Psoriasis Dr Abbas Pardakhty 2011 Kerman Faculty of

Psoriasis Dr Abbas Pardakhty, 2011 Kerman Faculty of Pharmacy

Prevalence Psoriasis occurs in 2% of the world’s population Prevalence in the U. S may be as high as 4. 6% Highest in Caucasians In Africans, African Americans and Asians between 0. 4% and 0. 7% • • 3

Prevalence Equal frequency in males and females • May occur at any age from infancy to the • 10 th decade of life First signs of psoriasis • Females mean age of 27 years – Males mean age of 29 years – 4

Prevalence Two Peaks of Occurrence • One at 20 -30 years – One at 50 -60 years – Psoriasis in children • Low – between 0. 5 and 1. 1% in children 16 – years old and younger Mean age of onset - between 8 and 12. 5 years – 5

Prevalence Two-thirds of patients have mild disease One-third have moderate to severe disease Early onset (prior to age 15) Associated with more severe disease – More likely to have a positive family history – Life-long disease Remitting and relapsing unpredictably – Spontaneous remissions of up to 5 years have been – reported in approximately 5% of patients • • 6
")
Genetics and Pathogenesis Psoriasis and the Immune System • The major histocompatibility complex (MHC) – Short arm of chromosome 6 • Histocompatibility Antigens (HLA) – HLA (human leukocyte antigen)-Cw 6 • HLA-B 13, -B 17, -B 37, -Bw 16 • T-lymphocyte-mediated mechanism – 7

Psoriasis as a Systemic Disease Koebner Phenomenon Elevated ESR Increased uric acid levels → gout Mild anemia Elevated α 2 -macroglobulin Elevated Ig. A levels Increased quantities of Immune Complexes • • 8

Psoriasis as a Systemic Disease Psoriatic arthropathy • Aggravation of psoriasis by systemic factors • Medication – Focal infections – Stress – Life-threatening forms of psoriasis • 9
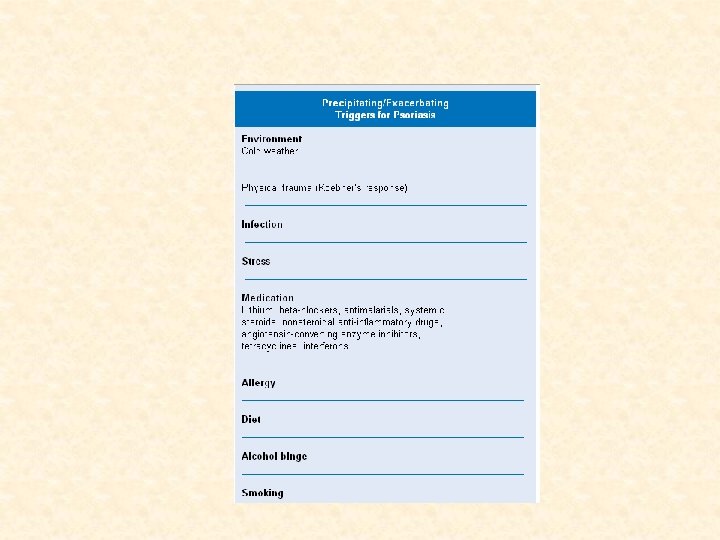

• Physical trauma: These injuries include endogenous and exogenous causes such as photosensitivity, dermatitis, herpes zoster, abrasions, burns, bites, shaving, surgery, and tattoos, among others. • Infection: Streptococcal pharyngitis and HIV type 1 appear to be triggers

