. Glass R, Synowitz M. Acta Neuropathol. 2014; 128(3): 347 -362. 4. Carson MJ et al. Immunol Rev. 2006. 213: 48 -65. 5. Ransohoff RM, Engelhardt B. Nat Rev Immunol. 2012; 12(9): 623 -635. 6. Jackson C et al. Clin Dev Immunol. 2011: 732413. doi: 10. 1155/2011/732413. 7. Louveau A et al. Nature. 2015; 523(7560): 337 -341. doi: 10. 1038/nature 14432. 17
GBM-related Inmunosupression
Cancer Immunity Cycle Chen DS, et al. Immunity. 39: 1 -10, 2013.
PD-1 and CTLA-4 Blockade Prolonged Survival in a Preclinical Mouse Model GL 261 murine glioma tumor-bearing mice were treated with anti-murine CTLA-4 and anti-murine PD-1 or anti-murine PD-L 1 blocking antibodies: Percent Survival 100 80 60 40 20 0 0 20 40 60 80 100 120 140 Days of Treatment Ig. G control α-CTLA-4 α-PD-1 Combo CTLA-4, cytotoxic T-lymphocyte antigen-4; Ig. G, immunoglobulin G; PD-1, programmed death-1. 1. Reardon DA et al. Poster presentation at ASCO 2014. 2084. 20
Society for Neurooncology Nov 2015 Abstracts Related with Checkpoint inhibitors
Trial Design for Check. Mate 143 (Nivolumab) Check. Mate 143: Ph I/III study of nivolumab as monotherapy or in combination with ipilimumab in GBM[2, 3] CTLA-4 CD 28 PD-1 OX 40 TIM-3 CD 137 LAG-3 Adapted from Mellman I et al 2011. [1] Start Date: January 2014 Safety Phase (n=~100) Key Eligibility Criteria • 1 st recurrence* Key Eligibility Criteria • Newly diagnosed Cohort 1 (randomized): • Nivo + ipi Cohort 1 c: Nivo + RT + TMZ Cohort 1 b (nonrandomized): Nivo + ipi Cohort 1 d (unmethylated: Nivo + RT Primary Endpoint: Safety and tolerability Phase III (n=340) Key Eligibility Criteria • 1 st recurrence* Cohort 2 (randomized): • Nivo • Bev Primary Endpoint: OS Secondary Endpoints: OS 12, PFS, ORR * After RT and TMZ. Bev, bevacizumab; GBM, glioblastoma; Ipi, ipilimumab; nivo, nivolumab; ORR, objective response rate; OS, overall survival; OS 12, OS at 12 months; PFS, progression-free survival; PD-1, programmed death-1; RT, radiotherapy; TMZ, temozolomide. 1. Mellman I et al. Nature. 2011; 480(7378): 480 -489. 2. Sampson J et al. Poster presentation at ASCO 2015. 3010. 3. Clinicaltrials. gov. NCT 02017717. 22
Safety and Activity of Nivolumab Monotherapy and Nivolumab in Combination With Ipilimumab in Recurrent Glioblastoma: Updated Results from CHECKMATE-143 John Sampson, 1 Antonio Omuro, 2 Gordana Vlahovic, 1 Solmaz Sahebjam, 3 Joachim Baehring, 4 David A. Hafler, 4 Alfredo Voloschin, 5 Robert Latek, 6 Vlad Coric, 6 a Timothy Cloughesy, 7 Michael Lim, 8 David A. Reardon 9 1 Duke University Medical Center, Durham, NC; 2 Memorial Sloan Kettering Cancer Center, New York, NY; 3 Moffitt Cancer Center, Tampa, FL; 4 Yale School of Medicine, New Haven, CT; 5 Emory University School of Medicine, Atlanta, GA; 6 Bristol-Myers Squibb, Lawrenceville, NJ; 7 University of California, Los Angeles, CA; 8 The Johns Hopkins Hospital, Baltimore, MD; 9 Dana-Farber Cancer Institute and Harvard University School of Medicine, Boston, MA a. At the time this work was conducted, Vlad Coric was affiliated with Bristol-Myers Squibb 23
