Psychopharmacology in the classroom Jaclynn Lubbers DNP RN

Psychopharmacology in the classroom Jaclynn Lubbers, DNP, RN, CPNP Calvin University Holland Pediatric Associates, PLLC

Goals for today: Share my own personal experience with the use of medications in children with AD/HD and anxiety Share my professional knowledge regarding medications for AD/HD, anxiety, depression, and others Humbly collaborate with educators to improve the educational and health related trajectory of children and adolescents with these conditions…or how can we all work together? Answer questions

My story…why am I here today? • MSN 2000, began working in private practice as a PNP. • 2003 and 2006 we were blessed with two children • 2009 back to graduate school • 2010 -2011 -our son’s experience in school • 2012 -graduated, started teaching for Calvin • 2013 -2014 -our daughter’s experience in school • 2018 -2019 -revisiting our son’s diagnosis

Lack of Child and Adolescent Psychiatric Care: Midwest severe shortage https: //www. aacap. org/aacap/Advocacy/Federal_and_State_Initiati ves/Workforce_Maps/Home. aspx Provider view: The state of the healthcare system in 2019 Primary care providers are becoming the front line providers for child and adolescent mental health State of health plans-private insurance versus state funded planshigh deductibles, increasing copays State of reimbursement State of complex care management Challenges of coordinating care MAPS system/scoring

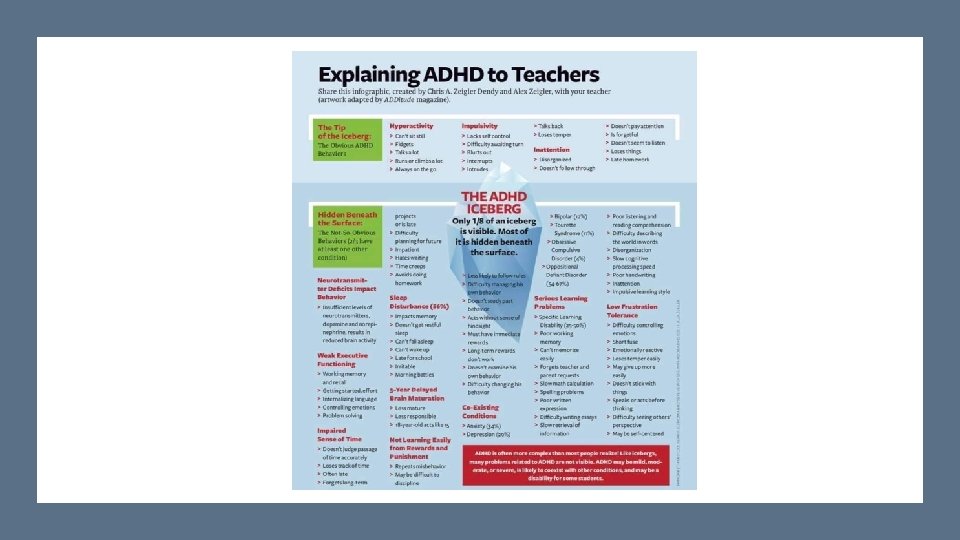
If only we could get kids to eat less sugar, we could solve the problem of ADD/HD. Two Truths and a Lie…. AD/HD represents a complex change in brain structure, function, and signaling. Properly diagnosing AD/HD requires the input of professionals from at least two of the child’s environments.

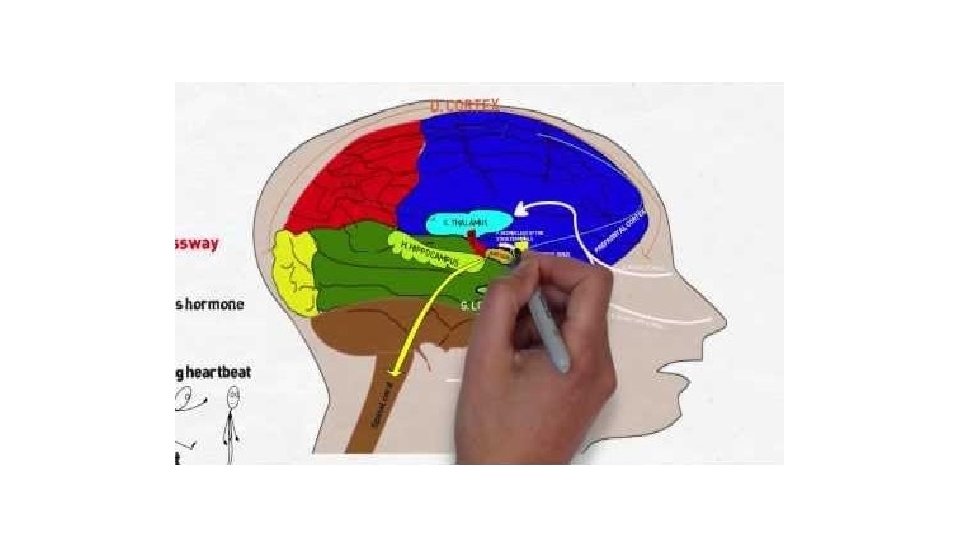
Brain function in ADHD…structure/function/signaling:

The “whole” scope of treating AD/HD:

The AD/HD Medications: Stimulants Methylphenidate: Amphetamine: “aka” Ritalin http: //www. adhdmedicati onguide. com/ Cotempla Adzenys (capsule and liquid) Concerta Metadate Effect size for stimulants is 1. 0 Focalin Quillavent (liquid) Daytrana (patch) Jornay (first nighttime medication) Adderall Vyvanse (chewable and capsule) Dexedrine Dynavel (liquid) Mydayis

The Stimulants: How do they work?

