Psychosis and Early Intervention CBT for Psychosis CBTp
 DEVELOPED BY MANY PEOPLE WITHIN CNTW,")
Psychosis and Early Intervention CBT for Psychosis (CBTp) DEVELOPED BY MANY PEOPLE WITHIN CNTW, INCLUDING: GUY DODGSON, SONIA PACE, ANNA LUCE, ROB DUDLEY, AMONG OTHERS………. . Please do contact Dr Anna Luce (anna. luce@cntw. nhs. uk) if anything isn’t clear, you have questions, or you wish to discuss this further

What we aim to cover today Part 1: What is psychosis anyway? ! What ‘causes’ psychosis? Bio-psycho-social model (SVM) Part 2: Cognitive Behavioural Therapy (CBT) CBT for psychosis

Background: What is psychosis? Psychosis is an umbrella term meaning a break from reality Symptoms of psychosis include (“positive symptoms”): ◦ Hallucinations ◦ Hearing, smelling, feeling, tasting and seeing things that are not present (can be in any sensory modality – often multi-sensory) ◦ Delusions ◦ Holding (an unusual) belief based upon incorrect inference and firmly sustained despite widespread evidence to the contrary ◦ Thought disorder ◦ Highly disorganized pattern of thinking

Background: What is psychosis? “Negative” symptoms: ◦ Alogia: Impoverished thinking, thought blocking ◦ Anergia: Lack of energy or drive. ◦ Anhedonia: Difficulty in experiencing pleasure or enjoyment; Emotional Blunting; Difficulty experiencing or expressing emotion ◦ Difficulties in attention and concentration
: ◦ Schizophrenia: 1/100; ◦ Bipolar: 1/100; ◦ Schiz in")
Incidence and prevalence (estimates vary): ◦ Schizophrenia: 1/100; ◦ Bipolar: 1/100; ◦ Schiz in Mild LD: 3/100 (Turner, 1989) ◦ ‘Psychosis’: 3 in every 100 young people (more common than diabetes); higher among those with LD

But, is it that simple? ! • Surveys: 10 – 25% of the general population 1+ hallucinatory experience (Morrison et al. , 2008) • Over 80% of older people who lost their spouse had a visual or auditory hallucination (of their partner) in month following their death (Grimby, 1993) • 4 to 5 % of general population experience hallucinations during any one year period (equates to 3 million people in Britain and nearly 15 million in the USA) (Tien, 1991) • A survey of students reported some experiences of verbal hallucinations are not related to mental health problems (Posey & Losch, 1983) • Annual prevalence of psychotic symptoms in general population is 5% (Johns et al. 2004) - only one third are classed as ‘ill’

Hallucinations frequently occur in: • Sleep deprivation** • Drug & Alcohol use and withdrawal • High fever/infection/delirium • Impaired hearing or sight • Dementias • Depression • Trauma & dissociation • “Personality disorders” • Etc. • Solitary confinement / isolation • Spiritual practices • Lack of food • High levels of arousal / stress • Low levels of arousal • Bereavement • Borders of sleep; sleep disorders • Sensory deprivation • Epilepsy

Have you ever … • Heard your name called when there was no one there? • Heard the phone ring when waiting for it, only to find out that no one has rang? • Felt your phone vibrate, when no message? • Seen a loved one who has passed away? • Heard things whilst drifting off to sleep? • Heard something about you or seen people looking at you funny when anxious at a party? • Experienced anything like this when sleep deprived? (e. g. , breast pumps from hell!)? • Felt that people are talking about you or mean you ill?

What is a delusion? Karl Jaspers described 3 main criteria for a belief to be considered delusional: • Certainty: held with absolute conviction • Incorrigibility: not changeable by compelling counterargument or proof to the contrary • Impossibility or falsity of content: implausible, bizarre or patently untrue

BUT! • • • Musical tastes? Football fans? Political view points? Religious beliefs? Falling in love? BREXIT? !!!

AND………………. . Our beliefs are very changeable and highly biased • Affected by emotional state, especially fear I don’t believe in werewolves (rational scientist!) • Today (day-time, company): belief: 0% • Watching Werewolf in London at home with friend: 5% • Walking down a deserted forest path at midnight on night of the full moon, alone: ? 15% or more…when there’s a noise behind me? ! FEAR

And……. Unusual/unrealistic/”delusional”- type beliefs not just in psychosis: • Body image in anorexia? • Negative thoughts/beliefs in depression (“I’m completely useless at everything”)? • Over-estimation of threat/risk in anxiety problems (e. g. , concerns over infection in OCD; “heart attack” in panic) • Grandiosity in politicians?