Study Design and Eligibility Criteria Nivolumab 3 mg/kg Q 2 W (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg Q 3 W x 4 doses, then nivolumab 3 mg/kg Q 2 W thereafter (n=10) Nivolumab 3 mg/kg + Ipilimumab 1 mg/kg Q 3 W x 4 doses, then nivolumab 3 mg/kg Q 2 W thereafter Eligible patients had no prior bevacizumab treatment and Karnofsky performance status ≥ 70 All patients in Cohort 1 had prior surgical resection, radiation, and temozolomide Patients received nivolumab for up to 2 years Imaging for disease assessment occurred every 6 weeks 24
Demographics and Clinical Characteristics Characteristic Median age (range), years Age, years, n (%) <65 ≥ 65–<75 Gender, n (%) Male Female Race, n (%) White Black/African-American Karnofsky performance score, n (%) 90 80 70 Histopathologic diagnosis, n (%) Glioblastoma Gliosarcoma MGMT gene promoter methylation status, n (%) Methylated Unmethylated Missing Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) 59 (42– 73) 57 (37– 68) 6 (60) 4 (40) 7 (70) 3 (30) 5 (50) 6 (60) 4 (40) 8 (80) 2 (20) 10 (100) 0 7 (70) 1 (10) 2 (20) 6 (60) 1 (10) 3 (30) 9 (90) 1 (10) 10 (100) 0 2 (20) 4 (40) 2 (20) 6 (60) 2 (20) 25
Patient Disposition Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) Patients in the treatment period, n (%) Continuing on treatment Not continuing on treatment 1 (10) 9 (90) 0 10 (100) Reason for not continuing on treatment, n (%) Disease progression Study drug toxicity Death 9 (90) 0 0 6 (60) 3 (30) 1 (10) Patients in the study, n (%) Continuing on study Dieda 3 (30) 7 (70) 1 (10) 9 (90) a Patient deaths in both treatment arms were due to disease At the time of data cutoff (September 9, 2015), one patient in the nivolumab monotherapy arm continues to receive nivolumab after 17. 5 months of treatment No patients receiving nivolumab monotherapy discontinued treatment due to drug toxicity. There were no deaths due to drug toxicity in the monotherapy or combination treatment arms Three patients receiving nivolumab monotherapy remain on study 26
Treatment-Related AEs Occurring in ≥ 2 Patients in Either Treatment Arm Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) Any Grades 3– 4 9 (90) 0 10 (100) 9 (90) Fatigue 3 (30) 0 8 (80) 1 (10) Diarrhea 1 (10) 0 7 (70) 3 (30) Lipase increased 2 (20) 0 5 (50) AST increased 0 0 5 (50) 1 (10) ALT increased 0 0 4 (40) 2 (20) Maculopapular rash 0 0 4 (40) 0 Vomiting 1 (10) 0 4 (40) 0 Amylase increased 1 (10) 0 3 (30) 1 (10) Headache 2 (20) 0 3 (30) 0 Hyperthyroidism 1 (10) 0 3 (30) 0 Nausea 3 (30) 0 Confusional state 1 (10) 0 2 (20) 1 (10) Hypothyroidism 2 (20) 0 1 (10) 0 Rash 2 (20) 0 1 (10) 0 Any treatment-related AE, n (%) No deaths occurred due to drug-related toxicities 27
