Protons Photons and Electrons Intern Case Report SALMAN






















 �SIADH (small cell) �Hypertrophic Pulmonary Osteoarthropathy �Cushing’s (small cell) �Dermatomyositis/polymyositis")


 Enhance nerve")




 �Risk of brain mets at 2 years is clinically 50%")



 produce high energy x- rays that are shaped")




 � 2. http: //www.")
- Slides: 43
Protons, Photons, and Electrons… Intern Case Report SALMAN HASAN, D. O. , PGY-1 1/23/2015
Case Presentation: 9/28/14 �Patient is a 56 y/o male presenting with generalized weakness for a few months. Lost about 30 lbs 2/2 gagging when chewing food Increasingly short of breath Anterior chest pain Had a fall and broke 3 ribs Nothing like this happened before
Case Presentation �Past Medical History HTN Diabetes �Past Surgical History None �Medications Aspirin 81 mg Lisinopril Metformin �Allergies Pseudoephedrine (hives) �Family History Uterine, colon cancer Father: lung cancer, died of an MI Celiac disease in mother and sister �Social History Former radar tech for the navy Lives alone Smoked 1. 5 -2 ppd for 40 years No alcohol use No illicit drug use
Case Presentation �ROS: �Constitutional: +weight loss, dizziness �HEENT: no changes in hearing or vision �Resp: dry cough, dyspnea on exertion �CV: positional chest pain, no palpitations �GI: nausea and vomited once after morphine �GU: no dysuria �Skin: no rashes or skin changes �Neuro: no numbness or tingling �Heme: no abnormal bleeding or bruising �Psych: + insomnia, no anxiety
Case Presentation � Vitals: BP: 131/61 P: 94 R: 18 Ox: 97 RA T-97. 9 � Physical Exam: � Gen: WD, NAD � HEENT: No scleral icterus � Neck: No thyromegaly or nodules � Lungs: Wheezing throughout, no crackles � Heart: RRR � Abd: Soft, NTND, BS+ � Ext/MSK: decreased muscle tone and temporal wasting � Skin: Pale, normal temperature � Neuro: 5/5 distal strength � Lymph: No cervical or supraclavicular lymphadenopathy � Psych: Full affect, fluent speech
Case Presentation �Labs: �CBC: WBC: 11. 8, Hgb: 13. 5, Plt: 349 �BMP: Na: 133, K: 4. 0, Cl: 97, CO 2: 23, BUN: 12, Crt: 1. 0, Glucose: 135, Ca: 9. 5 �UA (-), TSH WNL, Lipase WNL
Case Presentation � CXR: Borderline heart enlargement. Mediastinal contour is abnormal. Increased density of AP window. Lungs are hyperextended without consolidation. No pleural fluid. Remote right anterolateral seventh rib fracture. Findings may represent central adenopathy, enlarged with pulmonary artery or underlying mass. � CT Chest: Large left hilar, perihilar, and posterior mediastinal soft tissue mass with encasement and narrowing of the left pulmonary artery and its subsegmental branches and encasement and narrowing of the left mainstem bronchus and the lingular and inferior branches as above. Metastases to the bilateral ribs as above. Associated soft tissue mass of the left fourth rib. Nodular appearance of the left adrenal gland. Concerning given the presence of malignancy. Multiple tiny solid pulmonary nodules.
