Puberty in males and females Dr Najwa Abdur

Puberty in males and females Dr. Najwa Abdur Rashid

Objectives At the end of the lecture student should be able to : • Describe puberty and hormonal changes occurring during puberty in males and females • Describe the tanner staging for pubertal development • Describe types of puberty and its causes • Describe the abnormalities associated with hormonal changes in male and female • Describe the menopause and the changes which occur at this time

Puberty Onset of adult sexual life. Period when endocrine and gametogenesis functions of gonads have developed to the point where reproduction is possible. • Accelerated somatic growth • Maturation of primary sexual characteristics (gonads and genitals) • Appearance of secondary sexual characteristics • Beginning of Menstruation and spermatogenesis

Puberty – Terms & Events • • Thelarche: development of breast Puberache: development of axillary & pubic hair Menarche: the first menstrual period Adrenarche: the onset of an increase in the secretion of adrenal androgens – It occur at 8 -10 year in girl – 10 -12 year in boys – This rise is because of 17 -alpha hydroxylase

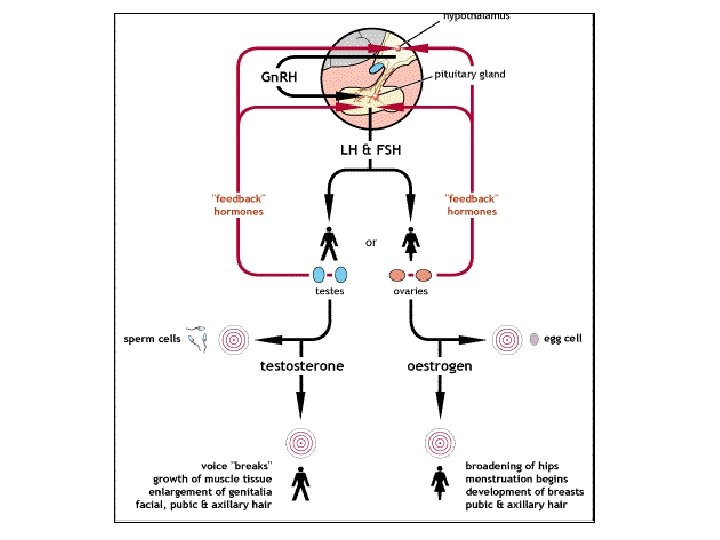
Hormonal changes • In young children, LH and FSH levels insufficient to initiate gonadal function • Between 9 -12 yrs, blood levels of LH, FSH increase • high levels of LH, FSH initiate gonadal development Hormonal changes precede physical changes Increased stimulation of hypothalamo-pituitary-gonadal axis – gradual activation of the Gn. RH – gonadotropins stimulate secretion of sexual steroids (estrogens androgens) – extragonadal hormonal changes (elevation of IGF-I, leptin, steroids) • GH secretion from pituitary also increases • TSH (thyroid stimulating hormone) secretion from pituitary increases in both sexes: – increases metabolic rate, promotes tissue growth

Hormonal changes

Puberty in Male • LH and FSH release increases ~10 yrs of age • Prostrate gland enlarge under the influence of testosterone. Grows till 50 yrs. • In boys, testicular enlargement is the first physical manifestation • of puberty (Gonadarche). • Testes in prepubertal boys has a volume less than 4 ml • Testicular size of 20 -25 ml average adult size • By the end of puberty, adult males have heavier bones • The rate of muscle growth, is attained about one year after a male experiences his peak growth rate. • By the age of 40 -50 yrs male sexual function decreases- male climacterics

Abnormality of male sexual function Prostrate abnormalities • Prostatic fibroadenoma can occur in older males. This hypertrophy is not because of testosterone but abnormal growth of fibrous tissue. • Prostrate cancer- 2 -3% male death • It is inhibited by removal of testis or by estrogen therapy Hypogonadism in male Male fetus testis are nonfunctional, no male sexual characteristic develop. A state of eunuchism in which he continues to have infantile sex organ and characteristics Slightly higher height because bone epiphyses is slow Muscles are weak Voice is child like