Investigator-Assessed Objective Responses per RANO Criteria Best overall response, n (%)a Complete response Partial response Stable disease Progressive disease Unable to determine aper Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) 0 1 (10) 5 (50) 3 (30) 1 (10) 0 0 4 (40) 6 (60) 0 RANO criteria The majority of patients (6/10) treated with nivolumab monotherapy experienced stable disease or better Four patients in the combination arm achieved best responses of stable disease 28
Exploratory Analysis of Overall Survival Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) Median, months (95% CI) 10. 5 (4. 1–NE) 9. 3 (4. 0– 12. 7) Range, months 4. 1– 17. 6 4. 5– 16. 0 6 -month rate (95% CI) 70. 0% (32. 9– 89. 2) 80. 0% (40. 9– 94. 6) 9 -month rate (95% CI) 60. 0% (25. 3– 82. 7) 12 -month rate (95% CI) 40. 0% (12. 3– 67. 0) 30. 0% (7. 1– 57. 8) NE, not estimable 29
Baseline PD-L 1 a Expression Nivolumab 3 mg/kg (n=10) Nivolumab 1 mg/kg + Ipilimumab 3 mg/kg (n=10) 10 (100) 9 (90) 0 – <1% 3 (30) 4 (44) 1 – <5% 2 (20) 2 (22) 5 – <20% 2 (20) 2 (22) ≥ 20% 3 (30) 1 (11) 0 1 (10) Patients with quantifiable PD-L 1 expression at baseline, n (%) Patients without quantifiable PD-L 1 expression at baseline, n (%) a. Tumor PD-L 1 assessment was measured in pre-treatment archival or fresh tumor biopsies using BMS/Dako immunohistochemistry assay (rabbit anti-human antibody, clone 28 -8) PD-L 1 expression ≥ 1% was detectable among the majority of patients 30
CHECKMATE -143 COHORTE 3 -Fase III, randomizada, abierto en GBM recurrente -Nivolumab Vs Bevacizumab en primera recurrencia -340 pacientes -Objetivo principal: SUPERVIVENCIA GLOBAL -Objetivos secundarios: SUPERVIVENCIA LIBRE DE PROGRESIÓN -PRIMER ANÁLISIS INTERMEDIO SE ESPERABA PARA SNO Noviembre 16 pero sólo se va a realizar el análisis final: ASCO 2017
Trial Design for ACT IV (Rindopepimut) ACT IV: Ph III study investigating the addition of rindopepimut to standard of care in newly diagnosed GBM (N=700) Key Eligibility Criteria • Newly diagnosed, EGFRv. III–positive GBM • Attempted surgical resection followed by conventional chemoradiation • No PD after initial therapy EGFRv. III vaccine Randomized: • Rindopepimut (+ GM-CSF) + TMZ • KLH (control) + TMZ Start Date: November 2011 Primary Endpoint: OS Secondary Endpoints: PFS, safety and tolerability EGFRv. III, epidermal growth factor receptor variant III; GBM, glioblastoma; GM-CSF, granulocyte macrophage colony-stimulating factor; KLH, keyhole limpet hemocyanin; OS, overall survival; PD, progressive disease; PFS, progression-free survival; TMZ, temozolomide. 1. Clinicaltrials. gov. NCT 01480479. 32
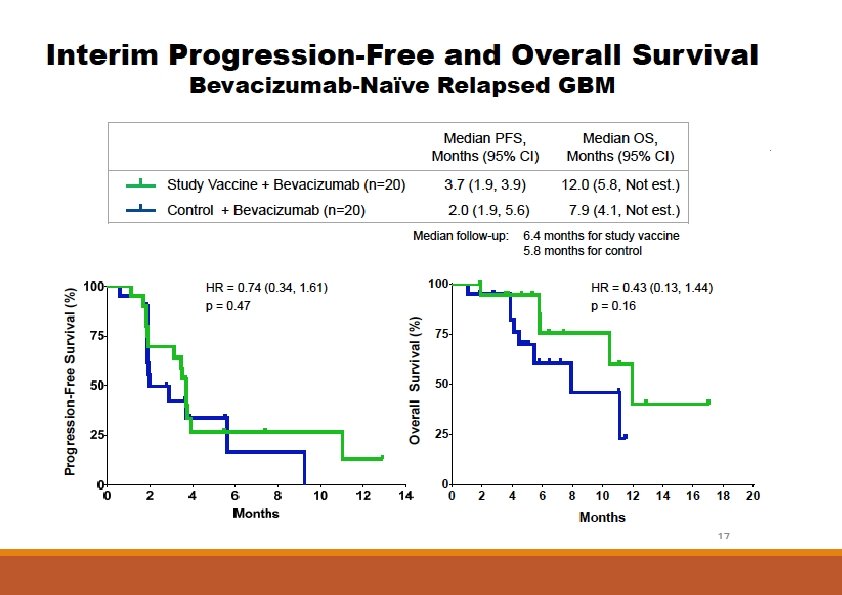
Trial Design for Re. ACT (Rindopepimut) Randomized Portion (n=70) Re. ACT: Ph II study investigating rindopepimut with bevacizumab in relapsed GBM[1, 2] EGFRv. III vaccine Key Eligibility Criteria • EGFRv. III–positive, 1 st or 2 nd relapse* • No prior bev or VEGF/VEGFR therapy Groups 1 A and 1 B (randomized): • Rindopepimut (+ GM-CSF) + Bev • KLH (control) + Bev Start Date: December 2011 Single-Arm Portion (n=~100) Key Eligibility Criteria • EGFRv. III–positive, 1 st or 2 nd