Psyche Spots Cancer November 2016 The Objectives As

Psyche: Spots: Cancer November 2016

The Objectives • • • As on the programme. Take a multidisciplinary approach. Relax. Have time to think. Enjoy the learning. LEARN THE HOT TIPS

What’s your experience of the psychology of skin disease?

What is the Origin? • Having good skin is an attribute required for beauty. • Is this just for women? • The maintenance creates enormous pressure


Hot Tip • The level of psychological distress is not necessarily proportional to the level of skin disease. • A small patch may be all that it takes.

So What Happens? • The link between stress and exacerbation of skin disease has been confirmed. eg. People with vitiligo notice more patches and eczema may get worse. • The change causes an increasing fear of rejection. • The result is increased anxiety, depression and the potential vicious cycle.

Hot Tip • Many people with chronic skin disease have never been asked about the psychological aspects of their skin problem

Hot Tip • Don’t forget delusional parasitosis

The Facts • Acne is the most common skin condition seen in the developed world. • It is the 8 th most prevalent disease worldwide. • Most 15 -17 year olds will have it and 20% will be classified as moderate to severe. • It is linked to puberty. • 40% will have acne in their thirties • It is more severe in male teenagers

Hot Tip • Acne is associated with a significant level of psychological morbidity

Risk Factors A FH doubles the risk Diet ? ? Over-exposure to sunshine Drugs eg. Phenytoin, steroids, oral contraceptives, depo-contraception, Mirena • Excess androgen states eg. PCOS, congenital adrenal hyperplasia • •

Hot Tip • Always ask about medication and remember that ‘The Pill’’ may not be considered a medication!

Drug Induced Acne • eg. Phenytoin, steroids, oral contraceptives, depo-contraception, Mirena, lithium, ciclosporin,

Excess Androgen States eg. PCOS, congenital adrenal hyperplasia

What is the Underlying Mechanism? Increased sebum production Hyperkeratosis of the pilosebaceous duct Colonisation with P. acnes (bacteria) Release of inflammatory substances eg. Cytokines. • Overall, chronic inflammation of the pilosebaceous unit • •

So What Are The Lesions in Acne? • ? ? ?

So What Do Pharmacists Do?

WWHAM Hot Tip

These Stand For • • W-Who is the preparation for? W-What are the symptoms? H-How long have the symptoms been present for? A-Action already taken? M-Medication being taken Add further ‘M’ for impact on mental health

Severity Guideline Mild <20 comedones or <15 inflammatory lesions Total count <30

Severity Guideline Moderate 20 -100 comedones or 15 -50 inflammatory lesions Total count 30 -125

Severity Guideline • • Severe >5 cysts or Comedomes >100 or Inflammatory lesions >50 or Total lesion count >125

Hot Tips-Promoting Self-Care Tell them not to pick or squeeze Apply treatment regularly and be patient Use gentle cleansers not harsh treatments Avoid the hair being greasy and keep away from forehead Make-up is OK and try oil-free products.

What’s Available OTC?

OTC Products • Benzoyl Peroxide-reduces bacteria but may dry the skin so moisturise and perhaps apply alternate days. Start low strength 2. 5% eg. Oxy 10, Quinoderm • Nicotinamide-anti-inflammatory managing redness and tenderness eg. Nicam gel, Freederm Treatment gel • Salicyclic acid helps to promote shedding of cells when acne not inflamed eg. Acnisal 2%

OTC Products • Antiseptics/Antimicrobials act to reduce the impact of bacteria-inflammation eg. Clearasil Cream Wash, Quinoderm Face Wash • Phycosaccharide AC-brown seaweed extract ? reduces sebum production and bacteria • Light Therapy-blue light or (blue/red light) aims to kill P. acnes. May take time to work and has to be maintained.

Management in Practice

Hot Tips • The primary aim of treatment is to stop scarring or at least keep it to a minimum. • Nodular acne should be referred straightaway

