Public mental health Peter Byrne Consultant liaison psychiatrist

Public mental health Peter Byrne, Consultant liaison psychiatrist at Homerton Hospital Assoc Registrar / Public mental health lead, RCPsych & Visiting Professor, University of Strathclyde, Glasgow @pubmentalhealth peter. byrne@eastlondon. nhs. uk

Content • • Why and How of Public Mental Health Big 4: our services, stolen years, lifestyle, EI Early intervention: think children and elders Chief Medical Officer (E&W) 2014 Report Inequalities Debates: smoking, vaping & abstaining Start a debate with users, carers & others: the What (to prioritise) of Public Mental Health

Public Education Psychoeducation Public Engagement Public Mental Health

Davies & Mehta, 2014: as quoted by CMO England
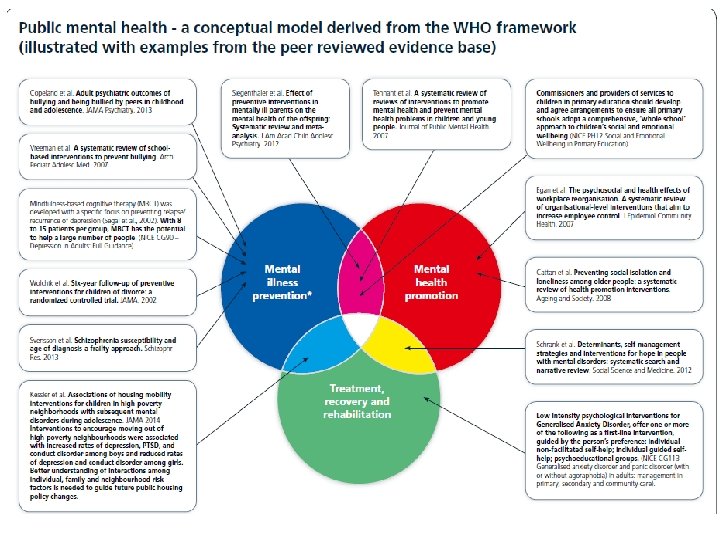
 definition 1. Mental health prevention: e. g. CMO Report of")
Public mental health (PMH) definition 1. Mental health prevention: e. g. CMO Report of 2012 on children, Prevention Pays …(women 2015) 2. Mental health promotion: often this involves NOT doing things (alcohol, drug misuse) as well as proven (exercise, MH first aid) and the not-so-proven (well being promotion) 3. Treatment, recovery, rehabilitation (overlap): this is what MH clinicians spend all time on

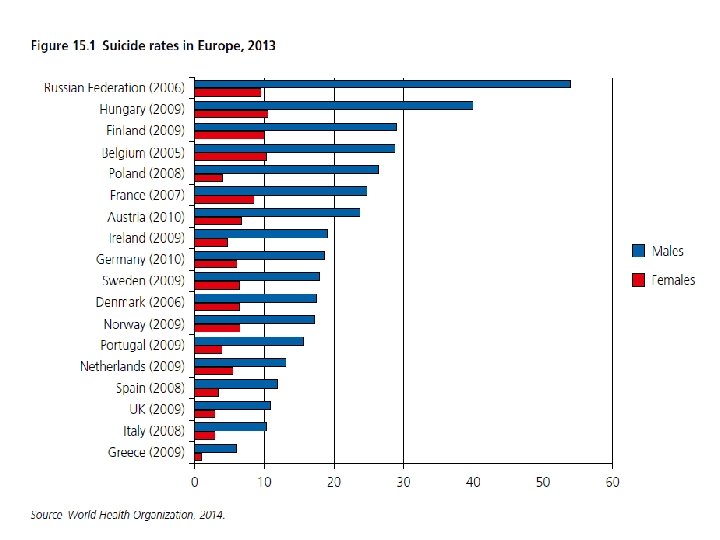
What’s the evidence for PMH? • Epidemiology: RCPsych “ 1 • Special challenges: in 4” tag apples to people who have common mental disorders (depr +/- anxiety): 60% of these are working. alcohol misuse in over 65 s men ↑ by 60% in 20 years; ↑ by 100% in older women equal to 4. 5% LOST to GNP people with SMI die >15 years before the rest of the (matched) population? Glasgow man with SZ loses 26 years; women lose 23 yrs • Premature mortality gap • Economic: £ 70 -100 b/ year = “Stolen years”: why do • Both: since 2008 crash, suicide rates rose by 4%. . . Self harm rates increasing

