Psychiatric Medication Monitoring in Primary Care Update on




 (Depakene) Carbamazepine (Tegretol)")
")










 Usually develops within 24 hours of med change")
 Diaphoresis Diarrhea Fever Above 100. 4")
: 1139 -1142")



 treatment-emergent SI is very rare In adults,")




- Slides: 29
Psychiatric Medication Monitoring in Primary Care & Update on the Open Door Psychiatry Program Jasen Christensen, DO Brent Jenkins, RN
Disclosure Presenters do not have an actual or potential conflict of interest in relation to this program/presentation.
Learning Objectives - Know the monitoring necessary when treating with mood stabilizers. - Know the monitoring necessary when treating with antipsychotic medications. - Know how to monitor for side effects of antidepressants.
Laboratory Monitoring for Mood Stabilizers
Time to steady Target Serum state Level Lithium Valproic Acid (Depakote) (Depakene) Carbamazepine (Tegretol) Oxcarbazepine (Trileptal) Lamotrigine (Lamictal) 5 days 0. 7 - 1. 1 Necessary Labs Lithium Trough At baseline After dose change TSH Every 6 months BMP Depakote Trough 3 days Variable At least 2 weeks NA NA 60 - 120 6 - 12 NA NA Lab Frequency CBC CMP Tegretol Trough CBC CMP CBC and CMP only if precipitous mental status changes NA At baseline Pearls Lithium IR can case nausea. Lithobid can cause diarrhea. Use Propranolol if tremor develops. After dose change Every 6 months Depakote ER needs 20% dose increase At baseline Induces its own After dose change metabolism through 3 A 4 Every 6 months NA NA Off-label for bipolar. Much better tolerated than Depakote or Tegretol. Always counsel that SJS is medical emergency.
These antiepileptics don’t have sufficient research to support use for bipolar disorder: Phenytoin (Dilantin) Levetiracetam (Keppra) Gabapentin (Neurontin) Topiramate (Topamax)
Metabolic Issues Related to Antipsychotics
Second Generation Antipsychotic Medications Can Cause Metabolic Side Effects Propensity to Cause Weight gain 1 Clozapine (Clozaril) Olanzapine (Zyprexa) Quetiapine (Seroquel) Risperidone (Risperdal) Paliperidone (Invega) Aripiprazole (Abilify) Ziprasidone (Geodon) Lurasidone (Latuda) Cariprazine (Vryalar) Brexpiprazole (Rexulti) High “ Moderate “ “ Low “ Very Low “ “ Some Pearls Not advisable in FQHC / needs REMS Very effective for acute mania Very effective for sleep Most likely to cause Galactorrhea Available as Q month and Q 3 month IM Most likely to cause Akathisia Must be taken with food - BID dosing Must be taken with food - once daily Very long half-life Sedation correlates with Metabolic Risk
Metabolic Syndrome NIH criteria: 3 or more of the following traits, including traits being controlled with medication: • • • Large waist — A waistline that measures at least 35 inches (89 centimeters) for women and 40 inches (102 centimeters) for men • • • High triglyceride level — 150 milligrams per deciliter (mg/d. L), or 1. 7 millimoles per liter (mmol/L), • • • HDL cholesterol — Less than 40 mg/d. L (1. 04 mmol/L) in men or less than 50 mg/d. L (1. 3 mmol/L) in women • Increased blood pressure — 130/85 millimeters of mercury (mm Hg) or higher • Elevated fasting blood sugar — 100 mg/d. L (5. 6 mmol/L) or higher
Rapid weight gain of more than 5% in the first month is the best predictor of significant 2 long-term weight gain.