Clinical Variants of Psoriasis 12

Clinical Types Guttate Chronic Plaque Flexural Pustular Nail Psoriasis Erythroderma Arthropathy • •
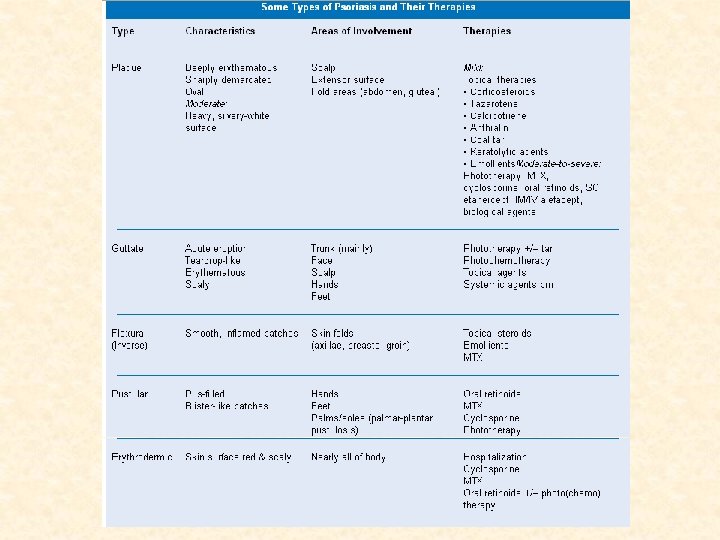

Characteristic Lesion of Psoriasis Sharply demarcated erythematous plaque • with micaceous silvery white scale Histopathology • Thickening of the epidermis – Tortuous and dilated blood vessels – Inflammatory infiltrate primarily of – lymphocytes 15

Psoriatic Plaque 16

Severity of Disease Three Cardinal Signs of Psoriatic Lesions • Plaque elevation – Erythema – Scale – Body Surface Area • 17

Chronic Plaque Psoriasis Most Common Variant Plaques may be as large as 20 cm Symmetrical disease Sites of Predilection Elbows – Knees – Presacrum – Scalp – Hands and Feet – • • 18

Chronic Plaque Psoriasis 19

Chronic Plaque Psoriasis 20

Chronic Plaque Psoriasis May be widespread – up to 90% BSA • Genitalia involved in up to 30% of patients • Most patients have nail changes • Nail pitting – “Oil Spots” – Involvement of the entire nail bed – Onychodystrophy • Loss of nail plate • 21

Widespread Chronic Plaque Psoriasis 22

Chronic Psoriasis 23

Psoriasis of the Nail 24

Psoriasis of the Nail 25

Symptoms of Chronic Plaque Psoriasis Pruritus Pain Excessive heat loss Patient Complaints • • Unsightliness of the lesions – Low self-esteem – Feelings of being socially outcast – Excessive scale – 26

Guttate Psoriasis Characterized by numerous 0. 5 to 1. 5 cm papules and plaques Early age of onset Most common form in children Streptococcal throat infection often a trigger Spontaneous remissions in children Often chronic in adults • • • 27

Guttate Psoriasis 28

Life–Threatening Forms of Psoriasis Generalized Pustular Psoriasis • Erythrodermic Psoriasis • 29

Generalized Pustular Psoriasis Unusual manifestation of psoriasis Can have a gradual or an acute onset Characterized by waves of pustules on erythematous skin often after short episodes of fever of 39˚ to 40˚C Weight loss Muscle Weakness Hypocalcemia Leukocytosis Elevated ESR • • 30

Generalized Pustular Psoriasis Cause is obscure • Triggering Factors • Infection – Pregnancy – Lithium – Hypocalcemia secondary to hypoalbuminemia – Irritant contact dermatitis – Withdrawal of glucocorticosteroids, primarily – systemic 31

Generalized Pustular Psoriasis 32

Erythrodermic Psoriasis Classic lesion is lost • Entire skin surface becomes markedly • erythematous with desquamative scaling. Often only clues to underlying psoriasis are • the nail changes and usually facial sparing 33

Erythrodermic Psoriasis Triggering Factors • Systemic Infection – Withdrawal of high potency topical or oral – steroids Withdrawal of Methotrexate – Phototoxicity – Irritant contact dermatitis – 34

