Prosthetic valves Types Selection Complications Types Bioprosthetic valves

Prosthetic valves Types Selection Complications
 • Bovine • porcine – Homograft (allograft)")
Types • Bioprosthetic valves – Heterograft (xenograft) • Bovine • porcine – Homograft (allograft) – Autograft • Pericardial • Pulmonary (Ross) • Mechanical – Caged ball valve – Tilting disc valve – Bileaflet valve
 • Stentless – Porcine • Toronto SPV valve, medtronic freestyle valve • Stented")
Heterografts(xenografts) • Stentless – Porcine • Toronto SPV valve, medtronic freestyle valve • Stented - facilitate implant, maintain 3 D relationship, more physiological flow The Hancock M. O. II aortic bioprosthesis (porcine) – Porcine • Hancock , carpenteir edward s, medtronic – Bovine • Stented bovine p prosthesis Carpentier-Edwards Duralex mitral bioprosthesis

Tissue heterograft • Advantages - No need of anticoagulation after 1 st 3 m – Little hemolysis • Disadvantages – Limited , uncertain durability • Cuspal tear • Perforation • degeneration – Rapid deterioration esp children • • Fibrin depostn Ca++ 10 -30% need re op in 10 yr 30 -60% need re op in 15 yr – Small size have poor hemodynamics

Bioprosthetic valve • • Preferred in Pregnancy Bleeding Diathesis Age> 70 years Poor compliance

Mechanical valves – Caged ball valve Advantages • Oldest • durabilty upto 40 yr Disadvantages • • high profile hemolysis high thrombogenecity Poor hemodynamics in small sizes Unique features • Occluder travels completely out of the orifice, reduces thrombus & pannus growing from the sewing ring • Continuously changing points of contact of the ball reduces the wear & tear in any one area • Thrombogenic risk 4 -6% / year

Starr Edwards Valve • not suitable - for the mitral position in patients with a small left ventricular cavity - for the aortic position in those with a small aortic annulus - those requiring a valve-aortic arch composite graft
 -")
Tilting disc valve- monoleaflet • - Medtronic Hall valve - Omnicarbon (Medical CV) - Monostrut (Alliance Medical Technologies) - Bjork-Shiley valves – Adv • low profile • Good hemodynamics even in small sizes • Excellent durability • Permit central laminar flow • – – – Medtronic hall valve Titanium housing teflon sewing ring carbon coated disc – disadv – • Anticoagulation mandatory • higher risk of thrombosis than cage ball v • sudden catastrophic valve thrombosis

Bileaflet valve St. Jude Medical mechanical heart valve Adv – Low bulk - flat profile Less thrombogenicy Central laminar flow two semicircular discs that pivot between open and closed positions • No need for supporting struts • Good hemodynamics even in small sizes • 2 lat , 1 central minor orifice , no chance of sudden catastro thrombosis Disadv- • • • Anticoagulation mandatory • risk of thrombosis Carbomedics Titanium housing Pyrolytic carbon

Types of prosthetic valves and thrombogenicity Type of valve Model Thrombogenicity Starr-Edwards ++++ Bjork-Shiley, Medtronic Hall +++ St Jude Medical, Sorin Bicarbon, Carbomedics ++ Carpentier-Edwards, Tissue Med (Aspire), Hancock II + to ++ Mechanical Caged ball Single tilting disc Bileaflet Bioprosthetic Heterografts Homografts +
 -")
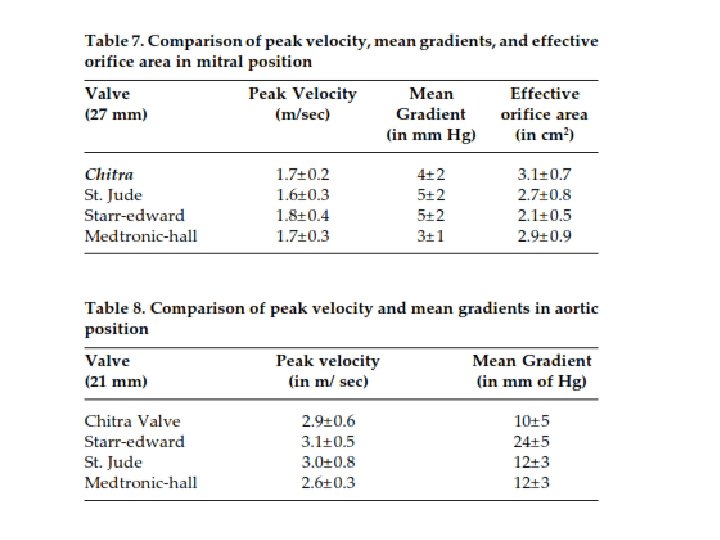
TTK chitra • tilting disc valve - metallic housing (cobalt based wrought alloy) - circular disc high molecular weight polyethylene - A polyester suture ring • Hemodynamically comparable to other mechanical valves • valve related complications are similar