relapse* • Bev-refractory Group 2/2 C: Rindopepimut (+ GM-CSF) + Bev Primary Endpoint: PFS (Groups 1 and 2), ORR (Group 2 C) Secondary Endpoints: Safety and tolerability, antitumor activity, EGFRv. III-specific immune response * Of de novo glioblastoma; for secondary glioblastoma, first diagnosis or first relapse. Bev, bevacizumab; EGFRv. III, epidermal growth factor receptor variant III; GBM, glioblastoma; GM-CSF, granulocyte macrophage colony-stimulating factor; KLH, keyhole limpet hemocyanin; ORR, objective response rate; PFS, progression-free survival; VEGF, vascular endothelial growth factor; VEGFR, VEGF receptor. 1. Clinicaltrials. gov. NCT 01498328. 2. Reardon DA et al. Oral presentation at ASCO 2015. 2009. 33
Trial Design for Phase III DCVax-L Trial NCT 00045968: Ph III study investigating the addition of DCVax-L to standard of care in newly diagnosed GBM (N=300) Key Eligibility Criteria • Newly diagnosed GBM • Received attempted GTR + SOC (RT + TMZ) • No PD at end of RT course DCs pulsed with patient tumor lysate Start Date: December 2006 Randomized: • DCVax-L • Placebo Primary Endpoint: PFS Secondary Endpoints: OS, TTP DC, dendritic cell; GBM, glioblastoma; GTR, gross total resection; OS, overall survival; PD, progressive disease; PFS, progression-free survival; RT, radiotherapy; SOC, standard of care; TMZ, temozolomide; TTP, time to progression. 1. Clinicaltrials. gov. NCT 00045968. 35
Trial Design for Phase III ICT-107 Trial NCT 02546102: Ph III study investigating the addition of DCVax-L to standard of care in newly diagnosed GBM (N=414) Key Eligibility Criteria • Newly diagnosed, HLA-A 2–positive GBM • Prior tumor resection followed by chemoradiation DCs pulsed with Tumor Antigens Start Date: November 2015 Randomized: • ICT-107 + TMZ • Control + TMZ Primary Endpoint: OS Secondary Endpoints: OS by MGMT status, PFS, safety and tolerability DC, dendritic cell; GBM, glioblastoma; HLA, human leukocyte antigen; MGMT, O 6 -methylguanine DNA methyltransferase; OS, overall survival; PFS, progression-free survival; TAA, tumor-associated antigen; TMZ, temozolomide. 1. Clinicaltrials. gov. NCT 02546102. 36
Immunotherapeutic Approaches in GBM: Combination Therapy Several combination therapies are being assessed in glioblastoma and malignant brain tumors: [1, 2] ◦ Vaccines + Adoptive Cell Transfer ◦ Vaccines + Chemotherapy, Targeted Therapy, and/or Radiotherapy ◦ Checkpoint Inhibitor Combinations (with other checkpoint inhibitors or other treatment modalities) GBM, glioblastoma. 1. Clinicaltrials. gov. 2. Preusser M et al. Nat Rev Neurol. 2015; 11(9): 504 -514. doi: 10. 1038/nrneurol. 2015. 139. 37
Conclusions Potential for inmune checkpoint inhibitors to benefit patients with GBM ◦ -Brain is not an imnuno privileged site ◦ -Glioblastoma cells express PD 1 L - -Promising results from the first trials with nivolumab (CHECKMATE 143) -Other results with inmunotherapies are expected in 2016: ACT IV, DCVAX…
MUCHAS GRACIAS POR SU ATENCIÓN