Erythrodermic Psoriasis 36

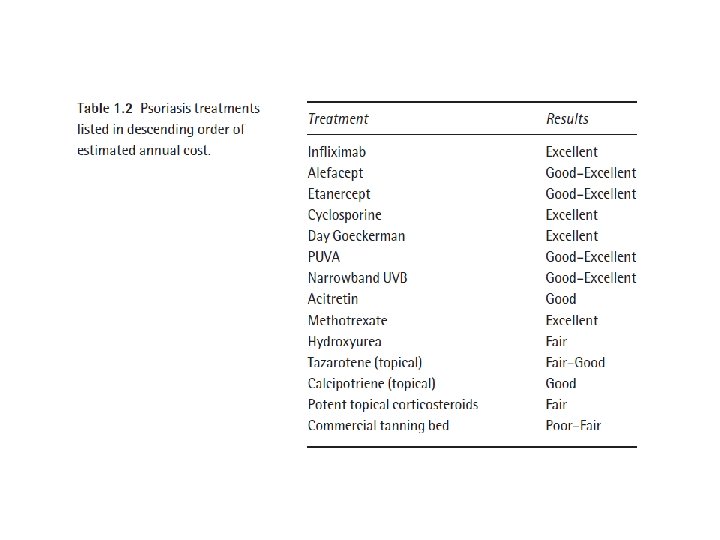
Psoriasis Treatment

Session 3

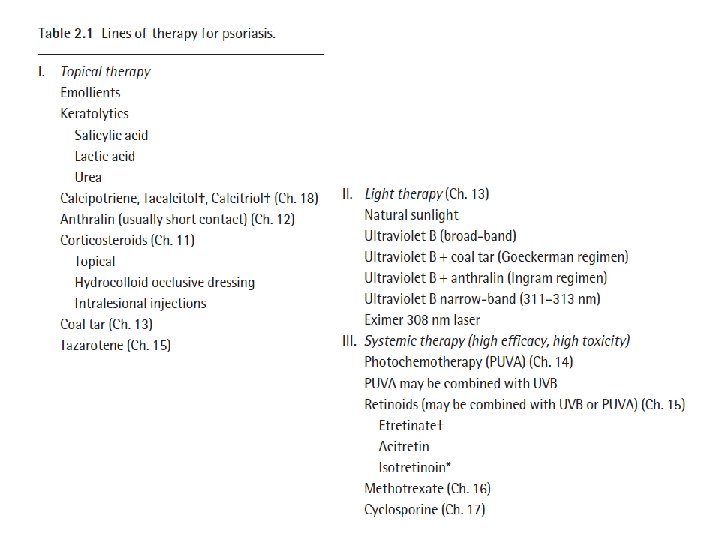
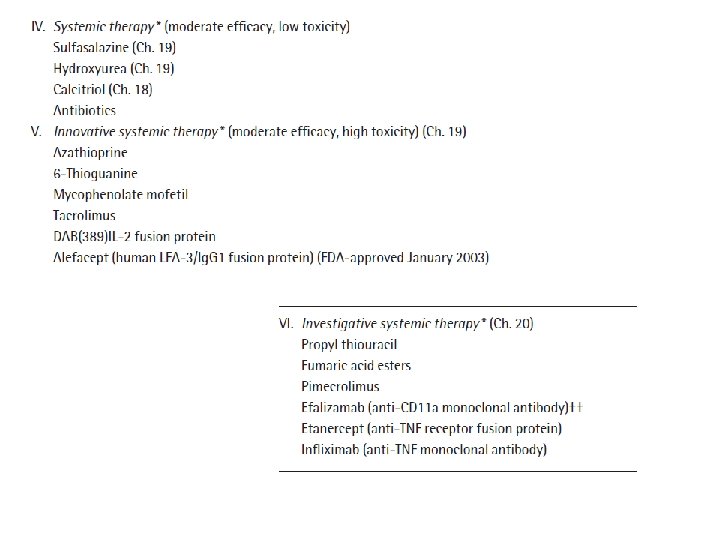
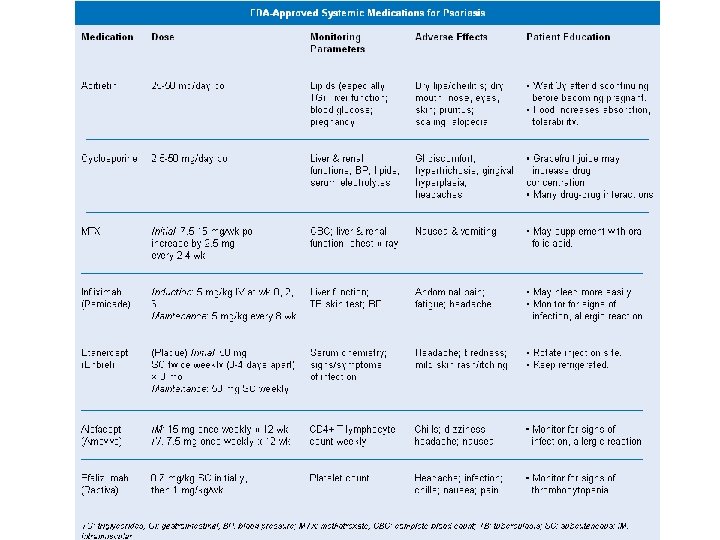
Psoriasis treatment Topical • Systemic • Phototherapy •
 Coal tar solution 5 m.")
Vehicle-Penetration Enhancer-Viscosity Enhancer Rx Psoriasis Lotion (100 m. L) Coal tar solution 5 m. L • Salicylic acid 5 g • Urea 10 g • Triamcinolone acetonide 160 mg • Propylene glycol qs 100 m. L • Dissolve the urea and salicylic acid in about 75 m. L of propylene • glycol; this may take 30 to 45 minutes. Add the triamcinolone acetonide and mix well. Incorporate the coal tar solution and mix well. Add sufficient propylene glycol to make 100 m. L and thoroughly mix. Package and label. Coal tar Solution: coal tar 20%, polysorbate 80 5%, in alcohol (96%), •