Understanding suspiciousness/paranoia • Having suspicious thoughts is VERY common • Some level of suspiciousness is helpful and protective; suspicious thoughts can be a reasonable and sensible response to everyday life • However, suspicious thoughts can be unhelpful if they become too dominant or they’re out of proportion to (realistic) threat (‘paranoia’)
: o Familial links (10% parent versus 1%) o Age (young")
Risk factors (increase “vulnerability”): o Familial links (10% parent versus 1%) o Age (young adulthood) o Men > women (? ) o Inner city > Rural o Black Caribbean men (in the UK) o Trauma (Bentall et al. , 2012): traumas = 17 X more likely to have voice hearing “Causes” of psychosis: ? genetics ? biology ? psychology ? society

Common factors in development of distressing voices/psychosis Intense emotional distress Bereavement Sleep deprivation Isolation Substances Stress Traumatic experiences
 • Psychotic experiences relatively common among humans (not")
Understanding psychosis & schizophrenia (BPS, 2014) • Psychotic experiences relatively common among humans (not necessarily mental illness) • Certain life experiences make them more likely (esp. childhood adversity, trauma, stigma - Read, et al. , 2014) • Psychotic symptoms “make sense” in the context of peoples’ lives – e. g. , aggressive voice-hearing or suspiciousness after being bullied • Delusional beliefs often attempts to explain unusual experiences or emotions – e. g. , surveillance/technology; supernatural? • How person responds to unusual experiences important (fear, lack of control; “I’m going mad”; “the devil”)
 Normalising:")
So, what is psychosis? BIO-PSYCHO-SOCIAL MODEL Stress Vulnerability “Bucket” (Brabban & Turkington, 2002) Normalising: anyone could become psychotic Psychosis on a continuua of ‘normal human experience’

� � Vulnerability � Our vulnerabilities are things from our past that might make us more at risk/more sensitive to stress or becoming unwell They are (generally) things we can’t change, including: Genetics/biology Cognitive and mental abilities Early life experiences (ACES) Vulnerability factors? Size of bucket: Our capacity to manage stress

� � � Stress factors or ‘stressors’ are the factors that contribute to our stress in the present or immediately before becoming unwell: • They are (generally) variable/able to change • They can be acute e. g. bereavement, or chronic e. g. debt • Stress occurs in different spheres or areas of our lives • NB: They can be ‘positive’ events! • Stress factors? Amount of water flowing into bucket: stress (before illness)
 flow out")
Coping strategies Helpful ‘Holes’ in the bucket – let the water (stress) flow out Unhelpful ‘Corks’ in the bucket – stop the water (stress) flow out

� � ‘Helpful’ Coping e. g. , Talking about it! Getting sleep Healthy diet Exercise Keeping a sense of perspective Structured meaningful activity Approaching challenges Problem solving Seeking out support Rest and respite Hobbies / enjoyable activities ‘Unhelpful’ Coping e. g. , • Self harming • Alcohol / substance misuse • Avoidance of dealing with stresses • Isolation • Rumination • Worry • Self blame etc. IN FACT, having a flexible and varied response is best!!

So; what is psychosis? • Increasingly accepted that psychotic experiences are on a continuum with non-psychotic experiences • Difficulties arise when experiences/beliefs are distressing and/or interfere with daily life • How people make sense of/understand these experiences (particularly early on) is vital • Early intervention: provide normalising, benign explanations for unusual experiences/feelings (and offer ways to manage them) • Reduces FEAR and SHAME; increases sense of CONTROL

Explanations appear key! • Difference between ‘healthy’ voice hearers and those in services include service users feeling more afraid of their voices, voice content and feeling more powerless (Romme, 1992; Beavan, 2006; 2010). • ‘What makes voice hearers become patients is their reaction to their voices and the way they cope with underlying problems that have evoked the voices’ (Romme, 1992). • In a group of 80 voice hearing children, 85% were able to directly link onset of voices to a traumatic of stressful event (Escher, 2004).

Cognitive Behavioural Therapy What is CBT? What is CBT for psychosis?
 Recommendations: v Offer CBT to all patients with Psychosis Adequate")
NICE Guidelines (March 2014) Recommendations: v Offer CBT to all patients with Psychosis Adequate course - at least 16 sessions During acute phase or later (offer to patients with persisting positive/negative symptoms or in remission) v If PTSD symptoms evident offer trauma therapy v Plus family intervention v Plus access to MDT (medication, physical health, work support etc. )

Evidence Base: CBT for Psychosis However, debate around whether value of CBTp is overstated (Lynch, Laws & Mc. Kenna, 2009): ◦ Meta-analytic reviews small ES on psychosis symptoms measures ◦ Or no effect when compared to TAU or other active treatment There a number of possible explanations for the modest benefit of CBTp (Thomas, 2015): Any ideas? ◦ Recognition that CBtpis not as effective as would be ideal (Dudley, Turkington & Brabban, 2009)