Topical Treatments • Comedomal acne-Retinoid eg. Adapalene, isotretinoin or adapalene/BPO • Papulo-pustular acne-add in BPO eg. adapalene/BPO or clindamycin/BPO or Clindamycin/tretinoin
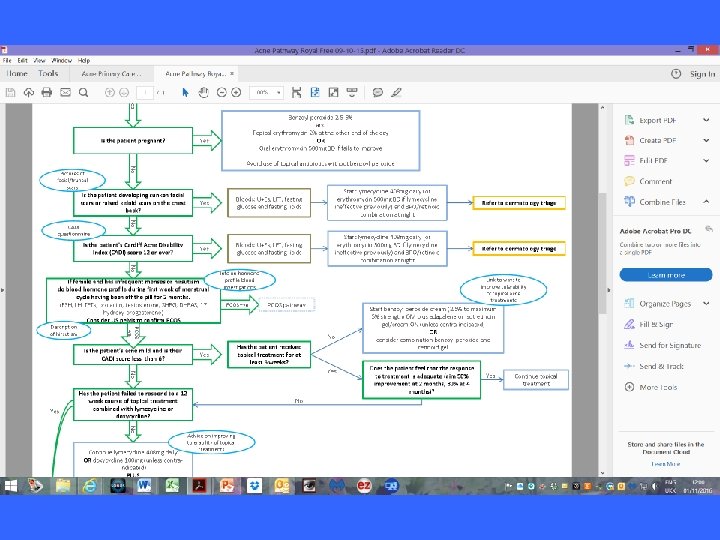
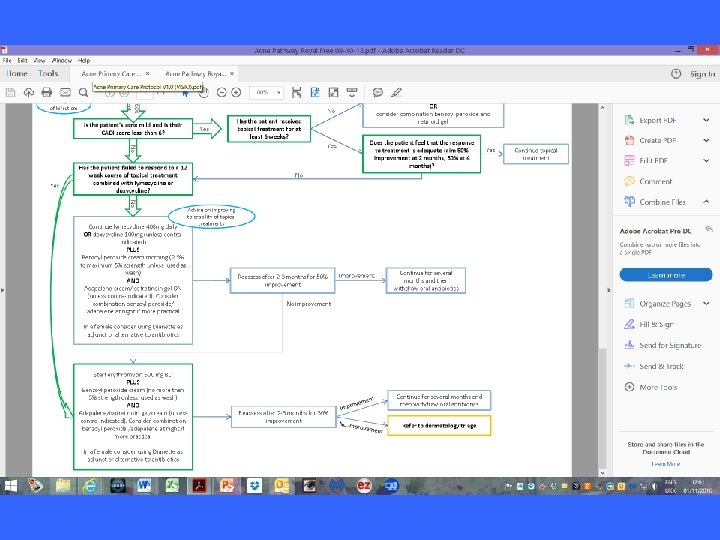

Hot Tip • Topical antibiotics are less effective against non-inflammatory acne and cause resistance. Combine with benzoyl peroxide (Duac) • Topical retinoids may exacerbate acne when first commenced eg adapalene, isotretinoin

Hot Tip • There is increasing resistance to erythromycin • Serial photographs will help to monitor progress

Oral Antibiotics • For severe acne • Acne that doesn’t respond to topical treatments • Acne on the trunk • Lymecycline first choice. Can try doxycycline • Erythromycin • Trimethoprim

Hot Tip • Doxycycline may cause significant upper GI symptoms eg. Oesophageal ulceration. • Watch for phototoxic reactions

Sun Care

What Do You Do To Promote Awareness?
: 1979 -2013 European Age-Standardised Incidence Rates per 100, 000 Population,")
Malignant Melanoma (C 43): 1979 -2013 European Age-Standardised Incidence Rates per 100, 000 Population, by Sex, Great Britain Source: cruk. org/cancerstats You are welcome to reuse this Cancer Research UK statistics content for your own work. Credit us as authors by referencing Cancer Research UK as the primary source. Suggested style: Cancer Research UK, full URL of the page, Accessed [month] [year].
: 2011 -2013 Average Number of New Cases Per Year and")
Malignant Melanoma (C 43): 2011 -2013 Average Number of New Cases Per Year and Age-Specific Incidence Rates per 100, 000 Population, UK Source: cruk. org/cancerstats You are welcome to reuse this Cancer Research UK statistics content for your own work. Credit us as authors by referencing Cancer Research UK as the primary source. Suggested style: Cancer Research UK, full URL of the page, Accessed [month] [year].
: 2002 -2006 Five-Year Relative Survival (%) by Stage, Adults Aged")
Malignant Melanoma (C 43): 2002 -2006 Five-Year Relative Survival (%) by Stage, Adults Aged 15 -99, Former Anglia Cancer Network Please include the citation provided in our Frequently Asked Questions when reproducing this chart: http: //info. cancerresearchuk. org/cancerstats/faqs/#How Note: Relative survival can be greater than 100% because it accounts for background mortality. A relative survival figure greater than 100 indicates that people diagnosed have a better chance of surviving one (five) year(s) after diagnosis than the general population. Prepared by Cancer Research UK Original data source: The National Cancer Registration Service, Eastern Office. Personal communication. http: //ecric. org. uk/

Skin Cancer
")
Risk Factors • Solar radiation • Sun beds (melanoma , actinic keratosis possibly SCC) • Azathioprine (SCC • Ciclosporin • Genetics
 grow slowly- 2 -3 mm/year")
Hot Tip • Basal cell carcinomas (BCC, rodent ulcer) grow slowly- 2 -3 mm/year • They may be multiple so a full skin survey should be completed • They may show blood on the surface

Hot Tip • Superficial spreading BCCs are becoming more common

Hot Tip • Don’t be afraid to feel the lesion. If it feels inappropriately hard or ill-defined then be suspicious.