Start at the beginning: challenges • There are lots of people out there who have MH problems (CMD… alcohol… eating ds…SMI) but are not engaged in any treatment for this We call this the Treatment gap: 75% • Access to services blocked by stigma (incl internalised stigma), gatekeepers, lack of funds • Parity of esteem: MH = 28% of morbidity, but gets 13% of UK health spending, falling slowly

But that is NOT the beginning • Genetic associations with MH disorders • Perinatal interventions protect M and child • Children’s lives ruined by parental alcohol and drug misuse: services cut, alcohol cheaper • Inequalities → MH probs, self harm, stolen years • Current disinvestment in children’s services • Early Intervention: lip service, pilots, or nothing • Evidence-based parenting programmes: no £

Parenting Skills Training Systematic reviews have shown that parenting interventions are effective in improving maternal psychosocial health, (77) reducing child behavioural problems in infants and toddlers, (78) and in children aged 3 to 10 years old, (79) reducing unintentional injuries in children aged 18 years and younger(80) and improving the mental health of families with children with conduct disorders (NICE, 2006). These programmes also reduce antisocial behaviour and offending. (81 -83) RCPsych Response to Marmot (Inequalities) Review, 2010 (77) Barlow J, Coren E, Stewart-Brown S. Parent-training programmes for improving maternal psychosocial health. Cochrane Database of Systematic Reviews 2003; (4). (78) Barlow J, Parsons J. Group-based parent-training programmes for improving emotional and behavioural adjustment in 0 -3 year old children. Cochrane Database of Systematic Reviews 2003; (2). (79) Barlow J, Stewart-Brown SL. Review article: behavior problems and parent-training programs. Journal of Developmental and Behavioral Pediatrics 2000; 21(5): 356 -70. (80) Kendrick D, Barlow J, Hampshire A, Polnay L, Stewart-Brown S. Parenting interventions for the prevention of unintentional injuries in childhood. Cochrane. Database of Systematic Reviews 2007; (4). (81) Hutchings J, et al. Parenting intervention in Sure Start services for children at risk of developing conduct disorder: pragmatic randomised controlled trial. BMJ 2007; 334: 7595. (82) Scott S. An update on interventions for conduct disorder. Advances in Psychiatric Treatment 2008; 14(61): 70. Page 52 of 52 (83) Woolfenden SR, Williams K, Peat J. Family and parenting interventions in children and adolescents with conduct disorder and delinquency aged 10 -17. The Cochrane Database of Systematic Reviews, 2006; 2006.

Concepts and slogans • Cartesian dualism: the separation of diseases of the mind from diseases of the body (mis. Q) • Separation of physical health services from mental health services • No health without mental health • Parity of esteem • No mental health without physical health: mens sano in corpore sano

Two questions • Number One preventable cause of cancer? In reality, the Number One Cause of cancer. • Number 2 preventable cause of cancer?
 Withdrawal seizures Confusion (acute")
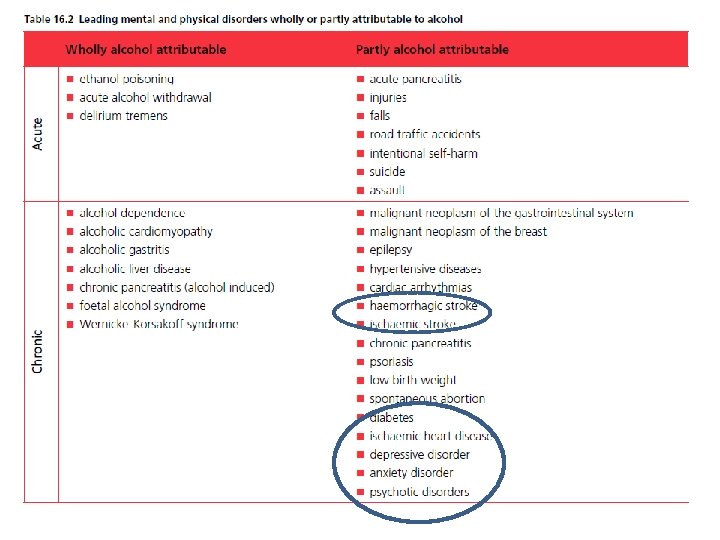
Neuropsychiatric sequelae Alcohol • • • Amnesias (e. g. blackouts) Withdrawal seizures Confusion (acute / chronic) Head injury / subdural Cerebellar damage Peripheral neuropathy Depression & anxiety ↑self-harm, ↑suicide Hallucinosis, psychosis Impotence / libido probs