Evidence Base: Interventions for Psychosis Small effect sizes are also found for medication 1 st & 2 nd generation antipsychotics, ES = 0. 3 to 0. 9 (Lepping et al. , 2011) Reduced further when high drop-out rates considered (See Lieberman et al. , 2005). Even Clozapine ES in small to medium range (Cohen’s d=0. 38, Moncrieff, 2003) Family Interventions medium to large
 •")
Cognitive models for psychosis • Cognitive Model for Hallucinations (Morrison et al, 2004) • Cognitive Theory of Delusions (Freeman et al, 2002) • Cognitive Model of Psychosis (Morrison et al, 2004) • Cognitive Model of Visual Hallucinations (Collerton and Dudley, 2004) • Adapted panic model! [For your reference - all provided at end of presentation]

CBT model based on Panic

Initial Stages Of Therapy Assessment • Problem list • Prioritisation of problems/goals • Potential for rapport • Review of symptoms, mental state • Risk/ traumatic events in childhood/adulthood • Support network/ medication/self medication
 CBT assessment • Antecedents, context • Affective, behavioural and")
Initial Stages Of Therapy (cont’d) CBT assessment • Antecedents, context • Affective, behavioural and cognitive consequences • Patient’s coping strategies/maintaining factors • Patient’s understanding of problems
 ◦ PANSS (Kay et")
Rating Scales Psychotic symptoms: ◦ PSYRATS (Haddock et al, 1999) ◦ PANSS (Kay et al, 1989) Specific/comorbid difficulties: ◦ BDI (Beck et al, 1961) ◦ BAI (Beck et al, 1988) Cognitive focus: ◦ Interpretation of Voice Inventory (Morrison et al, 2000) Qo. L/patient-focused ◦ Wellbeing (e. g. , WEMWEBS; NHS Scotland) ◦ Recovery (e. g. , QPR; Neil et al, 2007)

Initial Stages Of Therapy Engagement • Understanding patient’s experiences, and their model for their own problems • Why they believed what they believe(d) • Normalising rationale for symptoms • Stress-Vulnerability model (Zubin & Spring, 1977)
 Important in any therapy, but appears vital in psychosis, and can")
Engagement/therapeutic alliance (TA) Important in any therapy, but appears vital in psychosis, and can be particularly challenging as mistrust and suspicion is high: “TA has a causal effect on symptomatic outcome (PANSS) of a psychological treatment, and that poor TA is actively detrimental. These effects may extend to otherapeutic modalities and disorders” Goldsmith, (Lewis, Dunn & Bental, 2015)

Intervention focus Positive Symptoms: • Voice hearing • Visual hallucinations • Delusions Negative Symptoms: • Activity Scheduling • Social Skills Training • Art Therapy

Consider Is it necessary to directly address patients’ psychotic symptoms in order to reduce levels of distress and increase levels of functioning? Can this be achieved in other ways, such as directly addressing anxiety symptoms, which are often very prevalent in this client group? How do we work helpfully with those with very different understanding of their difficulties (including that they are not unwell)?

What are the Alternatives? • Treatment of co-morbid Depression/Anxiety (e. g. , Behavioural Activation/Graded Exposure) • Utilise psychological treatment approaches for disorders such as panic disorder, PTSD or OCD. • Formulate the difficulties of people with psychosis at the level of the person • Consider how “helpful” (or not) it is to view psychosis as “different” to other disorders! There are often more similarities than differences • Experience of using CBT with other client groups can be very helpful when working with psychotic patients (Morrison et al 2004)

Treatment of trauma Important difference between PTSD and Complex Trauma. Complex trauma is defined as experiences of prolonged and repeated trauma which might impact on a person’s affect, selfconcept, and relationships (Herman, 1992) People who experience complex trauma often report additional symptoms alongside formal PTSD symptoms, such as changes in their self-identity and the way they adapt to stressful events. NICE Guidance for PTSD (2005) - CBTt and EMDR recommended treatment.

Relapse Prevention • Normalising relapse • Identifying stresses/triggers • Reviewing formulation • Vulnerabilities • Early warning signs & WRAP Planning • Monitoring • Matching strategies to problems • Involving other people
 Dodgson: Three types of voice-hearing: •")
CBT for Auditory verbal hallucinations (AVH or “voices”) Dodgson: Three types of voice-hearing: • A) Inner speech • B) Intrusive memories • C) Hypervigilance All involve the brain misinterpreting either the source or the content of information
 Inner speech ‘voices’ occur when our own thoughts are misattributed as coming from")
a) Inner speech ‘voices’ occur when our own thoughts are misattributed as coming from an external source (rather than from our own minds; i. e. , “that’s not me!”) • Most voices are thought to be of this kind (80%) • Usually occur when we are on our own/quiet • Attention is internally focused • Can be long, complex (e. g. , ‘narration’, discussion) • Can assume ‘characters’ • Can become habitual

How inner speech develops Inner speech has the quality of a conversation – we are talking to ourselves. Vygotsky – Children are born into a very social world where they are having conversations with others. Over time, these conversations become internalised and become our “inner speech” – the things we say to ourselves in our own minds. Our inner speech will therefore be dialogic in nature – it goes two ways! We can see it in children when they are playing – they often play both “roles” in the dialogue.