Basic Recommended Laboratory Monitoring for patients taking a 3 Second Generation Antipsychotic FBG and Lipids: - at baseline, - then at 3 months - then Annually Get Weight at every visit
How to Manage Metabolic Syndrome or Weight Gain due to antipsychotics Try to transition to a less metabolically offensive medication Encourage exercise Diet counseling Consider Metformin
Movement Issues Related to Antipsychotics
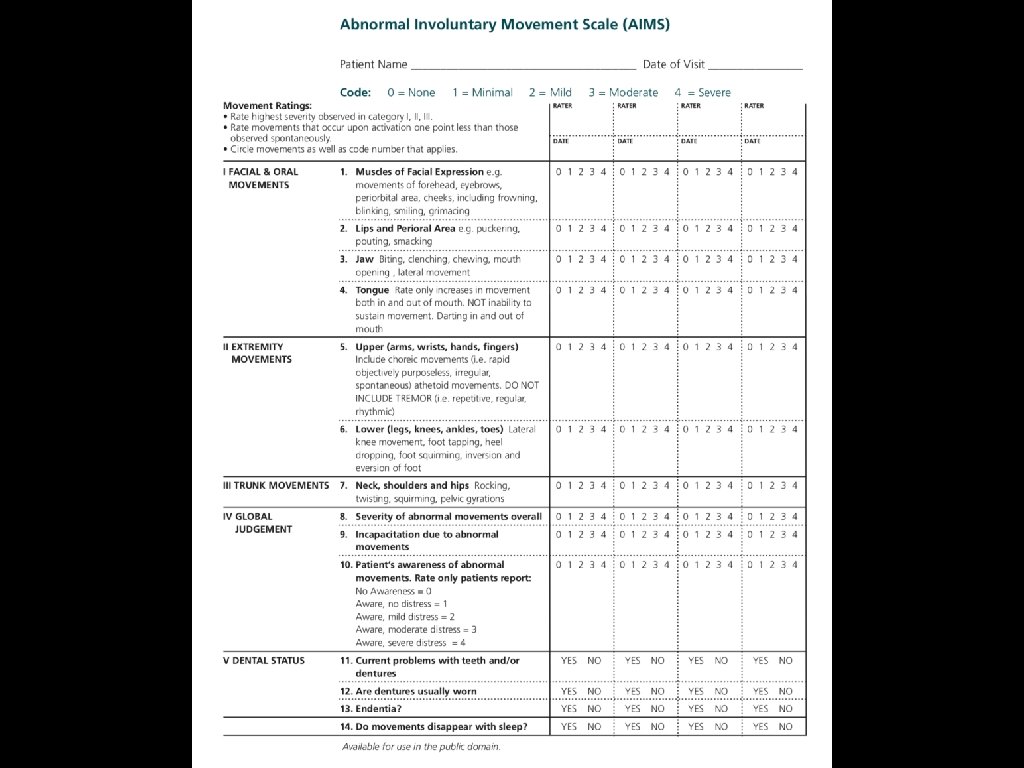
Abnormal Movement Monitoring for patients taking any antipsychotic medication. Restlessness > Akathisia > treat with dose reduction, B-blockers, Mirtazapine (Remeron) or Benzodiazepines * Pill-rolling Resting tremor > Parkinsonism > treat with dose reduction, anticholinergic medications (Cogentin), or Amantadine. Facial grimacing, > Tardive Dyskinesia > stop med if possible puckering, or use lowest possible dose, tongue movements Valbenazine (Ingrezza) $$$
Recommended Frequency of monitoring for Tardive Dyskinesia Ideally: AIMS test at baseline, then every 6 months (Q 3 months for people over 50) More Practically: a brief screen for abnormal movements Q 6 months and ask if patient has noticed abnormal movements.
Serotonin Syndrome
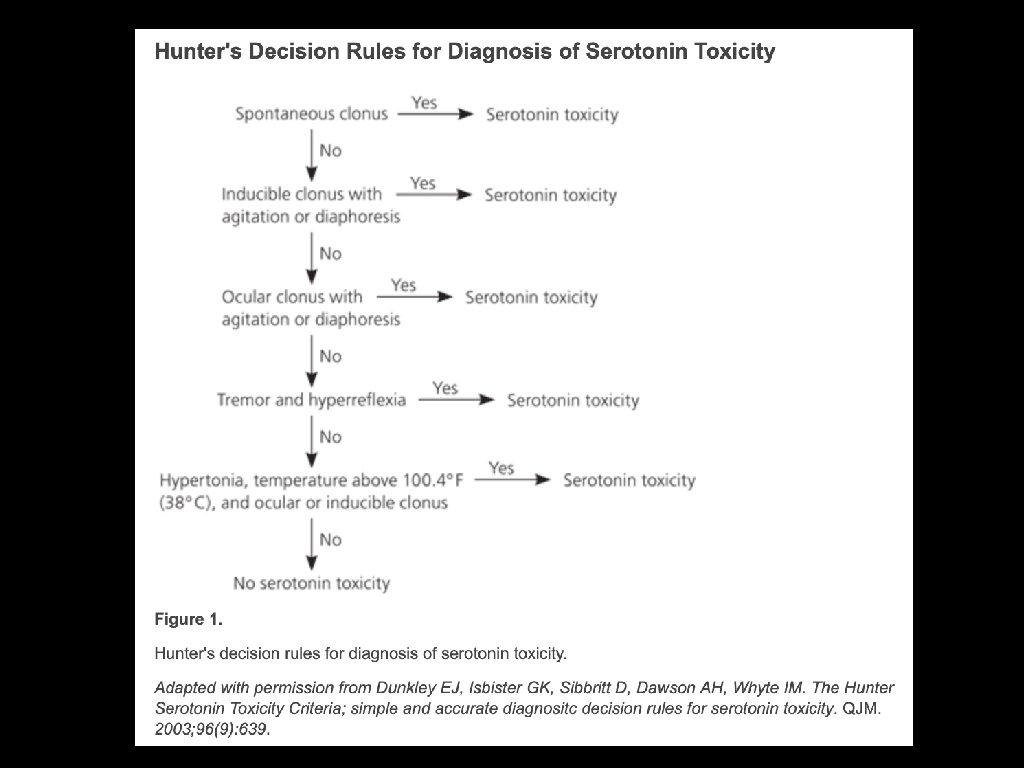
Rare (exact incidence is not clear) Usually develops within 24 hours of med change or exposure Signs/Symptoms fall into 3 categories: - Mental Status Changes - Autonomic Instability - Neuromuscular Rigidity
Signs and Symptoms of Serotonin Syndrome Agitation (restlessness) Diaphoresis Diarrhea Fever Above 100. 4 F Hyperreflexia Incoordination (ataxia) Mental Status Changes (confusion or hypomania) Mycoclonus Ocular Clonus Shivering In very severe cases: Rhabdomyolysis, D. I. C. , Seizures
Ables A, et. al. American Family Physician 2010 May 1; 81(9): 1139 -1142
y results from taking multiple medications wh Lets consider some examples: Effexor + Trazodone ? Prozac + Tramadol + Trazodone + Buspar ? Lexapro + Trazodone + Buspar + Zofran ? Linezolid + any SSRI or SNRI ?
Management of Serotonin Syndrome If symptoms are mild, simply Remove Causative Agent Symptoms resolve in 24 -72 hours If patient is experiencing: hypertonicity hyperthermia progressive mental status changes Send them to the ER
