PSYCHOSOMATIC MINDBODY MEDICINE Hamid Afshar MD Associate Professor
 MEDICINE Hamid Afshar MD. Associate Professor of Psychiatry Psychosomatic Research Center PSRC@mui.")
PSYCHOSOMATIC (MIND-BODY) MEDICINE Hamid Afshar MD. Associate Professor of Psychiatry Psychosomatic Research Center PSRC@mui. ac. ir

A holistic approach to medicine Relation between psychological factors and physiological phenomena in general and disease pathogenesis and illnesses in particular. Unity of mind and body Dynamic interacting systems

THE STRESS MODEL Stress disturbs or is likely to disturb normal physiological or psychological function. The body reacts to stresses (real, symbolic, or imagined); threatens an individual's survival by putting into motion a set of responses that seeks to diminish the impact of the stressor and restore homeostasis.
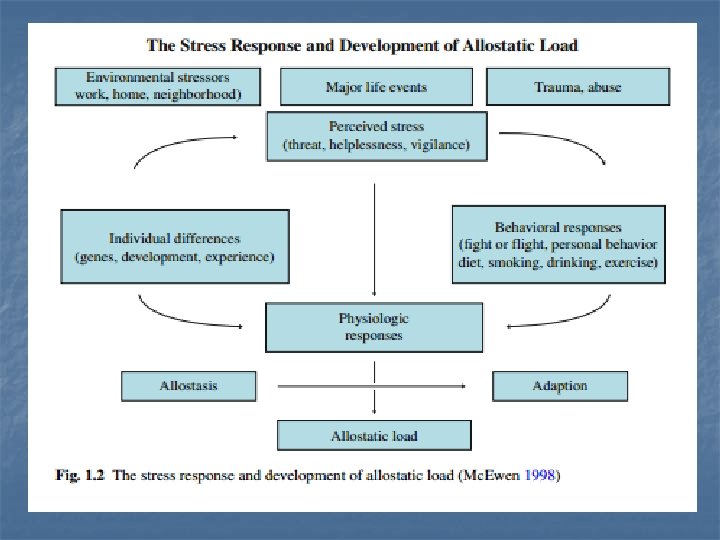

Endocrine Responses to Stress Two major facets of stress response: “Fight or Flight” response is mediated by hypothalamus, the sympathetic nervous system, and the adrenal medulla. If chronic, this response can have serious health consequences. The hypothalamus, pituitary gland, the adrenal cortex (HPA) mediate the second facet. CRF/ ACTH
 interleukin-1 (IL-1) and IL-6. These")
Immune Response to Stress Immune activation release of (cytokines) interleukin-1 (IL-1) and IL-6. These cytokines release of CRF increase glucocorticoid effects and thereby self-limit the immune activation. High level of Cortisol results in suppression of immunity which can cause susceptibility to infections and possibly also in many types of cancer. Psycho-Neuro-Immunology
 The link between the Nervous System, the Immune System and Behavior")
Psycho-Neuro. Immunology (PNI) The link between the Nervous System, the Immune System and Behavior The Nervous System (Neurobiology) Behavior (Psychology) Weintraub, 2007 PNI The Immune System (Immunology)

Functional somatic syndromes by specialty

Cardiovascular System Psychological factors have been closely studied as part of the pathogenesis of the cardiovascular diseases. Depression is an independent risk factor for the development of coronary artery disease. Depression increases mortality rates following myocardial infarction (MI). Hyperactivity of (HPA) , immune activation with release of proinflammatory cytokines, and activation of the sympathetic nervous system and of corticotropin-releasing factor (CRF) pathways in the central nervous system (CNS).

Gastrointestinal System Functional disorders represent 50% of complaints in GI clinics There is a strong & consistent association between functional gastrointestinal disorders and psychological factors Irritable Bowel Syndrome Brain-Gut axis Hypersensitivity of GI tract Role of stress

Somatic symptom disorder n A. One or more somatic symptoms that are distressing and/or result in significant disruption of daily life. B. Excessive thoughts, feelings, and behaviors related to these somatic symptoms or associated health concerns: At least two of the following are required to meet this criterion: (1) Disproportionate and persistent concerns about the medical seriousness of one’s symptoms. (2) High level of health-related anxiety (3) Excessive time and energy devoted to these symptoms or health concerns n n C. Chronicity: Although any one symptom may not be continuously present, the state of being symptomatic is chronic (at least 6 months).
: predominantly with pain complaints. individuals presenting")
n n n Predominant Pain* (previously pain disorder): predominantly with pain complaints. individuals presenting Persistent: A Persistent course is characterized by severe symptoms, marked impairments, and long duration(>6 mo). Severity: Mild (only one symptom with criterion B …) – Moderate (two or more with criterion B) –Severe(two or more in Critrion B plus multiple somatic complaints ) *Patients with other presentations of pain may better fit ; adjustment disorder psychological factors affecting a medical condition depressive disorders
 n Neurological symptoms / regardless appropriate medical")
Functional Neurological Disorder ( Conversion disorder ) n Neurological symptoms / regardless appropriate medical assessment/ incompatible with a neurological condition: weakness or paralysis, events resembling epilepsy or syncope, abnormal movements, sensory symptoms (including loss of vision and hearing), or speech and swallowing difficulties. n n n The symptoms may be acute or chronic. Psychological stressors or personally meaningful life events may often be associated with onset of symptoms, but their identification is not necessary for the diagnosis. Co-morbid neurological disease may also be present and does not exclude the diagnosis.