Hearing own voice in our head sounds different • Can you hear their thoughts spoken in your head? • Does it sound like your spoken voice? • What is it like when you hear a recoding of your voice, is it as they imagine they speak? Learning point: Our internal and spoken voice sound different 43

Hearing a song in your head • Try to hear their favourite song in their head? • Does it sound like the record? Learning point: We can hear complex sounds in our mind 44

Getting a song stuck in their head • Do you ever get snippets of songs stuck in your head? • Do they just pop into your head (intrusive thoughts) Learning point: Things get stuck in our minds without conscious control. 45

Replaying an argument in their head and hearing the ‘others’ voice • Have you ever replayed an argument in your mind? • Does the other person sound like they did in the argument? Learning point: It is easy to hear other people’s voices in our mind. 46

In the argument, does the ‘other’ say new things • Have you ever lost one of these replayed arguments? • It is unlikely that you have because people change the script and put words into the mouth of the other person. • However, the replayed and new parts of the script sound the same. Learning point: We can make people we know ‘say’ things in our mind that they have not said. 47

Can they hear their own speech as Donald Duck? • If you have managed to change their inner speech, can maintain this for a few minutes? • Our inner speech is malleable and it is possible for it to become a habit to hear different voices in our head. • Eventually this does not require conscious effort. An example is when people can hear the ‘voice’ of a character when they are reading a book. Learning point: It is possible for us to hear our inner speech in a different voice without conscious effort, particularly if it becomes a habit to do this. 48

Our inner speech and voices o. Our brains are already primed and ready to talk in dialogue with itself (having a conversation with ourselves) o. There may be times when we no longer recognise this inner speech or inner dialogue as coming from our own minds o. It is thought that the “raw material” of auditory-verbal hallucinations is the voice-hearer’s own inner speech that is being misattributed to an external source (Jones & Fernyhough, 2007)
 Intrusive memories Steel, Fowler & Holmes (2003): Transfer ideas from models of PTSD")
b) Intrusive memories Steel, Fowler & Holmes (2003): Transfer ideas from models of PTSD • Trauma memories can be distorted, fragmented, inexact • Lack context (“time stamp”) and can be interpreted as happening “now” (not “then”) • May not be available to conscious recall Therefore, might some ‘voices’ (and/or or other types of hallucinations, e. g. , tactile, visual) be of this kind?
 Hypervigilance hallucinations occur when neutral external events are interpreted as personally meaningful and")
c) Hypervigilance hallucinations occur when neutral external events are interpreted as personally meaningful and threatening: • Usually when in large groups or outside OR when alone but in high arousal and hypervigilant state (actively listening out) • More frequent with background noise (e. g. , neighbours’ mumbling, electric fans, chatting) • Usually much shorter, one word or phrase repeated • Often something highly relevant to us personally and highly emotionallycharged for us (e. g. , our names, name-calling, judgemental) • Expectancy effect/top down processing

Asking about experiences § Interview e. g…. • When did you hear the voice for the very first time? • When do you hear the voice now? • Have you noticed any pattern to when you more likely to hear them? • What are you normally doing when you hear it? • Are they more likely to happen when you are alone or with other people? • Do they happen more or less when you are at home or outside? • Is voice hearing more likely when you are in bed? • How are you feeling when you hear the voice? • Anything that makes it better or worse? • What do you think when it happens? • Does the voice remind you of anything? • Do you have an idea of what the voice looks like? • Do you agree with or believe what the voice is saying?

Attention § Hypervigilance AVH: The focus is on external events (e. g. noises in the street; neighbours) § Inner speech AVH: Attention likely to be unfocussed with the mind ‘drifting’ so intrusive thoughts more likely § Memory-based AVH: Unclear at present – some suggestion that voices are a form of dissociative experiences – parts of the self that are cut-off as a result of trauma
, shame. § Inner speech AVH:")
Emotion § Hypervigilance AVH: Fear, anxiety (including social anxiety), shame. § Inner speech AVH: Sadness, shame, boredom § Memory-based AVH: Emotions that may ‘trigger’ memories.

Number of voices § Inner speech AVH: Usually same couple of voices. They can become complex ‘characters’ and may reflect previous relationships. § Memory-based AVH: Usually same couple of voices repeated. § Hypervigilance AVH: Multiple voices as linked to people in nearby space. Occasionally a constant voice, e. g. neighbour.

