Proprioception and Proprioceptive Training Definition PROpreeoSEPshun from Latin

PRO-pree-o-SEP-shun); from Latin proprius, meaning \"one's own\" and")




-(muscle spindle)-(golgi tendon organ) These")











 • Reproduction of positioning:")










- Slides: 36
Proprioception and Proprioceptive Training • Definition: )PRO-pree-o-SEP-shun); from Latin proprius, meaning "one's own" and perception) is the sense of the relative position of neighboring parts of the body. • Sense of orientation of different body parts in relation to each other
proprioception • Is a third sensory modality that provides feedback on the status of the body internally. • It indicates where the various parts of the body are located in relation to each other. • Proprioceptors in the body tell the brain the position of each joint, the tension in the muscle and the pressure on each joint.
• Sensation is the fundamental ingredient that mediates the proprioceptive mechanism. • The articular structures of the body act as sensory chambers which relay proprioceptive information between specific neural pathways within the peripheral nervous system (PNS) and central nervous system (CNS).
Articular structures • Ligamentus tissue within and surrounding movable joint • Muscluotendinous tissue that cross and insert around the joint
• The neural innervations: of articular structures is supplied by peripheral receptors located within the tissue that surrounds these structures (i. e. the joint, muscle and cutaneous (skin) layer). These receptors include • nociceptive free nerve endings that signal pain • mechanoreceptors which signal mechanical deformation of soft tissue, also referred to as "deep touch".
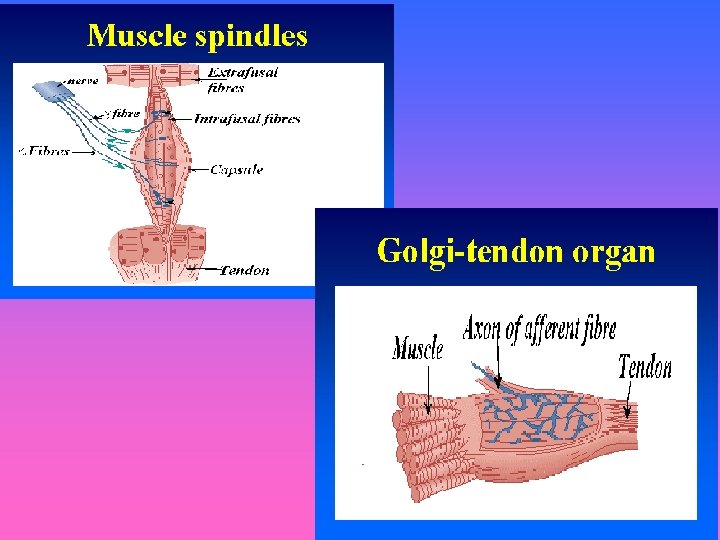
Types of mechanoreceptors • Type I receptors: ( Ruffini endings)-(muscle spindle)-(golgi tendon organ) These receptors have a low threshold for activation, and are slowadapting. • Type II receptors: (Pacinian corpuscle) This receptor is quick adapting, and has a very low threshold for activation. • Type III receptors: (Ruffini corpuscle) This receptor is slow-adapting and has a higher threshold for activation than the type I receptors. • Type IV receptors: ( nociceptive free nerve endings) are sensitive to touch, pressure, and pain.
• Quick-adapting mechanoreceptors, such as the Pacinian corpuscle, decrease their discharge rate to extinction within milliseconds of the onset of a continuous stimulus. • Quick-adapting mechanoreceptors are very sensitive to changes in stimulation and are, therefore, thought to mediate the sensation of joint motion • Slow-adapting mechanoreceptors, such as the Ruffini ending, Ruffini corpuscles, and the muscle spindle/GTO complex, continue their discharge in response to a continuous stimulus. .
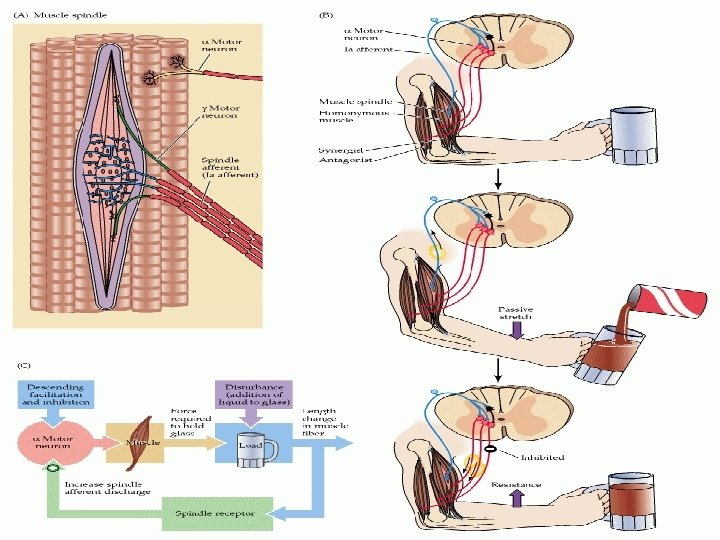
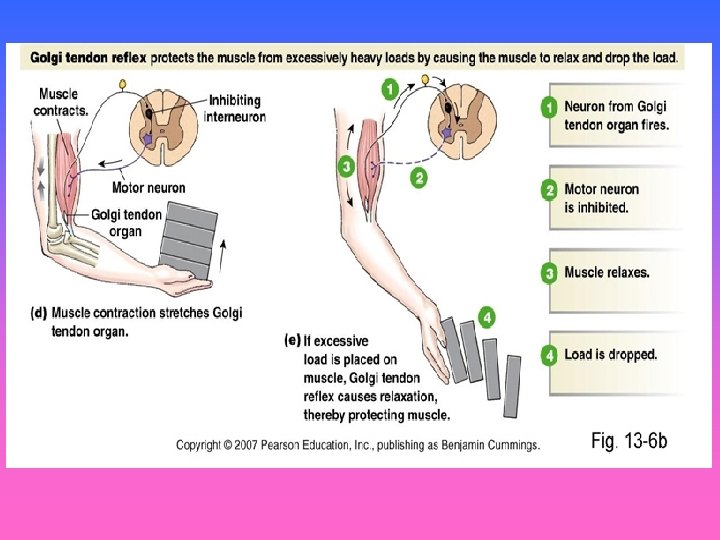
• Mechanoreceptors function by transducing some form of mechanical deformation into a frequency-modulated neural signal which is transmitted via afferent and efferent pathways. • The muscle spindle and GTO using the same pathways function by transducing information concerning muscle length and tension under static and dynamic conditions. The major difference between the function of the muscle spindle and the GTO is that the muscle spindle monitors muscle length, while the GTO monitors muscle tension.
Muscle receptors and joint receptors: • Information about joint motion (rapidly adapting receptors, e. g. Pacinian corpuscles), • Information about joint position (slowly adapting receptors, e. g. Ruffini endings and corpuscles, and the muscle spindle/GTO complex), • pain and touch (free-nerve endings).
• Proprioception versus kinesthesia Kinesthesia is another term that is often used interchangeably with proprioception, though use of the term "kinesthesia" can place a greater emphasis on motion. Some differentiate the kinesthetic sense from proprioception by excluding the sense of equilibrium or balance from kinesthesia. An inner ear infection, for example, might degrade the sense of balance. This would degrade the proprioceptive sense, but not the kinesthetic sense. The affected individual would be able to walk, but only by using the sense of sight to maintain balance; the person would be unable to walk with eyes closed.