Case Presentation � 10/1: MRI Brain: No acute intracranial abnormality, no metastatic disease. � 10/4: MRI Thoracic/Lumbar spine: Direct invasion of the T 4 vertebral body from posterior mediastinal mass without epidural or foraminal extension of tumor. No cord compression.
Case Presentation � 10/6: Posterior mediastinal biopsy: Sections show infiltrating carcinoma with tumor necrosis and apoptosis. The malignant cells show stippled chromatin, scant cytoplasm, and focal crush artifact. Nuclear molding is present. Histopathology consistent with small cell carcinoma Extensive Stage
Case Presentation �Started on carboplatin/etoposide Cycle 1: October 9 -11 -OSH Cycle 2: October 29 -31 Cycle 3: November 20 -22 � Neurology consulted recommended repetitive stimulation EMG (Concern for Lambert Eaton) Cycle 4: December 10 -12
Case Presentation: 12/20/14
Case Presentation: Neuro/Psych Exams � 1/5: � 1/6 � 1/9
Case Presentation � 1/5 -1/9/15: Returned for Restaging CT Head, Chest, Abdomen/MRI Brain: Show improvement in the prior mass and lymphadenopathy. No findings of metastases in the brain. Plan to undergo 2 more cycles of chemotherapy followed by prophylactic cranial irradiation. 1/8 Ordered: Voltage gated calcium channel antibody positive on 1/16/15
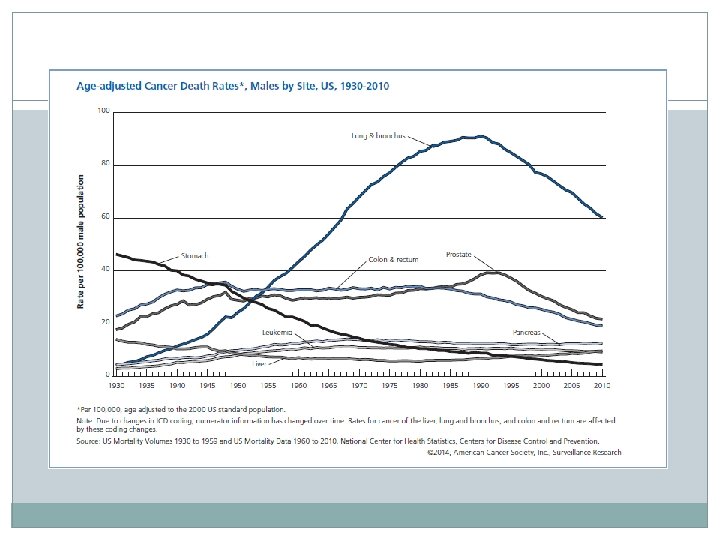
Cancer Epidemiology �Cancer is the second most common cause of death in the US, exceeded only by heart disease. 1 � 1 of every 4 deaths. 1
Lung Cancer � 2 nd most common cancer in men and women Men – prostate Women – breast �Highest death rate among cancers in both men and women �The 5 year relative survival rate for all cancers diagnosed between 2003 and 2009 is 68% up from 49% in 1975 -1977
Risk Factors �Smoking Accounts for 90% of all lung cancers 40 pack years increases risk by 20 fold compared to a nonsmoker �RT – Hodgkin's and breast cancer �Environmental toxins: asbestos, radon, polycyclic aromatic hydrocarbons �HIV �Genetic factors
Pathology �Small cell: 13% �Non small Cell Adenocarcinoma: 38% Squamous cell: 20% Large Cell: 5%
Small Cell Lung Cancer � 1/3 patients present with limited stage disease � 10 -15% present with brain metastases �Most common solid tumor associated with paraneoplastic syndromes �Most important prognostic factors are stage and performance status
Clinical Manifestations �Cough: 50 -75% �Hemoptysis: 25 -50% �Chest pain: 20% �Dyspnea: 25% �Superior vena cava syndrome �Pancoast tumors
Staging
Metastases �Bone �Brain �Adrenal �Typically osteolytic
Paraneoplastic Syndromes �Hypercalcemia (squamous) �SIADH (small cell) �Hypertrophic Pulmonary Osteoarthropathy �Cushing’s (small cell) �Dermatomyositis/polymyositis �Lambert Eaton Syndrome
Lambert Eaton Myasthenic Syndrome �Pathophysiology: Disorder of reduced Ach release from presynaptic nerve terminal due to antibodies against voltage gated calcium channel. �Incidence 3% of patients with SCLC �Symptoms Slowly progressive proximal muscle weakness Gait disturbance Depressed or absent DTRs Autonomic dysfunction: dry mouth, erectile dysfunction No weakness of extra ocular muscles
Lambert Eaton Myasthenic Syndrome �Diagnosis: Antibodies to VGCC Electrodiagnostic studies reproducible post-exercise increase in compound muscle action potential