Content of the voice § Hypervigilance AVH: Content consistent with the anticipated/ looked for threat. Often short. § Inner speech AVH: May vary and can reflect thoughts that are unacceptable to the voice hearer; long utterances common e. g. running commentary. § Memory-based AVH: Repetitive content usually associated with past experiences. Often short.

Categorising voice hearing

CBT for visual hallucinations Categorising visual hallucinations
 are relatively common in psychosis (Waters et")
Current evidence base • Visual hallucinations (VH) are relatively common in psychosis (Waters et al. 2014) • They are associated with increased disability (Mueser et al. , 1990) • But we don’t know (much about) how to treat them! • There is limited evidence of medication being helpful specifically for VH (Dudley, Collerton, Nicholson & Mosimann. , 2013) • In terms of psychological therapies, the evidence base is also limited; early research into CBT for visions usingle-case research methods shows positive results (Wilson et al. 2015; Thomson et al. 2017)

Key principles to remember There a number of similarities to working with voice hearing and the similar key principles apply: Normalisation The role of expectancy in perception Considering what maintains our sensory experiences (brain plasticity) But when we consider our formulation of visual experiences we want to consider the source of the distress as central, and consider ways to challenge this or support individuals to develop coping strategies targeted at this. The main aim is not to “get rid” of or dismiss visual experiences… it is more about making sense of them and reducing distress

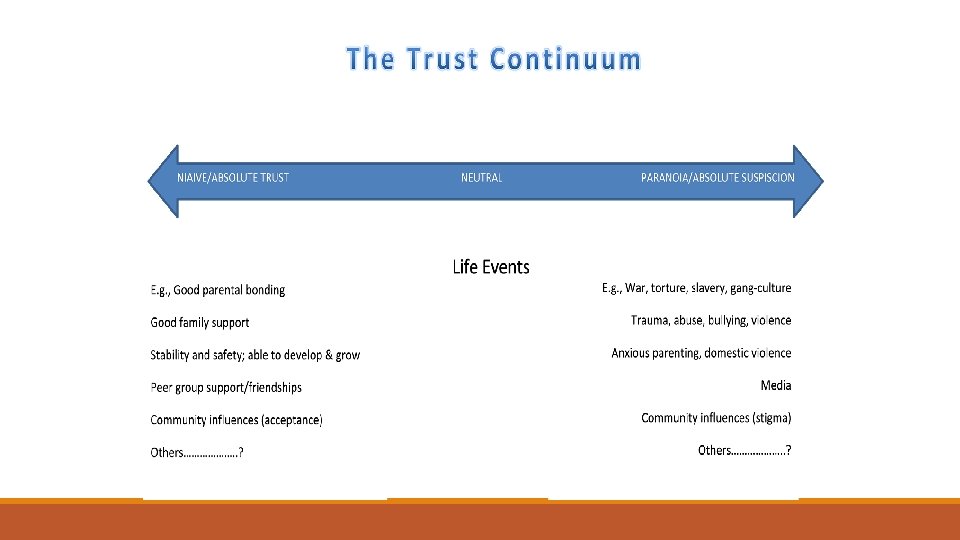
CBT for delusions • Identification of patients’ explanations for their delusions • Generate alternative (benign) explanations • Examine the evidence/identify biases • Reality testing • Trust Continuum (later) • Inference chaining

Unhelpful thinking styles/biases • Jump to conclusions • Ignore contradictory evidence • Hold their conclusions with greater conviction than people with culturally acceptable beliefs
 Emotional response")
Caveat to challenging delusions Importance of a feeling of safety (Freeman, 2016) Emotional response is based in reality, even if the explanation for it/the belief is not. Often there can be underlying feelings of shame. Challenging beliefs can be exposing and increase feelings of being “unsafe”. This is likely to prompt a counter-attack from the individual so that they can avoid emotional pain.

Other targets of therapy Living well despite beliefs Reducing shame, addressing trauma – PTSD and/or Complex trauma Managing emotions Improving ‘coping’ (reducing unhelpful coping strategies: avoidance, withdrawal, drug-use) Improving self-care/self-esteem Improving relationships Addressing ‘processes’ e. g. , worry or intolerance of uncertainty Re-engaging with society

“ 3 rd wave” CBT/other approaches Mindfulness Compassion-focused therapy “Relational” CBT Avatar therapy/VR trial Voice dialoguing Cognitive Analytic Therapy (CAT)

Normalisation via psychoeducation i. e. , challenging ‘catastrophic interpretations’

Psychoeducation/Normalisation Understanding how the mind/body works helps provide a benign explanations for voice hearing/psychotic experiences (which are human!), which can be understood, talked about, and managed/recovered from Challenges catastrophic misinterpretations: I’m mad, I’m being monitored; I’m being talked to by the devil, I’m weak and broken

Key concepts in psychosis psycho-education o This forms part of our normalisation and psychoeducation work. o We can offer non-threatening/benign explanations for experiences o Rather than “I’m mad, bad or weak”, “I was very stressed and stressed brains make mistakes”. o We can take a calm and curious stance (isn’t the brain amazing…and it makes mistakes!) o In it together: can we figure this out together o Offering hope (there are things we can try which others have found helpful)

Key ideas 1. The “old” and “new” brain Initiates our fight/flight response. Safety first. Emotional regulation and expression. Thinking brain. Planning, reflection, access to explicit memories. Can be hijacked by limbic system in event of real or imagined danger. Online from birth, regulates survival. Controls vital bodily functions, e. g. HR, breathing.