Coal tar and Salicylic acid ointment Coal tar 2 g SA 2 g Emulsifying wax 11. 4 g Polysorbate 80 4 g Liquid paraffin 7. 6 g White soft paraffin 19 g Coconut oil 50 g • •
. Coal tar, • a byproduct of the coal manufacturing process,")
Tar-based shampoos (Neutrogena T/Gel). Coal tar, • a byproduct of the coal manufacturing process, helps conditions such as dandruff, seborrheic dermatitis and psoriasis by slowing cell turnover. abpardakhty@kmu. ac. ir 46

Neutrogena T/Gel 1% Coal Tar • abpardakhty@kmu. ac. ir 47

Coal tar shampoo Dandruff Seborrheic dermatitis Psoriasis Wash first time Remain the foam for 5 min at second time Photosensitizer abpardakhty@kmu. ac. ir • • • 48

Polytar Wet the scalp and hair. Apply the medicine to the • scalp, massage into a lather, and allow it to remain on the scalp for 5 minutes. Rinse thoroughly and repeat. Wash your hands after using Coal Tar Shampoo. • If you miss a dose of Coal Tar Shampoo, use it as • soon as possible. If it is almost time for your next dose, skip the missed dose and go back to your regular dosing schedule. Do not use 2 doses at once. abpardakhty@kmu. ac. ir 49

Neutrogena T/Sal 3% Salicylic Acid Fragrance-free Preservative-free Color-free abpardakhty@kmu. ac. ir • • 51

To use shampoo as a scalp treatment: Use before bathing. Do not wet hair. Apply Salicylic Acid Shampoo with the applicator directly to affected areas of the scalp. Leave on for 5 minutes, gradually increasing the treatment time up to 1 hour. After treatment, rinse thoroughly with water. Wash your hands after each use. You may use a non-medicated shampoo after using Salicylic Acid Shampoo, if desired. abpardakhty@kmu. ac. ir • • • 52

To use shampoo as a medicated shampoo: Wet hair, apply Salicylic Acid Shampoo with the applicator directly to scalp, and massage vigorously for several minutes. Rinse thoroughly. Be sure to wash your hands after each use. Use Salicylic Acid Shampoo daily until the condition clears, or as directed by your doctor abpardakhty@kmu. ac. ir • • 53