Abnormality of male sexual function Hypogonadism in male • If testis is castrated after puberty then some of secondary sexual characteristics revert to those of child. • Sex organ regress slightly , voice also but not child like • Erection is normal but no ejaculation • In some instance it can be genetic inability of hypothalamus to secrete normal Gn. RH • Associated with feeding center abnormality causing to overeat. This is called adiposogenital syndrome or hypothalamic eunuchism Testicular abnormality and hypergonadism Leydic cell tumor develop in rare cases Causing short height and excessive development of male sex organ

Puberty in Females • Breast development is the first sign of puberty • surge of LH release initiates 1 st ovarian cycle • usually not sufficient to cause ovulation during few cycle-anovulatory • Estrogen levels in blood increase • Estrogen induces secondary sex characteristics: – growth of pelvis – Increase in BMI – Increase deposition of subcutaneous fat – growth of internal reprod. organs, external genitalia • Androgen release by adrenal glands increases
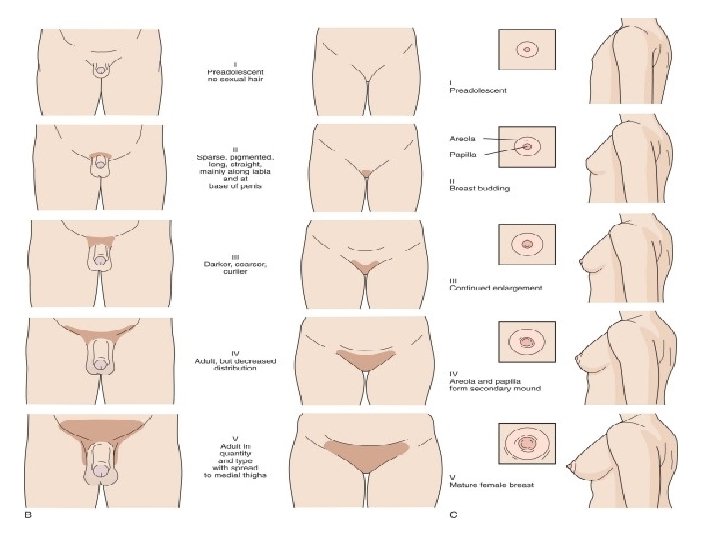
 Pubertal development is classified according to the Tanner standard")
Staging of pubertal development (Tanner) Pubertal development is classified according to the Tanner standard – 5 different stages Girls: • breast (B 1 -5) • pubic hair (Pu 1 -5) • axillary hair (A 1 -5) Boys: • testicular volume > 4 ml (Te) • penis enlargement (G 1 -5) • pubic hair (Pu 1 -5) • axillary hair (A 1 -5),

Normal pubertal development

Tanner scale I-Preadolescent no sexual hair II- Sparse, pigmented, long, straight, mainly along labia and at base of penis III-Darker, coarser, curlier IV- Adult, but decreased distribution V- Adult in quantity with spread to medial thighs

Tanner scale I-Preadolescent II-Breast budding II-Enlargement, change in texture III-Continued Enlargement III- Growth in length and circumference IV-Areola and papilla form secondary mound V-Mature female breasts IV-Further development of glans penis, darkening of scrotal skin V-Adult genitalia

Timing of Puberty • Critical body weight must be attained before activation of the reproductive system • Even though age of menarche is decreasing, the average body weight of menarche remains the same • Earlier puberty due to improvement of nutrition, living conditions, healthcare • evidence supporting hypothesis: – obese girls go through early menarche – malnutrition is associated with delayed menarche – primary amenorrhea common in lean female athletes – “bodyfat” setpoint very noticeable in girls with fluctuating body weight due to anorexia nervosa

Abnormal secretion of ovaries Hypogonadism Less secretion, abnormal ovaries or lack of ovaries If they are absent from birth or nonfunctional before pubertyeunichism Secondary sex characteristic does not occur and sex organ is infertile Long bones, very tall When ovaries are removed than organ regress, uterus become infantile, vagina become smaller, pubic hair decline, breast atrophy Irregularity of menses or amenorrhea Lack of estrogen or hypothyroidism can result in irregular cycles or absence of cycle