The “old brain” and threat § We have evolved to predict threat – immediate, physical threat. § When our brain perceives threat, our new brain switches off. § Even when we know that something isn’t real or true, our new brain cannot override the predictions of threat that our old brain makes. § Our old brain takes the approach that it is ‘better to be safe than sorry’, even at the cost of making mistakes to help us to survive! (It is better to see a bear that isn’t really there, than not to see a bear that is there!) § Modern life: most threats are SOCIAL (but response with old brain!) § OUR OWN THOUGHTS can become threats § DISSOCIATION

Key ideas 2. Emotions and thoughts §We all have a variety of weird and wonderful thoughts (and feelings) and can be random, disgusting and frightening §Thoughts are not wishes, and don’t necessarily reflect “our true selves” §Some thoughts pop into our heads unwanted and unbidden (“intrusive thoughts”) §If we have upsetting thoughts, it is natural to push them away (“thought suppression”); however, this makes a thought more frequent! §When we are feeling strong emotions, our thoughts become coloured by this emotion

Intrusive thoughts examples item hitting animals or people with car swerving into traffic slitting wrist/throat cutting off finger jumping off a high place fatally pushing friend jumping in front of train/car pushing family in front of train/car bumping into people insulting authority figure stabbing family member accidentally leaving heat/stove on home unlocked, intruder there taps left on, home flooded swearing in public breaking wind in public throwing something female % 46 55 20 19 39 9 25 5 37 34 6 79 77 28 30 31 28 male % 54 52 22 16 46 22 29 14 43 48 11 66 69 24 34 49 26
 “I’ve just remembered something awful/dangerous. I know!")
Intrusive thoughts - Suppression Old brain (fear) “I’ve just remembered something awful/dangerous. I know! I will generate a thought about this awful thing to warn the New Brain to take care (better safe than sorry!)” “I was right! I knew that thought was important – well, I know my job, I need to produce more of these thoughts!” “Proved right again! Those thoughts must be very important if New Brain is so desperate to get away from them. I BETTER MAKE SOME MORE” “The New Brain is really being affected by those thoughts, they have got to be very important indeed. I BETTER KEEP CHURNING THEM OUT!” New brain (judging) “Oh no! I have just had a horrible thought! This thought must mean something – it must be true. I need to stop having this thought or get rid of it somehow. THIS THOUGHT IS DANGEROUS!” “OH NO! Not more of those awful thoughts. I need to get away from them or avoid them or distract myself” “These awful thoughts won’t stop! What does it say about me to have these thoughts? I must be a bad person to have them. It must mean I am weak. ” AND SO ON………………. .

Key ideas 3. Our perceptual system is not 100% accurate Our brain’s make a “best guess” based on: ◦ The quality of the data/information in front of us ◦ Our past experiences and what we learned from them ◦ Our emotional state ◦ Sense of current threat

Only smart people can read this… 75

Brains make mistakes! § Brains “fill in the gaps” in order to make decisions about how to act quickly § Brains can make mistakes § ESPECIALLY when stressed, overwhelmed or overloaded. § Soldiers on operations or on exercise who are also sleep deprived usually accept that they are going to hallucinate!

Key ideas 4. Influence of attention § Our focus of attention can make a huge difference to what we perceive in the world around us §Awareness test: https: //youtu. be/Uf. A 3 iv. LK_t. E § Our emotions can shape our expectations – if we feel under threat, we might expect to see/hear something dangerous § We can miss lots of things because we do not expect them… § How might this relate to voice hearing?

Our expectations affect what we see and hear §We make predictions about what we are going see and hear all the time §Research suggests that our expectations (conscious and unconscious!) can influence our perception § Our experiences can influence what our brain “expects” and this can be imposed upon our perceptions. https: //youtu. be/G-l. N 8 v. Wm 3 m 0 - Mc. Gurk Effect https: //www. youtube. com/watch? v=0 ukn 2 YT 5 je. M – Peter Kay

Key ideas 5. Isolation/withdrawal When we are alone for too long, our brain can generate voice hearing experiences as we are designed to be in conversation with others. Combine this with sleep deprivation… https: //www. youtube. com/watch? v=0 nnekx. GE 0 n. M&index=2&list=P L 0 DCDF 28 C 82617678

Key ideas 6. Tracking the self It is easy to lose track of what belongs to us and what belongs to other people. It is therefore very natural, and human, for thoughts, feelings and sometimes even body parts to not feel like part of us. Rubber hand illusion: https: //www. youtube. com/watch? v=sxwn 1 w 7 MJvk Dissociation ****** If this is a normal human experience, what might this say about hearing voices that do not feel like part of us?