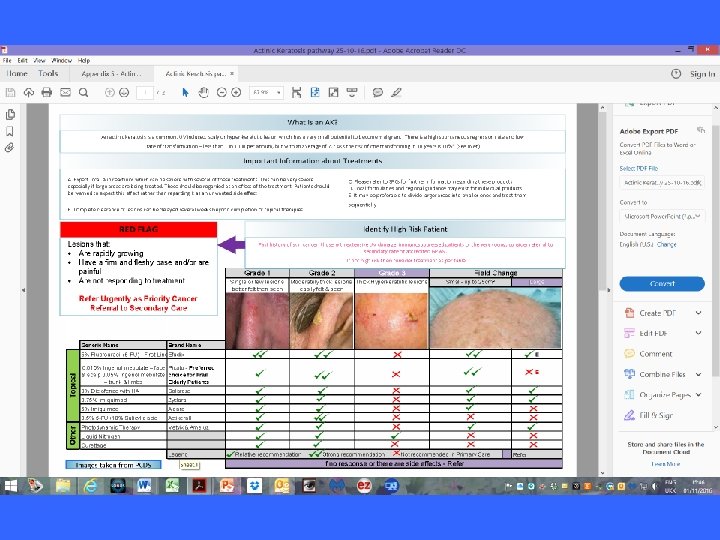
Actinic Keratosis • The result of long-term sun exposure • Scaly crusty lesions on areas exposed to light • Graded according to character and thickness

Yes No No Make every contact count: Smoking status Alcohol consumption BMI / physical inactivity /poor diet Dangerous sun/UV exposure? BMI ≥ 30, <150 mins PA / wk Does the patient have one of the below? Is it a non-healing lesion >6 weeks Single lesion pathway Smoker >14 units/wk♀ >21 units /wk♂ No New mole after onset of puberty Changing mole – size, shape, colour Y Y History - assessment of risk factors • Family history of skin cancer • Immunosuppressed sunburn / sunbed use • Multiple naevi • Personal history of skin cancer Lifestyle advice Is it a pigmented lesion? KEY: Reassurance, information, self-surveillance and sunscreen advice Questions for GP to ask Urgent referral Routine referral Public health intervention Audio-visual aids for patient and GP • Fitzpatrick skin type • Level of UV exposure - episodes of Examination - Does the patient have any red flags? Suspected melanoma Glasgow 7 -point checklist Lesions scoring 3 points or more are suspicious Major features – 2 points each Minor features – 1 point each Change in size Irregular shape Irregular colour Yes Fitzpatrick skin type Pictures of SCCs and melnanom a Unsure Diameter 7 mm or more Inflammation Oozing Change in sensation Suspected squamous cell carcinoma (SCC) - enlarging non healing, scaly or crusted area of skin or lump, often tender and commonly occurring on sunexposed sites No Is the lesion: Pigmented? -eg seborrhoeic keratosis, Pigmented basal cell carcinoma Vascular? -eg haemangioma Crusted / scabbed/ulcerated? -eg basal cell carcinoma, seborrhoeic keratosis, viral wart Photographs of most common differential diagnoses Urgent Referral to Rapid Access Skin Cancer Clinic Suspected malignant melanoma or squamous cell carcinoma - refer as per 2 week cancer referral guidelines Refer to dermatology triage Suspected Melanoma/ SCC Suspected BCC Benign lesion 2 week wait referral Fast track to minor ops list for biopsy Refer back to GP with advice Useful links for differential diagnosis Yes Are you confident in your diagnosis and confident it is benign? No Refer to dermatology triage Suspected Melanoma/ SCC Suspected BCC Benign lesion 2 week wait referral Fast track to minor ops list for biopsy Refer back to GP with advice Yes Watchful waiting review 8 weeks Reassurance, information, selfsurveillance and sunscreen advice Patient with persistent or slowly evolving unresponsive skin conditions in which the diagnosis is uncertain

Squamous Cell Carcinoma • Risk Factor-exposure to sunlight • Age
")
Melanoma • • • 4 types Superficial spreading Nodular Lentigo maligna (face ad neck) Acral melanoma (palms, soles, under nails)

Risk Factors • High risk-strong family history and large congenital naevi • Moderate-Organ transplants, large number of moles (atypical naevus syndrome) • Slight increased rsik-Fh, skin that burns easily, • Red/blonde hair

Hot Tip • Most melanomas start de novo
")
EFG • E-Elevation • F-Firmness • G-Growth (in the last 4 -8 weeks)

Quiz
- Slides: 57