Evidence based measures: 7 Babor et al, 2010: Alcohol - no ordinary commodity • Pricing: alcohol taxes • Regulate availability: minimum age, licencing hours, no. of outlets • Modify drinking environ: server liability, enforce on premises laws, train staff • Drink driving: best evidence - some behaviours can & need to be stigmatised • Early intervention: selfhelp, mutual help, IBA, medical detox IF linked with talking therapies, weak evid for pharmacol • Restrict marketing: laws work, less so vol codes • Educ & Persuasion: labels, classroom, mass media – less strong evidence

The Great Lie: we need more evidence

, June 2012 The Chief Medical Officer believes that -")
Alcohol Minimum Pricing Act (Scotland), June 2012 The Chief Medical Officer believes that - like the smoking ban - minimum price would save lives within a year. Research by the University of Sheffield estimated that the proposed minimum price of 50 p per unit would result in the following benefits: • Alcohol related deaths would fall by about 60 in the first year and 318 by year ten of the policy • A fall in hospital admission of 1, 600 in year 1, and 6, 500 per year by year ten of the policy • A fall in crime volumes by around 3, 500 offences per year • A financial saving from harm reduction (health, employment, crime etc) of £ 942 m over ten years
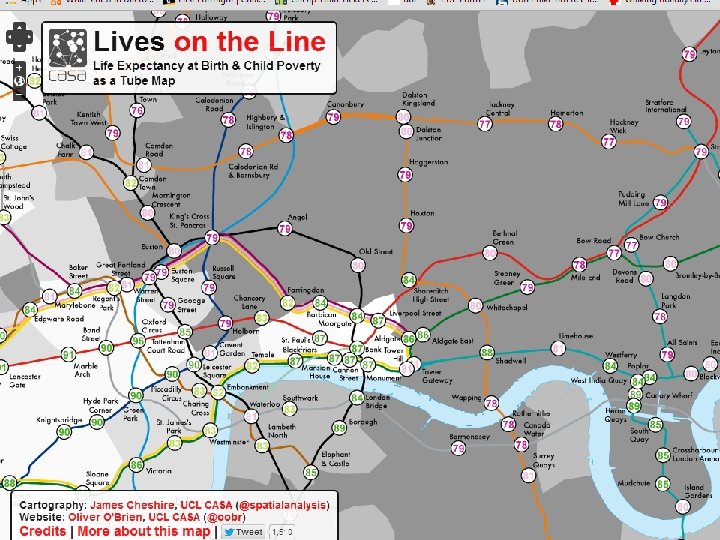

Inequalities Cigarettes Mental illness Low income, U/E, low education, poor health, health risks Worst possible outcomes X 3 fold differences in MH probs and DSH between top 20% and bottom 20% incomes Obesity Alcohol misuse

Self-harm and Suicide • Up to 10% of young people have self harmed, of which 1 in 8 have sought treatment • <65: 30 -40 hosp DSH for each suicide; >65: 10 • Suicide rates fell until 2008: since then 4% rise • 28% of suicides had contact with MH services in previous year; ½ of these contact that week • Hanging in 2/3 men & > 1/3 women who die • Prevention: access to method, alcohol, services

RCPsych Manifesto Sept 12, 2014. The manifesto has six key asks: 1. Everyone who requires a mental health bed should be able to access one in their local NHS Trust area, unless they need specialist care and treatment. If specialist care is required, then this should be provided within a reasonable distance of where the patient lives. 2. No-one should wait longer than 18 weeks to receive treatment for a mental health problem, if the treatment has been recommended by NICE guidelines and the patient’s doctor. 3. Everyone experiencing a mental health crisis, including children and young people, should have safe and speedy access to quality care, 24 hours a day, 7 days a week. The use of police cells as ‘places of safety’ for children should be eliminated by 2016, and by the end of the next Parliament occur only in exceptional circumstances for adults.