Key ideas 7. Neural networks § The brain has around 1 quadrillion connections between individual cells – also called “neural networks”. § We keep the networks we need and lose (or prune) the ones we do not. § The more the network gets used, the easier it is for this network to be activated – e. g. we are more likely to use a well-trodden path than one that has lots of bushes/branches in the way. § The more we think about something, the more we will think about it in the future.

Key idea 8. Beliefs and delusions • Unusual beliefs …………… • Unusual in context (others in same social/cultural group don’t share) • Held onto without evidence/in face of counter-evidence and likelihood/extreme • Cause high distress to individual or difficulties in getting on with their ‘normal’ life and relationships e. g. , paranoia: thinking that others are ‘out to get me’; behaviour: stop going out or seeing friends

What maintains suspicious thoughts? THOUGHTS: Believing our suspicions are true (e. g. , threatbased thinking styles): Good at noticing things that support that our suspicions are true Not good at noticing things that seem to contradict our suspicious thoughts Tending to jump to conclusions (‘better safe than sorry’; ‘false alarms’) Tending to jump to negative interpretation of events Not good at thinking through a range of possible explanations for events

What maintains suspicious thoughts? BEHAVING: As if my suspicions are true: Avoiding situations which make us feel threatened Avoiding others/reduced social contact (or casual contact with strangers) Difficulty ‘talking things through’ with others [no chance to find out if true or resolve problems] Keep ourselves to ourselves, not sharing our worries Don’t make friends

What maintains suspicious thoughts? FEELINGS: Anxious and down: Suspicious thoughts make us feel anxious and low in mood Spending a lot of time worrying Over-estimate threat Trying to prepare for danger (hypervigilance) Feel unable to make friends Feel unmotivated (because low) Depressed thinking (e. g. , dwelling, negative thinking) keeps us stuck Under-estimate our abilities
 of the harm or threat? Type")
Understanding suspicious thoughts Some areas for consideration: Perpetrator(s) of the harm or threat? Type of harm? Timing of the harm? Motivation or reason for the harm? What are the suspicious thoughts about? Who do they believe will harm them? How, when and why? How might they link with past experiences?

Understanding unusual thoughts Attempt to explain unusual or distressing experiences or physical sensations (e. g. , voices)? Attempt to explain or manage unusual or distressing thoughts? Attempt to explain or manage unusual or distressing feelings? What are the unusual thoughts about? How might they link with past experiences? What ‘evidence’ are they basing these on? What biases in thinking (e. g. , threat-based) might be going on?

http: //www. ted. com/talks/eleanor_longden_the_voices_in_my_head

General working with psychosis • Normalising and Psycho-education • Offer non-threatening/benign explanations for experiences (“I’m mad, bad or weak” to “I was very stressed and stressed brains make mistakes”) • Take the “heat” out of the system • Calm and curious (isn’t the brain amazing…and it makes mistakes!) • In it together: can we figure this out (your very frightening experiences) together • Hope (there are things we can try which others have found helpful)

Medical Investigations • Base on history • If any organic symptoms/signs consider EEG, MRI, NMDA/VGKC antibodies • Urine drug screen • For everyone: • Baseline bloods (including prolactin) • ECG if considering medication
 •")
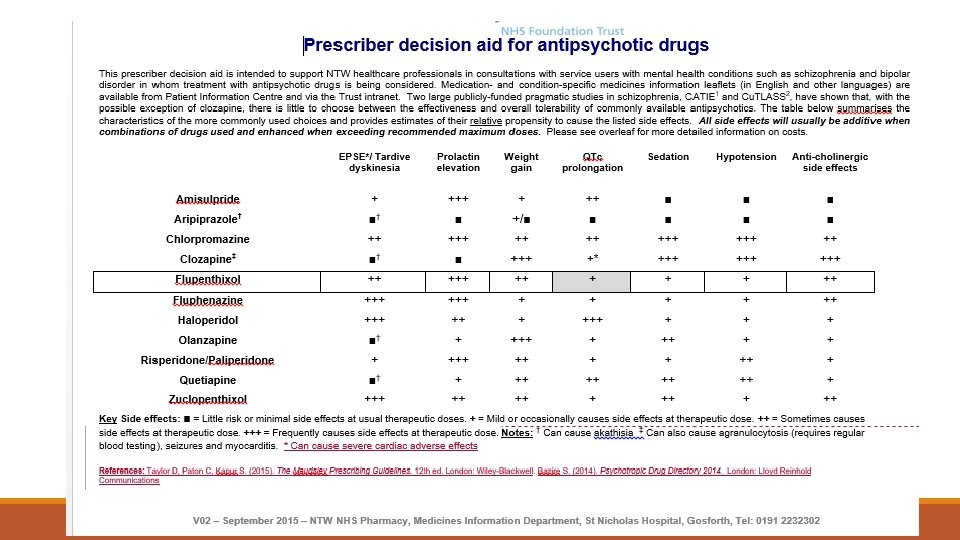
Antipsychotics: General principles • Second generation similar effectiveness (except clozapine and perhaps olanzapine) • Choose which side effects are least undesirable to patient (joint decision) • START LOW, GO SLOW • Avoid olanzapine (weight gain ++++) ◦ 11 kg weight gain in 24 weeks –worse in young people • Baseline monitoring plus regular physical health monitoring essential
 § Use benzos §Antipsychotic")
Prescribing §A period of antipsychotic free initial assessment (~7 days) § Use benzos §Antipsychotic medication for the treatment of FEP should be commenced by a specialist (or in consultation) §The patient should be included in the choice of antipsychotic medication and there should be documentation of this in the patient’s notes.