AD/HD Medications: the nonstimulants Norepinephrine reuptake inhibitor-Atomoxetineaka “Strattera”-Black box warning -Extended release guanafacine-”Intuniv” Alpha 2 adrenergic agonists: -Extended release clonidine Effect size for nonstimulants is 0. 7

How do the nonstimulants work?

Evaluation materials Making the diagnosis/starting treatment: Appointment Medication initiation Follow up appointments -choice of medication -dosage of medication -side effect management -role of medication

Height, weight, and blood pressure monitoring Provider view: the follow up is ESSENTIAL Effectiveness-Right med? Right dose? Duration of effect? -school feedback is especially helpful Side effect management -appetite suppression -sleep Comorbidity monitoring-depression, anxiety, obsessive compulsive disorder, suicidality, sleep disorders

Parent view: Process of obtaining stimulant medications for your child Initial evaluation Prescription Pharmacy visit Cost Insurance regulations Prescription regulations Having a child on stimulant medications is a part-time job!

Emerging evidence about brain changes on MPH-increased white matter in males especially An abundance of evidence that stimulant use in adolescents PREVENTS substance abuse Long term stimulant use: Tolerance/tachyphylaxis/addiction/dependence Growth concerns Dosage adjustments over time

Females > Males (males with AD/HD are more likely to have externalizing comorbities, females with AD/HD are more likely to have internalizing comborbities) Depression and Anxiety: as stand-alone diagnoses or as comorbidities to AD/HD Approximately 20% prevalence for depression by age 20 Up to 30% prevalence for anxiety during adolescence Universal Screening for depression using a standardized assessment tool, USPSTF, 2016

Depression and anxiety are also complex disorders of brain structure, signaling, and processing. Two truths and a lie: People with these diagnoses just need to “get over it” Suicide is the third leading cause of death among adolescents in the United States


Arise from brain structure, processing, and signaling dysfunction In short, both depression and anxiety: Treatment for both is similar: -mild -moderate -severe The use of Selective Serotonin Reuptake Inhibitors (SSRI) medications are the first line choice of pharmacologic treatment of these disorders.

Treatment for mild depression and anxiety: • Cognitive Behavioral Therapy or CBT • Dr. Aaron Beck • Treatment challengesinsurance, silos of care, “fit”, “buy-in” • Modes of delivery-area of study!

• SSRIs block the reabsorption of serotonin at the synapse • Serotonin is our “feel good” neurotransmitter • Most researched SSRI in children is fluoxetine (Prozac), this is the only SSRI to be approved by the FDA Mild and Moderate Depression and Anxiety: SSRI’s and how they work: • All SSRIs and SNRIs have a “black box” warning

Depression and Anxiety treatment: WRITING THE PRESCRIPTION IS THE EASY PART! SIDE EFFECT MANAGEMENT TEACHING MANAGING EXPECTATIONS IMPORTANCE OF THERAPY (TADS STUDY) CARE MANAGEMENT FOLLOW UP VISITS DURATION OF TREATMENT

Primary care depression treatment flowchart

Austic Spectrum Disorders: bringing the above diagnoses together, newer pharmacologic considerations Overall prevalence for anxiety with ASD is 42 -79% Greater than 50% of children with ASD have symptoms of ADHD Depression estimate for ASD are 1072%, but are more likely to present differently-insomnia and restlessness
, Risperdol (FDA), Seroquel, Zyprexa to name a")
Atypical Antipsychotic Medications for ASD: Abilify (FDA), Risperdol (FDA), Seroquel, Zyprexa to name a few Inhibit both serotonin and dopamine reuptake Used for irritability, aggression, self injury, hyperactivity, and stereotyped behavior

Atypical Antipsychotics: the good and the not so good… The good: The not so good: • About one in ten children with ASD are taking an antipsychotic • Some studies lack control groups • Multiple studies have demonstrated decrease in irritability, aggression, self injury • Noteable side effects: -weight gain -sedation -tremors -movement disorders • Concern for increased cholesterol, glucose, prolactin

Psychopharmacology for AD/HD, Depression, Anxiety, and ASD is both an art and a science The current medical system presents challenges to best care In conclusion: Future research in pharmacogenetics will impact care Wise health care providers, educators, and child psychologists are needed to “bridge the gaps” in care for the best outcomes. What is the next care model? How can we leverage technology to provide these new care models? How can we reform payer systems to help with both cost of medications and reimbursement for care?
 Clinical practice guideline for the diagnosis, evaluation, and")
References American Academy of Pediatrics (2019) Clinical practice guideline for the diagnosis, evaluation, and treatment of Attention- Deficit/Hyperactivity Disorder in children and adolescents. Pediatrics, 144, 1 -25. Cheung, A. H. , Zuckerbrot, R. A. , Jensen, P. S. , Ghalib, K. , Laraque, D. , Stein, R. E. , et al. (2018) Guidelines for adolescent depression in primary care (GLAD-PC): II. Treatment and ongoing management. Pediatrics, 141 Posey, D. J. , Stigler, K. A. , Erickson, C. A. , & Mc. Dougle, C. J. (2008). Antipsychotics in the treatment of autism. The journal of clinical investigation, 118, 6 -14 Zuckerbrot, R. A. , Cheung, A. , Jensen, P. S. , Stein, R. E. , Laraque, D. , et al. (2018) Guidelines for adolescent depression in primary care (GLAD-PC): Part I: Practice preparation, identification, assessment, and initial management. Pediatrics, 141
- Slides: 30