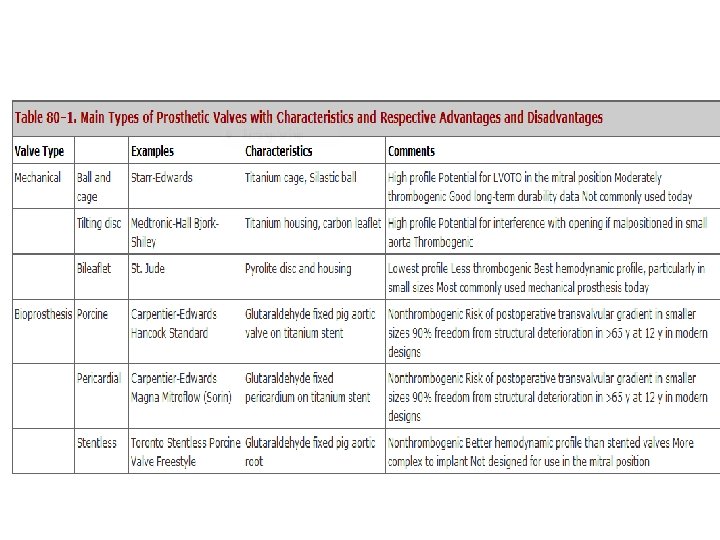
Characteristics of Various prosthetic valves

Flow Dynamics

Desired valves • Mechanical valves - preferred in young patients who have a life expectancy of more than 10 to 15 years who require long-term anticoagulant therapy for other reasons (e. g. , atrial fibrillation) • Bioprosthetic valves preferred in patients who are elderly have a life expectancy of less than 10 to 15 years who cannot take long-term anticoagulant therapy • A bileaflet-tilting-disk or homograft prosthesis is most suitable for a patient with a small valvular annulus in whom a prosthesis with the largest possible effective orifice area is desired.

algorithm for choice of prosthetic heart valve

Radiologic Identification Starr-Edwards caged ball valve Radiopaque base ring Radiopaque cage Three struts for the aortic valve; 4 struts for the mitral or tricuspid valve Silastic ball impregnated with barium that is mildly radiopaque (but not in all models)

TTE – stenosis Valve area calculations • Continuity equation Area Ao prosthesis = (diameter sewing ring)² x 0. 785 x. LVOT VTI/ Ao prosthesis VTI Area mitral prosthesis= (diameter LVOT)²x 0. 785 x. LVOT VTI/ VTI mitral prosthesis • Pressure Half time ( mitral valve prosthesis) • Dimensionless index. LVOT velocity/ aortic prosthesis velocity < 0. 23 indicates prosthetic valve stenosis

Prosthetic Valve regugitation • Mitral – velocity 2. 5 m/sec - jet area 2 cm² • Aortic -- aortic PHT≤ 250 m/sec -- flow reversal in aorta

Normal Doppler Values of Prosthetic Valves Aortic Position Mitral Position Velocity Mean Gr Starr Edward 3. 1± 0. 5 24± 4 St Jude 3. 0± 0. 8 11± 6 Medtronic Hall 2. 6± 0. 3 12± 3 Aortic Homograft 0. 8± 0. 4 7± 3 Hancock 2. 4± 0. 4 11± 2 Carpentier’s 2. 4± 0. 5 14± 6 Velocity Mean. Gr Starr Edward 1. 8± 0. 5 7± 2 St Jude 1. 5± 0. 3 5± 2 Medtronic Hall 1. 6± 0. 3 5± 2 Aortic Homograft 1. 5± 0. 4 4± 2 Hancock 1. 5± 0. 3 5± 2 Carpentier’s 1. 5± 0. 3 5± 2

Importance of TEE • higher-resolution image than TTE • size of vegetation defined more precisely • peri annular complications indicating a locally uncontrolled infection (abscesses, dehiscence, fistulas) detected earlier • limitation -inability to detect aortic prosthetic-valve obstruction or regurgitation, especially when a mitral prosthesis is present

Mitral Bileaflet

Cinefluoroscopy • Structural integrity • Motion of the disc or poppet • excessive tilt ("rocking") of the base ring partial dehiscence of the valve • Aortic valve prosthesis - RAO caudal - LAO cranial Mitral -- RAO cranial