Prescribing Second generation antipsychotics should be used as first line treatment: ◦ Aripiprazole ◦ weight sparing antipsychotic ◦ prolonged prescription of antipsychotics sometimes induces changes in dopamine receptors, causing super-sensitivity, which could diminish the effectiveness of antipsychotic medication over time. ◦ Dopamine partial agonists may be less likely to do this.

Prescribing § Antipsychotic treatment should start at a low dose and be slowly titrated upwards within the dose range given in the BNF. § Patients should be treated with the lowest effective dosage to minimize adverse effects. § The use of combinations of antipsychotics is not supported by evidence and is associated with more adverse effects. § Up to 40% of those whose psychosis remits after a first episode should be able to achieve a good outcome in the long term either with no antipsychotic medication or with a very low dose.

Clozapine §If two individual antipsychotics do not provide adequate benefit, use Clozapine rather than combinations of antipsychotics. §For one third treated for psychosis, antipsychotic medications will have little or no therapeutic benefit. §Clozapine remains the sole medication approved for treatment-resistant schizophrenia, and studies have demonstrated its superior efficacy in reducing psychotic symptoms. §The use of Clozapine for treatment-resistant schizophrenia is underutilized, nationally and internationally ◦ In UK, mean time to first trial of Clozapine was 6. 7 years and the mean number of antipsychotics prescribed before Clozapine trial was 4. 85. ◦ Having a younger age at onset, lack of employment, a lower Global Assessment of Functioning disability score, and a higher Positive and Negative Syndrome Scale total score at baseline were factors associated with Clozapine use.

Physical health monitoring for young people on antipsychotics §Height and weight §Pulse and blood pressure §Bloods § Prolactin § Lipids § Glucose § Hb. A 1 c §ECG §Movement disorder/EPSE §Don’t just screen, intervene!

Any Questions?

Online resources “Understanding Psychosis and Schizophrenia” – British Psychological Society report, downloadable from http: //www. bps. org. uk/system/files/Public%20 files/rep 03_understanding_psychosis. pdf One women’s story: http: //www. ted. com/talks/eleanor_longden_the_voices_in_my_head www. hearing-voices. org www. intervoiceonline. org www. rethink. org www. aminormal. org www. healthtalkonline. org/mental_health/experiences_of_psychosis
 Trigger Auditory Hallucinations Mood and arousal Avoidance and")
CBT Model For Hallucinations (Morrison, 1998) Trigger Auditory Hallucinations Mood and arousal Avoidance and safety behaviours Catastrophic misinterpretations
 Paranoid beliefs are threat beliefs Generate")
Cognitive Theory Of Delusions (Freeman et al, 2002) Paranoid beliefs are threat beliefs Generate high levels of anxiety Meaning of different experiences Biases in psychological processing Explanation for experiences Delusional beliefs
 Cognitive biases associated with psychosis Jumping to conclusions/Attentional bias")
Cognitive Theory Of Delusions (Cont’d) Cognitive biases associated with psychosis Jumping to conclusions/Attentional bias Attributional bias Theory of mind dysfunction
 Intrusion into awareness (cognitive, body")
A Cognitive Model Of Psychosis (reproduced from Morrison, 2001) Intrusion into awareness (cognitive, body state, emotional or external information) Culturally unacceptable Interpretation of intrusion Beliefs about self, world, others (informational processing biases) Life experiences Cognitive & Behavioural responses Including negative symptoms (including safety behaviours, selective Attention and thought control strategies) Mood & Physiology (and negative symptoms)

Collerton and Dudley, 2004
- Slides: 109