Criteria A, B, C and D must all be fulfilled to make the FND diagnosis: n n A. One or more neurologic symptoms such as altered voluntary motor, sensory function, or seizure-like episodes B. The symptom, after appropriate medical assessment, is not found to be due to a general medical condition, the direct effects of a substance, or a culturally sanctioned behavior. C. The physical signs or diagnostic findings are internally inconsistent or incongruent with recognized neurological disorder. D. The symptom causes clinically significant distress or impairment in social, occupational, or other important areas of functioning or warrants medical evaluation.

Illness worries are thoughts about illness or symptoms that make patient worry that he/she may be seriously ill.

Illness anxiety disorder n n A. Preoccupation with having or acquiring a serious illness. B. Somatic symptoms are not present or, if present, are only mild in intensity. If a general medical condition or high risk for developing a general medical condition is present, the preoccupation is clearly excessive or disproportionate. C. There is a high level of anxiety about health or having or acquiring a serious illness and the individuals is easily alarmed about personal health state. D. Excessive behaviors (e. g. checking one's body for signs of disease, repeatedly seeking information and reassurance from the internet or other sources), or exhibits maladaptive avoidance (e. g. avoiding doctor's appointments and hospitals, avoiding visiting sick friends or relatives, avoiding triggers of illness fears such as exercise).

n n E. Illness preoccupation has been present for at least 6 mo, but the specific illness that is feared may change over the time period. F. Not better accounted for by another mental disorder such as somatic symptom disorder, panic disorder, generalized anxiety disorder, or obsessive compulsive disorder or delusional disorder ( somatic type). Specify whether: Care seeking type Care avoidant type

DSM-IV Diagnostic Criteria for Psychological Factors Affecting Medical Condition A. A general medical condition (coded on Axis III) is present. B. Psychological factors adversely affect the general medical condition in one of the following ways: (1) the factors have influenced the course of the general medical condition as shown by a close temporal association between the psychological factors and the development or exacerbation of, or delayed recovery from, the general medical condition. (2) the factors interfere with the treatment of the general medical condition. (3) the factors constitute additional health risks for the individual. (4) stress-related physiological responses precipitate or exacerbate symptoms of a general medical condition.

Mental disorder affecting medical condition (e. g. , an Axis I disorder such as major depressive disorder delaying recovery from a myocardial infarction) Psychological symptoms affecting medical condition (e. g. , depressive symptoms delaying recovery from surgery; anxiety exacerbating asthma) Personality traits or coping style affecting medical condition (e. g. , pathological denial of the need for surgery in a patient with cancer, hostile, pressured behavior contributing to cardiovascular disease)

Maladaptive health behaviors affecting medical condition (e. g. , lack of exercise, unsafe sex, overeating) Stress-related physiological response affecting general medical condition (e. g. , stress-related exacerbations of ulcer, hypertension, arrhythmia, or tension headache) Other unspecified psychological factors affecting medical condition (e. g. , interpersonal, cultural, or religious factors)

Consultation Liaison Psychiatry The subspecialty of psychiatry that incorporates clinical service, teaching, and research at the borderland of psychiatry and medicine. Liaison refers to interactions with non psychiatrist physicians for teaching psychosocial aspects of medical care. knowledge of psychotherapeutic and psychopharmacological interventions

MODELS OF COMORBIDITY MEDICAL ILLNESS PSYCHIATRIC ILLNESS MEDICAL ILLNESS

TREATMENT FOR MEDICAL ILLNESS PSYCHIATRIC ILLNESS TREATMENT FOR PSYCHIATRIC ILLNESS MEDICAL ILLNESS SMOKING AND NICOTINE DEPENDENCE

Medical illnesses stress CLP Mind – Body interaction Psychological state Psychiatric disorders Somatoforms (somatic symptoms disorders) Health Functio nal disorders

MANAGEMENT Caring rather than curing Management is more realistic than treatment Therapeutic relationship Nature of symptoms in psychosomatic context Rule out depression and anxiety disorders Avoid investigations without indications Pharmacotherapy Coping skills Lifestyle changes
- Slides: 34