Fluoroscopy of a normally functioning Carbo. Medics bileaflet prosthesis in mitral position A=opening angle B=closing angle

• St. Jude medical bileaflet valve – Mildly radiopaque leaflets are best seen when viewed on end – Seen as radiopaque lines when the leaflets are fully open – Base ring is not visualized on most models

MRI • Not useful in assessing prosthetic-valve structure • used only when prosthetic-valve regurgitation or para valvular leakage is suspected but not adequately visualized by echocardiography

Cardiac Catheterization • measure the transvalvular pressure gradient, from which the EOA can be calculated • can visualize and quantify valvular or paravalvular regurgitation

Valve dysfunction complication example Role of echo Primary mechanical failure Ball variance Strut fracture Visualize structure, assess gradient & regurgitation Nonstructural dysfunction Pt- prosthesis mismatch pannus Gradient, visualize tissue in & around the sewing ring Bleeding event Intracranial hge Source of embolus, presence & mobility of masses Endocarditis Vegetation, abcess, dehiscence Visualize area around the sewing ring, echo dense / lucent area, perivalvular regurgitation Thrombosis Thrombus impedes opening &closing of occluder mechanism Localize mass, assess gradient, detect regurgitation Embolism stroke Identify & characterize the source of emboli

patient-prosthesis mismatch • • • When the effective prosthetic valve area, after insertion into the patient less than that of a normal valve (Rahimtoola in 1978) EOA indexed to BSA is less than 0. 85 cm 2/m 2 EOA (echo) differs from geometric orifice area (measured directly) EOA for each prostheses type & size obtained in literature from pts normally functioning prostheses Average if > 1 value -- mild (0. 9 - 1 cm² /m² -- moderate (0. 6 - 0. 9 cm 2/m² -- severe (i. EOA < 0. 6 cm²/m² (Rahimtoola)

• in-vitro area of the majority of valve prostheses ( int diameter <23 mm) < that of the normal human valve area • the in-vivo prosthetic area further reduced by IVS hypertrophy, progressive endothelialization and tissue ingrowth (Aortic prosthetic devices may be functionally stenotic)

three-step algorithm • Step 1: Calculation of the patient BSA. Step 2: Reference to the specific table for identification of the adequate valvular EOA according to the patient BSA. Step 3: Selection of the most appropriate type and size of valve prosthesis according to the target i. EOA

Valve Thrombosis Incidence of 0. 1 to 5. 7 % per patient-year <0. 2% per year for mech valves <0. 1% bioprosthetic valves • small thrombus, at the hinge portion of a bileaflet valve obstruct the mechanism • tilting disk -- a much larger thrombus to prevent function • Ball and cage valves – less susceptible occluder has no contact at all with the valve housing for a portion of every cycle Clinical – Non obstructive- incidental/embolic phenomenon – Partial obstruction- dyspnea, systemic embolism , fever – Severe obstruction- overt heart failure

• Fibrinolytic therapy - Rt sided thrombosis 80 -100% success rate • Surgery for fibrinolysis failure/symptoms > 3 wk • Surgery – Lt sided thrombosis, large clot burden

FIBRINOLYTIC PROTOCOL heart 2007; 93: 137 -142 • 2 types of protocol -rescue fibrinolysis (short protocol for unstable pt) - long protocol for stable pt • Short protocol - r t. PA 10 mg bolus + 90 mg in 90 min or - SK 15 lac in 60 min • Long protocol -- SK- 5 lac u in 20 min f/b 15 lac u for 10 hr -- rt. PA -- 10 mgbolus f/b 90 mg/hr for 9 hrs • Urokinase – High dose: 4, 500 IU/kg/h for 12 h without heparin – Low dose: 2, 000 IU/kg/h with heparin for 24 h

Embolisation • cerebral embolization CT normal/infarct warf & heparin – 72 hrs APTT lower therapeutic level till the desired INR • anticoagulantion delayed for at least 7 to 14 days ICH, extensive cerebral infarction OAC