…/ RCPsych manifesto 4. Every acute hospital should have a liaison psychiatry service which is available seven days a week, for at least 12 hours per day. This service should be available to patients across all ages. Emergency referrals should be seen within one hour, and urgent referrals within five working hours. 5. A minimum price for alcohol of 50 p per unit should be introduced. This will reduce the physical, psychological and social harm associated with problem drinking, and will only have a negligible impact on those who drink in moderation. 6. There should be national investment in evidence-based parenting programmes, in order to improve the life chances of children and the well-being of families.

CMO Report • “more accurate data”, “more research needed” • Some use in collecting well-being data • Questions Rose hypothesis: “better well-being leads to less mental disorders” • Advising commissioners NOT to invest in wellbeing promotion unless (new) evidence • Recommendations limited or obvious (data and training) but highly quotable text

Where else should we go? • Some role in MH Promotion: Director of Public Education → Director of Public Engagement • Until recently, www. rcpsych. ac. uk was the number 2 site (to APA) for MH information • By speciality (MH cannot be ageless), MH prevention: primary “vague”; secondary = EI • Branding: gen hosp / “liaison” psychiatry, psychological medicine, EI in a general hosp

Older adults • Specialist MH services: <65 16% of population, >65 34% of this age group use these services • Multimorbidity, poorer outcomes, less £ • Depression in 10 -20% of community >65, but 20 -30% of gen hospital / care home >65 • Older people in general hosp: 1/5 delirium, 2/3 have a treatable MH disorder… RAID investment • To achieve parity with 35 -55 y. o. +24% increase
 >50% mortality")
Smoking cessation Now 18% smoking rates, England Anti-smoking messages work (middle class) >50% mortality differences rich / poor = cigs THESE ARE GETTING WORSE… NHS smoking cess reverses these inequalities People with SMI just as likely to quit cigs BUT programmes will have to be brought to them • Possible TCO = Tobacco Company Obligation • • •

Are new things always good? PRO e. Cigarettes (think of a Nuclear conflict, and a conventional war seems rather nice) ANTI / Caution e. Cigarettes • Significant uptake among young / new “vapers” • Rising use in ex-smokers • Flavours, marketing • Far less carcinogens • Big tobacco investing • e. Cigs help people quit, but • Facilitate nicotine delivery most “vapers” still smoke and therefore addiction • Not seen as treatment • Second hand smoke less bad • Nicotine harmful in preg, might also be carcinogenic • Public attitudes: want same ban in public places • Other drugs delivered…



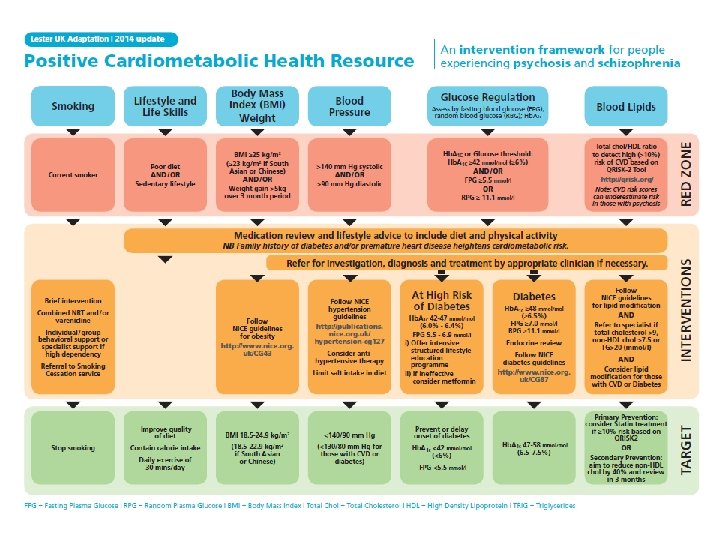
Stolen years • The ultimate case for Parity of Esteem is that our patients with SMI die 15 -20 years early • We know it’s Inequalities + cigs / alcohol • Final common pathway: cardiovasc disease, cancer, victims of violence, untreated disease • Medical response: can’t someone else do it? • Evidence is there already: cigs; min pricing; safer prescribing of APs; Lester Adaptation

PMH: conclusions Promotion, Prevention, Treatment Big 4: our services, stolen years, alcohol, EI Get Psychiatry’s (& specialities’) voice heard Opportunities to engage new people, ££s Hardest bits: inequalities, stigma, people at the margins - collaborate to advocate • Talk to us: lthorpe@rcpsych. ac. uk peter. byrne@eastlondon. nhs. uk • • •
- Slides: 36