Public Health in Scotland 2016 Early Clinical Career

Public Health in Scotland 2016 Early Clinical Career Fellowship Masterclass 31/08/2016 Pauline Craig Head of Population Health
")
Outline • Nursing to public health – a career pathway (or crazy paving? ) • What IS public health? – Theory, practice and priorities • The public health workforce in Scotland – Where does nursing fit? – What does it mean to me?

Our vision and mission Our Strategy 2012 -17: “A FAIRER HEALTHIER SCOTLAND”
 working with public,")
NHS Health Scotland • Small national Health Board (c. 280 employees) working with public, third and private sectors to reduce health inequalities and improve health http: //www. healthscotland. com/ • Our main focus is on knowledge into action for influencing and implementing policy, planning and practice. We are also known for public facing health information (eg screening, Ready, Steady Baby, smoking cessation etc) • We are developing a new strategy for 2017 -2022, building on AFHS and human rights, and within the context of the recent public health review

NHS Health Scotland Chief Execs Office Gerry Mc. Laughlin Public Health Sciences Andrew Fraser - Evaluation -Evidence for Action - Public Health Observatory (Scot. PHO) - Scot. PHN - Knowledge Services Health Equity George Dodds - Population Health - Place and Equity - Learning and Improvement - Marketing and Digital Services Health and Work Steve Bell - Fit For Work - Healthy Living Award - Employee Health, safety and wellbeing Strategy Cath Denholm - Strategy and Communications - Performance, People and Planning

What is public health? • ‘the science and art of preventing disease, prolonging life and promoting health through the organised efforts of society’(Acheson 1988) • Population based, multidisciplinary • Collective responsibility across the state, ie beyond healthcare • Determinants of health as well as disease: health and well being, more than absence of disease • Key figures from C 19 UK history: Edwin Chadwick (Poor Laws and sanitation reform); John Snow (Broad Street Pump); Florence Nightingale (social causes of death, hospital reforms)
 three key domains • Health improvement: population surveillance, housing")
Faculty of Public Health (FPH) three key domains • Health improvement: population surveillance, housing and education etc, lifestyles, health inequalities (NHS Health Scotland) • Improving services: need, efficiency, audit, governance, equity (NHS Boards, Scottish Public Health Network, Information Services Division) • Health protection: infectious diseases, environmental health, emergency responses (Health Protection Scotland; Information Services Division) • Underpinned by workforce: Standards, education, training, development (Faculty of Public Health, NHS Education Scotland, NHS Health Scotland; Professional Organisations – RCN, Re. HIS)

FPH standards based on nine key areas • • • Surveillance and assessment of the population's health and wellbeing Assessing the evidence of effectiveness of health and healthcare interventions, programmes and services Policy and strategy development and implementation Strategic leadership and collaborative working for health Health Improvement Health Protection Health and Social Service Quality Public Health Intelligence Academic Public Health

Science and art • Epidemiology: biomedical science, incidence and distribution of disease and factors relating to health • Needs-based, effective and high standard services • Environmental health: communicable diseases, chemicals, air quality • Social determinants: poverty and income inequality, power and disadvantage, housing, education, green space, food, culture • Curiosity, influencing, advocacy, driving change, leadership, vision

Examples from health improvement practice • Developing new knowledge and understanding • Knowledge into action • Social change

Determinants of health
 Source: Mok PLH, Kapur N, Windfuhr K, et")
Age-standardised suicide mortality (15 -44 y) Source: Mok PLH, Kapur N, Windfuhr K, et al. Trends in national suicide rates for Scotland for England & Wales, 1960 -2008. British Journal of Psychiatry 2012; 245: 245 -51.

All cause death rates, men 0 -64 y, 2001 Glasgow City Inverclyde West Dunbartonshire Dundee City Eilean Siar North Ayrshire Renfrewshire North Lanarkshire Source: Alastair H Leyland, Ruth Dundas, Philip Mc. Loone & F Andrew Boddy. Inequalities in mortality in Scotland 1981 -2001. Glasgow, MRC SPHSU, 2007.

Males - 75. 8 y Females - 83. 1 y Hillhead Jordanhill St George’s Cross Buchanan Street Hyndland Partick Exhibitio n Centre Charin g Cross Anderston Argyll St. Govan Ibro x Cessnoc k QUEEN STREET CENTRA L Bridgeton St Enoch Males - 61. 9 y Females - 74. 6 y Life expectancy data refers to 2001 -05 and was extracted from the Glasgow Centre for Population Health community health and wellbeing profiles. Adapted from the Strathclyde Partnership for Transport travel map. Source: Mc. Cartney G. Illustrating Glasgow’s health inequalities. JECH 2010; doi 10. 1136/jech. 2010. 120451.