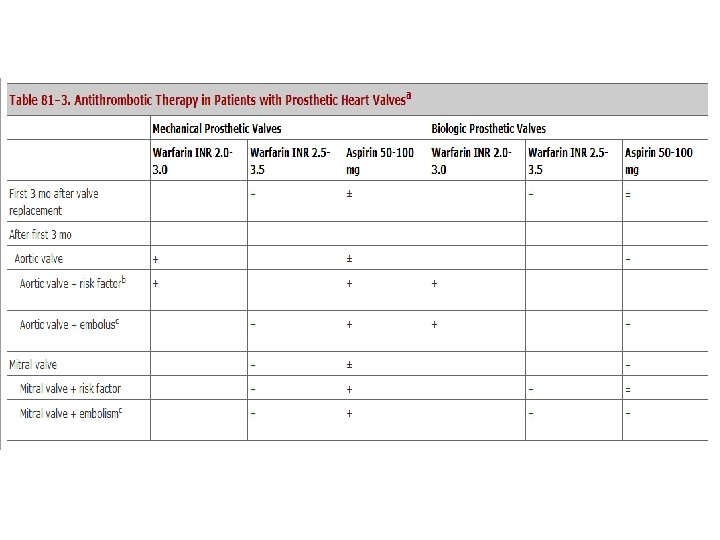
If embolic event occurs while the patient is on adequate antithrombotic therapy • If on warfarin with INR of 2. 0 to 3. 0: increase dose to achieve INR of 2. 5 to 3. 5 • If on warfarin with INR of 2. 5 to 3. 5: add aspirin 50 to 100 mg/d • If on warfarin with INR of 2. 5 to 3. 5, plus aspirin 80 to 100 mg/d: aspirin dose may also need to be increased to 325 mg/d • If on aspirin 325 mg/d: switch to warfarin with goal INR of 2. 0 to 3. 0

Excessive Anticoagulation • vit K 2. 5 mg daily until the INR is acceptable • fresh frozen plasma • Human recombinant factor VIIa, 15 to 19 g/kg (INR >10. 0 with bleeding)

Structural Failure of Bioprosthetic Valves • About 30 % of heterograft bioprosthetic valves and 10 to 20 % of homograft valves require replacement within 10 to 15 years because of structural failure • severe regurgitation due to a tear or rupture of one or more of the valve cusps • calcified and rigid valves • Rarely severe valvular stenosis

Structural deterioration • Higher incidence patients <40 years & with mitral prostheses • gradual onset of dyspnea and other symptoms of heart failure • Bioprosthetic-valve regurgitation or stenosis can be detected by auscultation • valve dysfunction assessed by echocardiography or catheterization

Failure of Bio prosthetic Valves

Hemolysis • Incidence - 6% • Subclinical intravascular hemolysis • severe hemolytic anemia uncommon & suggests paravalvular leakage due to partial dehiscence of the valve or infection • Patients with a caged-ball valve / multiple prosthetic valves have an increased incidence & severity of hemolysis.

Hemolysis • Pts with hemolytic anemia treated with iron & folate supplements or blood transfusion - decreased blood viscosity & increased COP a/w anemia increase the hemolysis • Paravalvular leakage & severe hemolysis – valve replacement or repair

• • • Para valvular leak improper implantation of a valve A heavily calcified annulus is a risk factor for paravalvular leaks -- incomplete debridement of calcium compromises both suture placement and valve seating Active endocarditis is also a risk factor Late paravalvular leaks are suggestive of prosthetic valve endocarditis generally result in hemolysis In the absence of a paravalvular leak, a normally functioning modern valve should not result in hemolysis

Paravalvular Regurgitation • mild or moderate paravalvular leakage asymptomatic , may have only a mild hemolytic anemia - can be observed carefully with serial echo • severe paravalvular leakage - usually have symptoms of heart failure or severe anemia - should be treated with surgical repair or replacement of the valve
 salient features • Endovascular, microbial infection occurring on parts of a")
PVE (2 -6%) salient features • Endovascular, microbial infection occurring on parts of a valve prosthesis or on reconstructed native heart valves , with or without implantation of an annular ring • early PVE is 5% higher in surgery during active IE • Diagnostic approach, surgical indications same

PVE how diff from native? PVE NVE • Early- nosocomial • Late- comm acquired • Mech prosthesis -originate from the sewing cuff /from nearby located thrombi → periprosthetic leaks, ring abscesses, invasion of adjacent tissue • Bioprosthesis infections mostly restricted to the cusps → secondary bioprosthetic failure • Staphylococci, HACEK group, fungi occur more frequently in PVE • Strepto & enterococci found more frequently in native valve endocarditis

• vegetations larger • irreversible adhesion production of a biofilm, inhibit the host defence mech protects against antimicrobial Tt • Duration of Tt longer • Smaller • No such biofilm

Pannus Valve obstruction occurs 5 -10% of mechanical valves per year Thrombus Pannus • mobile, somewhat less echo -dense, associated with spontaneous contrast • Pannus formation -more common in aortic position • fibrous tissue ingrowth • highly echogenic • usually firmly fixed to the valve apparatus • Pre valve jet suggests pannus