Other Common or Severe Side Effects of Antidepressants
Suicidal Ideation In adults (over age 24) treatment-emergent SI is very rare In adults, antidepressants reduce suicide rates by as much as 19% 4 ——————————————————— FDA back box warning on SSRIs “Increased suicidality risk in children, adolescents, and young adults” (< 24) Highest risk in first 2 months Nearly every guideline recommends treating when indicated Counsel the patient and family about risk See patient back soon and frequently in the beginning
Sexual Dysfunction Incidence up to 40% 5 Most commonly Decreased Libido, Diminished or Delayed Orgasm MANAGEMENT: First: try to determine if symptoms were present before treatment Try lowering the dose Consider switching to Wellbutrin or Remeron or Consider ADDING low-dose Wellbutrin (SA 100 mg QAM)
Nausea Most common side effect by far Most common with Effexor and Zoloft Least common with Lexapro, Prozac, Wellbutrin, Remeron Hang on - - this resolves after 2 weeks in most cases Try dividing doses in the mean time Always instruct patients to take with food in the beginning ( to avoid this side effect and increase adherence ) 6
One last point Always ask about Seizure History before starting Wellbutrin Always document this before prescribing Wellbutrin Thank you! - for everything
References 1. Dayabandara M, et. al. Neuropsychiatric Disease Treatment. 2017; 13: 2331 -2241. 2. Vandenberghe F, et. al. J Clinical Psychiatry. 2015; 76(11) 1417 -1423. 3. American Diabetes Association, American Psychiatric Association, American Association of Clinical Endocrinologists, and the North American Association for the Study of Obesity. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004; 27(2): 596 -601. 4. Isacsson G, Acta Psychiatry Scand. 2000 Aug; 102(2): 113 -7. 5. Rothschild AJ, Journal of Clinical Psychiatry. 2000; 61 Suppl 11: 28 -36. 6. Kelly K, Posternak M, Alpert JE. Toward achieving optimal response: understanding and managing antidepressant side effects. Dialogues Clin Neurosci. 2008; 10: 409 -418.