Ceanel A clear, viscous golden-yellow colored liquid containing: Undecenoic acid 1% v/v, Cetrimide 10% w/v, Phenylethyl alcohol 7. 5% v/v Dandruff Seborrhoeic dermatitis Psoriasis abpardakhty@kmu. ac. ir • • 54
 •")
Tazarotene Tazorac® (Tazarotene) •

Tazarotene is a prodrug that is de-esterified in the skin to its active form, tazarotenic acid. Psoriasis: tazarotene 0. 05% cream or gel is used initially and increased to 0. 1% if necessary. Acne: tazarotene is applied as a 0. 1% gel or cream once daily in the evening. photodamage (facial fine wrinkling, mottled hypo- and hyperpigmentation, and benign facial lentigines): A 0. 1% cream • •
 •")
Acitretin Soriatane®, Neotigason® (Acitretin) •

Acitretin is used by mouth in the treatment of • severe psoriasis resistant to other forms of therapy, palmo-plantar pustular psoriasis, and in severe congenital ichthyosis and Darier's disease (keratosis follicularis). Acitretin is used alone or with PUVA or UVB in • psoriasis.

Acitretin In the UK, it is given in an initial daily dose of • 25 or 30 mg with food for 2 to 4 weeks In the USA initial doses up to 50 mg daily are • permitted. The daily dosage is adjusted thereafter according to clinical response and adverse effects
 •")
Daivonex® (Calcipotriene, Calcipotriol) •

Calcipotriol is a vitamin D 3 derivative. In vitro • it appears to induce differentiation and to suppress proliferation of keratinocytes. Calcipotriol is used in a cream or ointment for • the management of plaque psoriasis and as a solution in the management of scalp psoriasis; the concentration of calcipotriol used is 0. 005%.
 • Alefacept is a recombinant human fusion • protein that binds")
Alefacept Amevive® (alefacept) • Alefacept is a recombinant human fusion • protein that binds to CD 2 on memory Tlymphocytes, preventing their activation and reducing their number.

Alefacept blood test every 2 weeks to check your T-cell • levels Cancers (mostly skin cancers), lymphomas, • serious infections, including wound infections and pneumonia. Liver injury •
 •")
Efalizumab Raptiva® (efalizumzb) •

Efalizumab is a humanised monoclonal • antibody that binds to human CD 11 a on leucocytes to inhibit the activation of Tlymphocytes. Efalizumab is given by subcutaneous injection. •
 •")
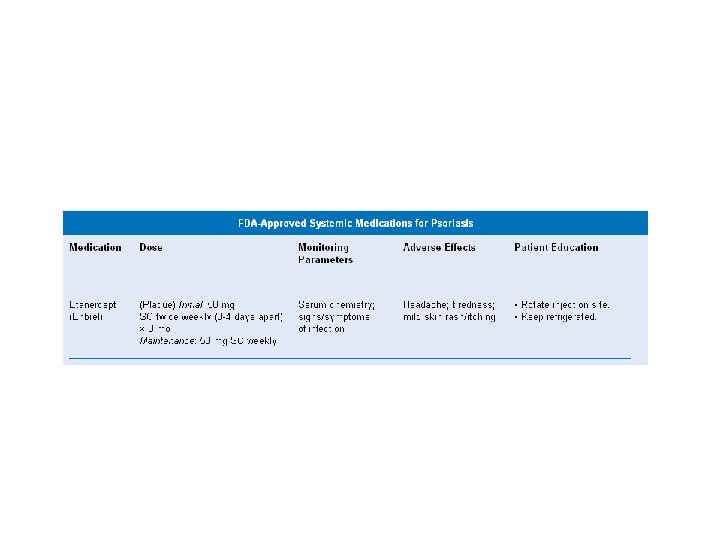
Enbrel® (Etanercept) •
 receptor that")
Etanercept is a recombinant version of soluble human tumour necrosis factor (TNF) receptor that binds specifically to TNF and blocks its interaction with endogenous cell-surface TNF receptors. rheumatoid arthritis psoriatic arthritis ankylosing spondylitis juvenile idiopathic arthritis In the USA, etanercept is also used in the treatment of chronic, moderate to severe plaque psoriasis in patients over 18 years. • • •
 Tacrolimus is a potent macrolide (macrolactam) immunosuppressant derived from Streptomyces tsukubaensis, and")
Tacrolimus (Prograf®) Tacrolimus is a potent macrolide (macrolactam) immunosuppressant derived from Streptomyces tsukubaensis, and has actions similar to those of ciclosporin. transplantation atopic eczema Tacrolimus has been shown to be effective in the treatment of psoriasis when used orally or topically. • •