MCQ

1. Factors favouring bioprostheses include all except a. Age > 70 yrs b. Bleeding diathesis c. Combined multivalvular placement d. Poor compliance

2. Which of the following favours valve repair? a. RHD b. Endocarditis c. Extensive leaflet destruction d. MVP

3. Which is the most durable mechanical prosthesis? a. St Jude medical b. Medtronic Hall c. Starr- Edwards d. Bjork Shiley

4. Indication for long term anticoagulation in aortic bioprosthesis include all except a. Prior embolic events b. Atrial fibrillation c. Ventricular tachycardia d. LV dysfunction

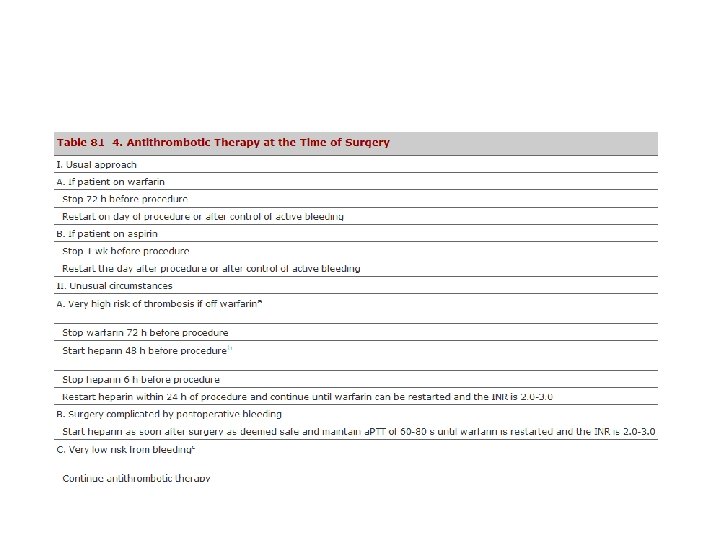
5. 55 yr male, s/p AVR for BAV , SR, good LV function, Dental prophylaxis needed, anti thrombotic therapy would be the following a. Stop warf 72 hrs before procedure, restart after control of bleeding b. Stop warf 72 hrs before procedure, start heparin 48 hrs before procedure c. Stop warf 1 wk before procedure d. Continue warf

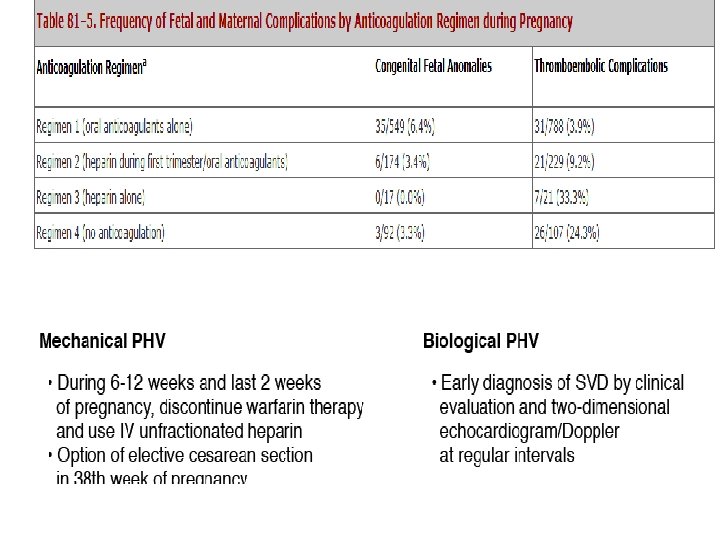
6. Heparin alone regimen in a pregnant lady on OAC, s/p MVR , thrombo embolic complications would be a. 25% b. 33% c. 43% d. 45%

7. Ideal anti thrombotic therapy in a 45 yr female, s/p MVR for RHD, with h/o embolic stroke would be the following a. Warfarin INR 2. 5 - 3. 5, aspirin 50 - 100 mg b. Warfarin INR 2. 0 - 3. 0, aspirin 50 - 100 mg c. Warfarin INR 2. 5 - 3. 5, aspirin 75 - 150 mg d. Warfarin INR 2. 0 - 3. 0, aspirin 75 - 150 mg

8. Prosthetic valve thrombosis would be catastrophic in the following a. b. c. d. Bioprosthesis Tilting disc valve Bileaflet valve Starr- Edwards valve

9. Mitral prostheses best assessed by a. b. c. d. RAO cranial RAO caudal LAO cranial LAO caudal

10. Clinical hemolysis is maximum with a. b. c. d. Caged ball Bioprosthesis Tilting disc Bileaflet
- Slides: 66