• Kinesthesia is a key component in muscle memory and hand-eye coordination, and training can improve this sense. The ability to drive a car or to catch a ball requires a finely-tuned sense of the position of the joints. This sense needs to become automatic through training to enable a person to concentrate on other aspects of performance, such as maintaining motivation or seeing where other people are
• The mechanism of proprioception There are many receptors within joints, muscles and skin that continually convey information to the central nervous system (CNS). Using this information we continually make subconscious and conscious modifications to how we move, allowing us to carry out normal functional activities. • Each receptor supplies a different type of information: joint pressure, joint acceleration/deceleration and joint velocity. • When the receptors are stimulated through movement or other forces, they act as transducers and convert this mechanical deformation into an electrical sensory impulse. This sensory impulse then passes onto the CNS, triggering the appropriate motor response.
walking on uneven ground
• The large volume of proprioceptive information entering the CNS is utilized at three different levels: • Spinal level. Reflex contraction occurring at this level contributes to reflex stability within a joint, helping to reduce the risk of injury from sudden forces acting on the joint. • Brainstem. This is the part of the brain which receives input from the vestibular centers in the eyes and ears and helps to control balance. • Motor cortex. Cerebellum and basal ganglia, responsible for control of complex movement pattern.
• Instability • The word "instability" is frequently encountered when dealing with patients who display reduced proprioception. Instability can effectively be divided into two types: • Mechanical (true) instability. Disruption of the ligamentous structure of the joint produces disability. This is the type of instability detected by manual testing- for example valgus stress testing at the knee to test the medial collateral ligament. • Functional instability. Ligamentous structure is intact with no laxity detected through manual testing. The patient, will, however, complain of symptoms such as giving way "low limb" or pain and heaviness "upper limb". The problem is one of poor neuromuscular control.
valgus stress testing
Potential causes of functional instability within a joint. Cause Rationale Articular mechanoreceptors are damaged, deafferentation reducing the afferent impulse to the CNS, resulting in a decreased motor response. Differentiation Trauma can result in direct damage to the motor supply, resulting in a decreased muscular control over the joint. Neurogenic It may be related to joint inflammation and Inflammation inflammatory mediators directly affecting the motor endplate and therefore the motor response. Capsular distension Joint effusion following trauma can cause muscle inhibition, leading to instability.
ASSESSING PROPRIOCEPTION • Threshold to detection of passive movement (TTDPM) • Reproduction of positioning: 1. Reproduction of passive positioning 2. Reproduction of active positioning
• Proprioceptive rehabilitation of the limbs • The key aims of proprioceptive rehabilitation are: • To provide early afferent input to the joint • To restore reflex stability • Restore neuromuscular coordination • To enhance the neuromuscular response
Wobleboard
Wobleboard work in sitting
How to progress proprioceptive exercises. • • • Removing visual stimulus Altering the base of support Increasing weight-bearing Increasing speed of an activity Making an exercise more complex(more than one type of exercises at the same time(
Altering the base of support with proprioceptive exercises
lower limb proprioceptive exercises
lower limb proprioceptive exercises (double leg stance on (wobble board
lower limb proprioceptive exercises holding a ball and throwing it
Arm and leg movement while carrying a board on trunk