LEMS � Treatment � Symptomatic Prescriptions 3, 4 -Diaminopyradine (3, 4 -DAP) Enhance nerve terminal depolarization enhancing Ca entry � Seizures � Acetylcholinesterase inhibitors � Pyridostigmine No benefit in combination
Diagnosis
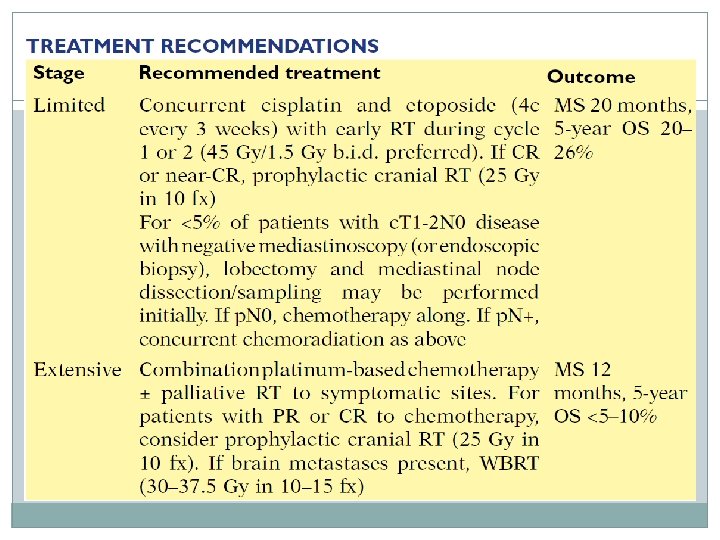
Management
Management
Management
Prophylactic Cranial Irradiation (PCI) �Risk of brain mets at 2 years is clinically 50% and about 80% in autopsy �Two meta analyses showed benefit in terms of brain mets incidence (50% reduction) and survival (26% improvement) at 3 years �PCI recommended for patients with limited disease and extensive stage with a complete or partial response to therapy
Oncology Team �Medical Oncologist �Surgical Oncologist �Radiation Oncologist Use ionizing radiation as part of cancer treatment to control malignant cells Ionizing radiation damages DNA either directly or indirectly through the production of free radicals Cancer cells have decreased ability to repair damage Gray (Gy) units of radiation= 1 joule of radiation/kg of matter Therapy is fractionated � Ie. 30 Gy in 10 fractions
Radiation Therapy Team �Radiation Oncologist –MD/DO �Medical Physicist – help plan treatments, quality control, equipment maintenance �Radiation Therapist – operate the equipment �Dosimetrist – helps create treatment plan, calculates precise amount of radiation delivered to the patient �Nursing
Radiation Course
Radiation Oncology Intro �Linear Accelerator (LINAC) produce high energy x- rays that are shaped to conform to the shape of the patients tumor External Beam RT Sterotactic Radiosurgery focused beams � Cyberknife � Gamma � Etc. knife
Proton Therapy �Photons deposit energy along their path through tissue �Protons deposit much of their energy at the end of their path
Brachytherapy �Brachy – Greek for short distance �Sealed radioactive sources placed in the area of treatment �Low Dose Rate (LDR) – 2 Gy/h Ie. Prostate seeds �High Dose Rate (HDR) - >12 Gy/h
Conclusion �Small Cell Carcinoma of the lung �Lambert Eaton Syndrome �PCI �Intro to Radiation Oncology �Thank you
Questions?
Resources � 1. http: //www. cancer. org/acs/groups/content/@research/documents/webc ontent/acspc-042151. pdf (ACS) � 2. http: //www. cdc. gov/nchs/fastats/leading-causes-of-death. htm � 3. http: //www. uptodate. com/contents/overview-of-the-risk-factorspathology-and-clinical-manifestations-of-lungcancer? source=search_result&search=lung+cancer&selected. Title=1~150 � 4. http: //www. uptodate. com/contents/overview-of-the-risk-factorspathology-and-clinical-manifestations-of-lungcancer? source=search_result&search=lung+cancer&selected. Title=1~150 � 5. http: //www. uptodate. com/contents/clinical-features-and-diagnosis-oflambert-eaton-myasthenicsyndrome? source=search_result&search=lambert+eaton+myasthenic+syn drome&selected. Title=1~26 � 6. NCCN � 7. Hanson and Roach. Handbook of Evidence Based Radiation Oncology. � 8. https: //www. astro. org/uploaded. Files/Affiliates/ARRO/Future_Resident s/Intro. To. RO. pdf