Prolonged labour Definition The labour is prolonged when

Prolonged labour


Definition The labour is prolonged when the combined duration of the first and second stage is more than the arbitrary time limit of 18 hours. [ D. C. Dutta] Prolonged labour is defined when the first and second stage of labour last more than 24 hours, currently duration is taken as more than 18 hours. Duration of labour is calculated from mother’s subjective estimate of labour onset [Dawn]

Prolongation due to Ø Protracted cervical dilatation in the first stage Ø Inadequate descent of the presenting part during the first or in the second stage Ø Labour considered prolonged when the cervical dilatation rate is < 1 cm/hr and the descent of the presenting part is < 1 cm/hr for a period of minimum 4 hours observation.

Types of prolonged labour v Hypotonic uterine dysfunction: due to low intensity uterine contractions. general factors ü Elderly primi gravida ü Anemia ü Nervousness, anxiety and fear ü Hormonal ü Improper use of analgesics local factors over distention of uterus developmental anomalies myomas of uterus mal presentations, CPD malpositions full bladder and rectum

Cont… v Hypertonic uterine dysfunction: it can be a. Incordinate uterine action b. colicky uterus c. Asymmetrical uterine dysfunction d. Hyperactive lower segment e. Constriction ring dystocia v. Cervical dystocia: cervix becomes thin and fails to dilate within a reasonable time inspite of good uterine contractions.

Cervical dystocia In coordinate uterine action

Incidence Primi gravidae 25% Multi gravidae 2%

Risk factors of prolonged labour ü age and parity: commonly primigravidae, more in elderly one ü CPD and fetal malposition ü Uterine distention- twins, hydramnios ü Uterine defect- fibroid, malformation ü Nervousness, fear and emotion ü injudicious use of analgesia in labour ü injudicious induction of labour by ARM and oxytocin drip. ü unknown cause.
![Causes of prolonged labour Faults in power [commonest cause] *inefficient uterine dysfunction *constriction ring](http://slidetodoc.com/presentation_image_h2/8c09291f6b987051ca71672acfa62a1f/image-10.jpg "Causes of prolonged labour Faults in power [commonest cause] *inefficient uterine dysfunction *constriction ring")
Causes of prolonged labour Faults in power [commonest cause] *inefficient uterine dysfunction *constriction ring *cervical dystocia *over dose of sedative and analgesics * epidural analgesia *improper use of oxytocics

Cont… Faults in passage: ü PROM ü Contracted pelvis ü CPD ü Cervical stenosis ü Fibroid or carcinoma ü Ovarian tumor ü Uterine fibroid 20%

Engagement & descent of the foetal head presence of cephalopelvic disproportion

Engagement & descent of the foetal head presence of cephalopelvic disproportion

Cont… Faults in passenger: ü Occipito posterior positions of vertex ü Other malpresentations ü Twins ü Hydramnios[ 30%]

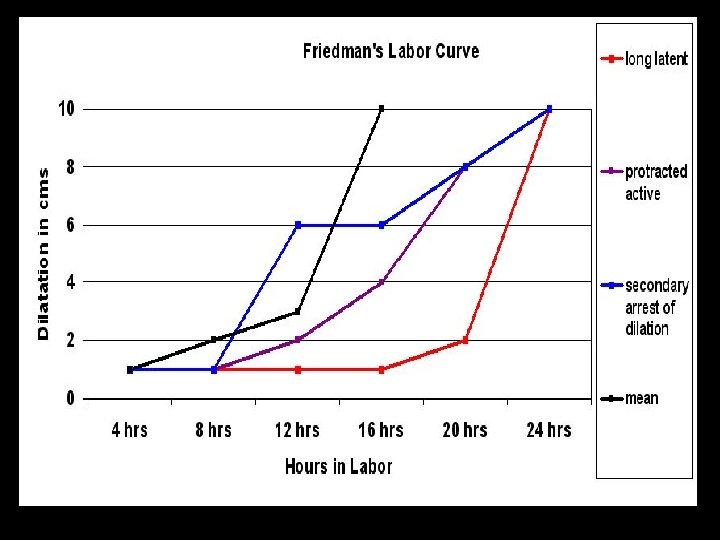
Labour disorders due to inefficient uterine action prolonged latent phase beyond 12 hours a. Hypotonic or hypertonic dysfunction b. Predisposing factors are sedation, anaesthesia , false labour, unknown cause. Prolonged active phase[ protraction disorder] Ø Slow rate of cervical dilatation below 1 cm/hr in nullipara and 1. 5 cm/hr in multipara Ø Caused by hypotonic dysfunction, hyperactive lower segment. Ø Predisposing factors : CPD, fetal malpositions and sedation

Cont… secondary arrest of cervical dilatation or head descent Ø Arrest of cervical dilatation is taken when there is no cervical change for 2 hrs. Ø there is head descent less than 1 cm/hr in nullipara or less than 2 cm/hr in multipara and no head descent for one hour. Ø Due to hypotonic dysfunction and incordinate uterine dysfunction. Ø The causative factors are occipito posterior positions [70%], pelvic contraction , excessive sedation.
![DIAGNOSIS Clinical features Hypotonic dysfunction [more frequent] 1. Timing of dysfunction [more frequent] 2.](http://slidetodoc.com/presentation_image_h2/8c09291f6b987051ca71672acfa62a1f/image-17.jpg "DIAGNOSIS Clinical features Hypotonic dysfunction [more frequent] 1. Timing of dysfunction [more frequent] 2.")
DIAGNOSIS Clinical features Hypotonic dysfunction [more frequent] 1. Timing of dysfunction [more frequent] 2. Labour pains At latent phase from start of labour usually running to active phase Less painful, short lasting, infrequent abdominal pain and no back ache Hypertonic dysfunction [ less frequent] Latent phase from start of labour Severely painful , prolonged lasting, frequent pain as abdominal colic or as backache , desire to bear down during contraction with incompletely dilated cervix.