• Primary amenorrhea- never occurred because of failure of sexual maturation • Secondary amenorrhea- cessation of menstrual in a woman who previously has normal and regular cycle • Causes- hypothalamic disease, pituitary disorder, primary ovarian disorder, emotional stimulus, change enviornment • Hypomenorrhea- scanty menstruation • Menorrhagia- abnormal flow • Metrorrhagia-bleeding between periods • Oligomenorrhea-reduced frequency of periods • Dysmenorrhea- painful menstruation Hyper secretion of ovaries Rare clinical entity A rare granulosa tumor may develop after menopause which has estrogenic effect- hypertrophy of uterine epithelium development and irregular bleeding

Pubertal disorders Precocious puberty Precocious onset of puberty is defined as occurring younger than 2 SD before the average Girls <8 years old Boys <9 years old Gonadotrophin-dependent (true / central 85 -90% cases) Early but otherwise normal pubertal pattern of gonadotropin secretion from pituitary Premature pubarche/ Adrenarche and premature thelarche are two common, benign, normal variant conditions that can resemble precocious puberty but are non progressive or very slowly progressive Gonadotrophin-independent (peripheral/peudo 10 -15% cases) Early development of secondary sex characteristic without gametogenesis caused by abnormal exposure of immature males to androgens or females to estrogen
 • Constitutional – no cause can")
Gonadotrophin-dependent precocious puberty • (true / central ) • Constitutional – no cause can be determined. More common in girls • tumours or infection involving hypothalamus

• A definitive diagnosis of central precocious puberty may be confirmed by measuring LH and FSH levels 30 -60 minutes after stimulation with gonadotropin-releasing hormone (Gn. RH). • An increase in LH levels is diagnostic of central precocious puberty • If no increase in LH and FSH levels after the infusion of Gn. RH suggests precocious pseudo puberty

Gonadotrophin-independent precocious puberty • Peripheral/ pseudo • Precocious steroidogenesis or gametogenesis can occur without pubertal pattern of gonadotropin secretion • Sensitivity of LH receptors to gonadotropins is increased

Delayed puberty Initial physical changes of puberty are not present by age 17 years in girls (primary amenorrhea at 15. 5 -16 y) or testicular development by age 20 years in boys • Absence of breast development by the age of 13 years in girls or in a boy testicular volume of less than 4 ml by age of 14 years • Abnormal pubertal development due to functional or structural deficiencies of the hypothalamic-pituitary-gonadal (HPG) axis which is in most of cases

Causes of delayed puberty Chromosomal abnormalities causing gonadal dysgenesis (ovarian insufficiency due to the premature depletion of all oocytes and follicles) – 50 % ●Hypothalamic hypogonadism including functional hypothalamic amenorrhea – 20 % ●Absence of the uterus, cervix and/or vagina, müllerian agenesis – 15 % ●Transverse vaginal septum or imperforate hymen – 5 % ●Pituitary disease – 5 %
 – Turner’s Syndrome – Klinefilter’s")
Causes of delayed puberty • Gonadal failure (Hypergonadotrophic hypogonadism) – Turner’s Syndrome – Klinefilter’s syndrome • Gonadal deficiency – Congenital hypogonadotrophic hypogonadism Hypothalamic/pituitary lesions (tumours, post-radiotherapy) – In 70% patients adenoma of pituitary has elevated plasma prolactin levels. – Hyperprolactemia may cause galactorrhea – Prolactin may produce amenorrhea by blocking the action of gonadotrophin on ovaries.

Menopause At the age 40 -50 years Cessation of woman’s menstrual cycle It is preceded by period of irregular cycles and dwindling estrogen levels This loss of estrogen causes dryness of vagina irritability, fatigue, anxiety, sensation of dyspnea Skeleton (decrease bone density) Hot flushes, night sweats Negative feedback effect reduces causing increase FSH and LH level occasionally psychotic states Some estrogen are produced by adipose tissue, liver and adrenal cortex after menopause
- Slides: 27