Methotrexate Folic acid antagonist • Usually reserved for severe, recalcitrant, • disabling psoriasis Maximum improvement can be expected after • 8 -12 weeks 70

Contraindications - Methotrexate Nursing mothers Patients with alcoholism Alcoholic liver disease Other chronic liver disease Patients with overt or laboratory evidence of immunodeficiency syndromes Patients who have preexisting blood dyscrasias • • • 71

Methotrexate Pregnancy Category X drug product • Contraindicated in pregnant women with psoriasis – Pregnancy must be excluded in women of childbearing potential – Pregnancy should be avoided if either partner is receiving MTX during – and for a minimum of 3 months after therapy for male patients and for at least one ovulatory cycle after therapy for female patients 72

Methotrexate – Side Effects Acute or chronic hepatotoxicity Hepatic cirrhosis Leukopenia Thrombocytopenia Anemia, including aplastic anemia Rarely, interstitial pneumonitis Stomatitis Nausea/vomiting Alopecia Photosensitivity Burning of skin lesions • • • 73

Neoral Potent Immunosuppressive • Adult, non-immunocompromised patients • with severe, recalcitrant plaque psoriasis Maximum efficacy achieved at 16 weeks of • therapy 74

Contraindications - Neoral Concomitant PUVA or UVB therapy Methotrexate or other immunosuppressive agents Coal tar or radiation therapy Patients with abnormal renal function Patients with uncontrolled hypertension Patients with malignancies Nursing mothers • • 75

Neoral – Side Effects Possibility of Irreversible renal damage Hypertension Headache Hypertriglyceridemia Hirsutism/hypertrichosis Paresthesia/hyperesthesia Influenza-like symptoms Nausea/vomiting Diarrhea Lethargy Arthralgia • • • 76

Neoral Multiple prescreening tests are required • Tests must continue throughout treatment • with dosage adjustment as necessary to prevent end-organ damage 77
therapy Two types of phototherapy • Ultraviolet B (UVB) – Ultraviolet A + psoralen")
Photo(chemo)therapy Two types of phototherapy • Ultraviolet B (UVB) – Ultraviolet A + psoralen (PUVA) – 78
 – Treatment")
UVB Two types • Broadband UVB – Narrowband UVB (311 -313 nm) – Treatment is time consuming • 2 -3 visits/week for several months – Side effect – possibility of experiencing an • acute sunburn reaction 79

PUVA Consists of ingestion of or topical treatment with a psoralen followed by UVA Usually reserved for severe, recalcitrant, disabling psoriasis Time consuming – 2 -3 visits/wk; at least 6 weeks Precautions • • Patients must be protected from further UV light for – 24 hours post treatment With oral psoralen, wrap around UV-blocking glasses – must be worn for 24 hours post treatment 80

PUVA Side effects with oral psoralen • Nausea – Dizziness – Headache – Side effects with PUVA • Early – Pruritus • Late – Skin damage • Increased risk for skin cancer, particularly squamous • cell (SCC) and after 200 - 250 treatments, increased risk for melanoma 81

Day Goeckerman UVA + Coal tar •

Contraindications to PUVA Patients less than 12 years of age Patients with a history of light sensitive disease states Patients with, or with a history of melanoma Patients with invasive SCC Patients with aphakia (the absence of the lens of the eye) • • • 83
- Slides: 83