Cont… 3. membranes 4. Cervical dilatation Remains intact slow 5. Fetal head Caput develops late 6. Fetal distress Appears late Ruptures early Slow. it hangs thick lipped without pressure of head. Caput develops even before rupture of membranes Appearing early

Cont… 7. Maternal effect 8. Difficult labour little Same in both groups She becomes distressed in pain, goes to dehydration and acidosis early.

Cont… Other measures such as : ü radiography, CT or MRI ü Abdominal and vaginal examination. ü partograph

Cont… First stage: is considered prolonged Ø When the duration of labour is more than 12 hrs Ø The rate of cervical dilatation is < 1 cm / hr in a primi and < 1. 5 cm/ hr in a multi Ø when the cervicograph crosses the alert line and falls on zone 2 Ø Intervention is required when the cervico graph crosses the action line and falls on zone 3

Cont… Secondary arrest : is defined when the active phase of labour ( cervical dilatation ) commences normally but stops or slows significantly for 2 hrs or more prior to full dilatation of the cervix. It is commonly due to malposition or CPD

Cont… Second stage: is considered prolonged When it lasts for more than 2 hrs in primi and 1 hr in multi. Diagnosis : Sluggish or non descent of the presenting part even after full dilatation of the cervix. ( failure of head descent within 1 hr of full dilatation is called protraction of descent. ) Variable degrees of molding and caput formation in cephalic presentation. Identification of the course of prolongation.
 Maternal effects: Distress PPH Trauma to genital tract Increased operative delivery Puerperal sepsis")
Dangers(Complications) Maternal effects: Distress PPH Trauma to genital tract Increased operative delivery Puerperal sepsis Sub involution.

Cont… Fetal effects : Hypoxia Intra uterine infection Intra cranial stress or hemorrhage Increased operative delivery

Management Prevention : Antenatal or early intra natal detection of the factors likely to produce prolonged labour. Use of partograph Selection and judicious augmentation of labour by low rupture of the membranes followed by oxytocin drip. Change of posture in labour, other than supine to increase uterine contractions, avoidance of dehydration in labour and use of adequate analgesia for pain relief.

Cont… Actual Rx: Careful evaluation to find out Cause of prolonged labour Effect on the mother Effect on the fetus

Cont… Definitive Rx : First stage patient is referred to level 11 care without any solid food. Only water is allowed orally. Maintain partograph Identify or diagnosis of hypotonic and hypertonic labour dysfunction. Monitor maternal vital signs and FHS Identify CPD or fetal mal position. Maintain I. V line with 5% DW/RL Antibiotics ( cefazoline ) 1 gm I. V and repeated after 6 hrs on PROM

IN CASE OF PROM GROUP A: Hypotonic uterine dysfunction Os 3 cm on 12 hrs labour since admission on vertex presentation. CPD excluded. FHS normal Artificial rupture of membrane , if liquor shows meconium CS. If liquor clear wait for 60 min. for improvement of contractions Otherwise – oxytocin 5 units. 500 ml 5% dectrose in primi or 2 units in 500 ml DW in multi. Fetal monitoring is done. If failure to progress or fetal distress GROUP B: Hypertonic uterine dysfunction Os 3 cm at 12 hrs labour since admission; i. v. 5% DW and RL is set up Nothing by mouth Inj. Pethedine 100 mg, phenergan 25 mg, continuous epidural or caudal analgesia if available. CPD is evaluated FHR monitoring done on recovery from sleep , her hypertonic dysfunction may improve. Uterine hyper tone Persists, fetal distress C. S Uterus relaxes AROM oxytocin, wait for Vaginal delivery CS CS

Cont. . Group A: Second stage Head at outlet, FHS normal; AROM. If membranes present followed by oxytocin drip for uterine dysfunction Failure to progress Low forceps/ vacuum extraction if late referral/ dead fetus/malformed fetus Oxytocin drip Craniotomy delivery Group B: Second stage Cervical dystocia, Duhrssen’s incision is made at 3 o’ clock and 9 o’ clock position on cervical lip by applying forceps or vacuum extractor, thus delivery is done. For constriction ring, vaginal delivery can be done under deep general anaesthesia if fetus is not distressed

Cont… • Third stage actively managed • Neonatal care is important due to meconium aspiration

Nursing diagnosis • Risk for injury to mother and fetus • Fatigue and exhaustion related prolonged efforts and pain • Anxiety related to process and outcome of labour • Knowledge deficit related to labour process

- Slides: 35