Alcohol-related mortality* rates per 100, 000 population, 1950 -2006 Source: Updated from Leon & Mc. Cambridge (2006) *as indicated by liver cirrhosis

Upstream Downstream Alcohol Brief Interventions Minimum Unit Pricing Multi-buy discount ban Improved labelling Public Health objective Duty rises/falls National indicator / SOA Increased investment for T&C

The Framework for Action • Recognition that alcohol misuse was a population problem • Move towards outcomesbased approach to formulate evidence-informed policy • Whole population approach to reducing alcohol consumption and related harms • Importance of price and availability recognised • Move towards better data collation
")
Source: Scottish Schools’ Adolescent Lifestyle and Substance Use Survey (SALSUS, 2013)

Defining the Problem Recorded Crime in Scotland 16000 14000 Number of Crimes 12000 Non Sexual Crimes of Violence 10000 8000 Handling an offensive weapon 6000 Sexual offences 4000 2000 0 2003 -042004 -052005 -062006 -072007 -082008 -092009 -102010 -112011 -122012 -13

Adverse Childhood Experiences Troubled Families - Average 9 problems. 40% had 3 or more children Aged 18 to 69 (n = 3, 885) Bellis et al, BMC Medicine, 2014

Successes and challenges for public health in Scotland

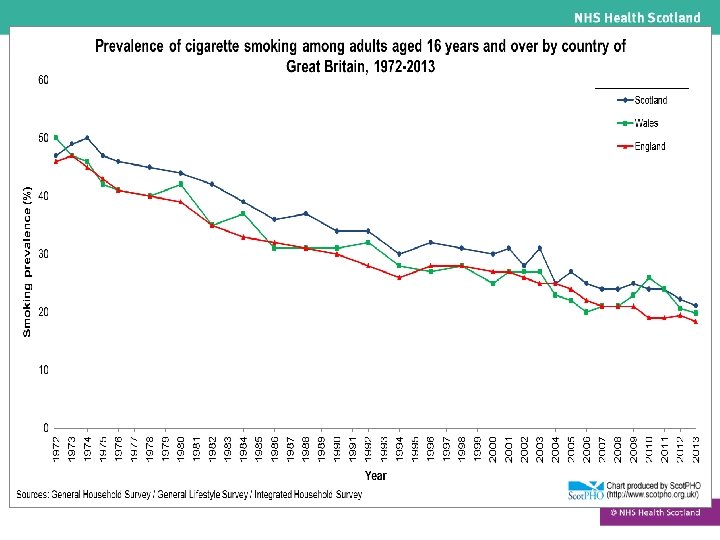
We can build on success – these have been life changing improvements over the last 50 years. These 4 ‘waves’ - lots of success in Scotland For example we have seen: • Roll out of successful immunisation and screening • Reductions in premature mortality from CHD, respiratory disease, stroke • Improved cancer survival rates • Marked reduction in tobacco use • Recent reduction in suicide rate • Recent reduction in risk behaviours among young people

The most pressing challenges of the next decade • Focusing upstream on prevention to reduce high levels of preventable mortality and multimorbidity in the future. • Helping everyone stay well for as long as possible whatever their current state of health. In particular, ensuring the best start in life and increasing the number of years in good health for our poorest citizens. • Addressing recent trends in over-consumption, inactivity and obesity which have the potential to overturn recent gains in life expectancy and healthy life expectancy. • Giving attention to mental health and wellbeing which can affect life chances and often coexist with physical health problems. • Continuing to address Scotland’s challenge with harmful alcohol consumption and continuing our efforts on tobacco control to reduce smoking further. • Ensuring collective, cross-government and cross-sector effort focussed on prevention.

People in public health

Public health structure in Scotland • NHS based specialist function: 14 regional Boards, each with a DPH, handful of consultants and sometimes a few public health specialists and health protection nurses. Management or connection with health promotion/health improvement. Four of the eight national Boards have or include a public health function: HS, NSS, NES, HIS • Core workforce in NHS eg information specialists and analysts, PH pharmacists, health improvement, research and evaluation etc; also local authority and voluntary sector staff eg physical activity, food etc, also practitioners with PH roles eg HVs. Could be in local services or partnership structures, with and without a professional home (eg HVs vs analysts) • Wider workforce in NHS: GPs, nurses, midwives, AHPs; other public sector, third sector, academics, scientists, lawyers, police, fire and rescue etc
: – – Directors, consultants and")
Scottish Public Health Workforce • PH workforce includes (arguably): – – Directors, consultants and specialists in PH Scottish Government health policy staff PH in titles (eg PH nurses, specialists etc) PH in day jobs but not in titles (eg HVs, Health promotion/improvement officers, programme managers in special boards, researchers, multiple skills required for rural areas etc) – ‘wider PH workforce’ eg nurses, midwives, teachers, social workers, Board chairs, community volunteers

Findings Directors of public health, Intelligence and knowledge consultants, specialists and specialist professionals trainees 370 -660 189 Directors of Public Health [18] Health Visitors 2, 185 Public Health academics 360 School nurses 500 Public health managers and practitioners 970 Public Health nurses (TB, inf control etc) 640 Public health academics 360 Environmental health professionals 980

What does all this mean to me? • In current role • As a contributor to the public’s health • Something to find out more about • Something to leave to others
- Slides: 30