Procedures pediatrics emergencies BagMask Ventilation INDICATIONS To ventilate

Procedures pediatrics emergencies

Bag-Mask Ventilation
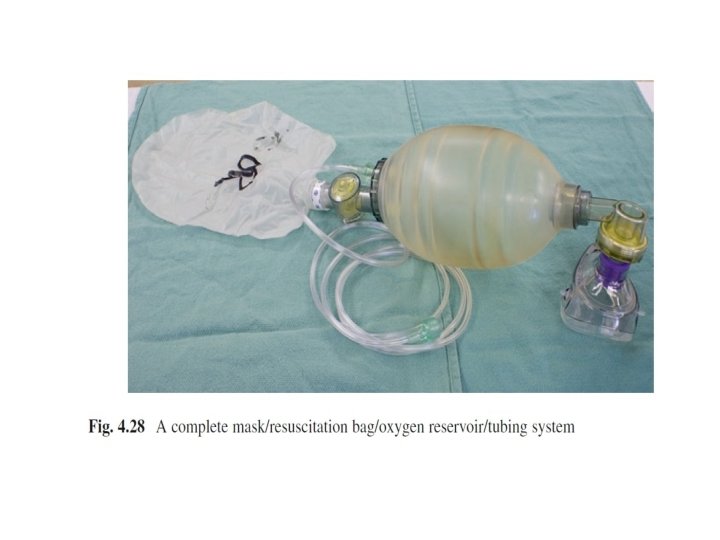

• INDICATIONS • ■To ventilate and oxygenate a patient. • ■A ventilation face mask may be used with an oropharyngeal or nasopharyngeal airway during spontaneous, assisted, or controlled ventilation • RISKS • ■Vomiting and aspiration

• PEARLS AND TIPS • ■Bag-mask ventilation gives the clinician time to prepare for more definitive airway management. • ■Good technique involves preserving good mask-face seal, inflating the chest with minimal required pressure, and maintaining the optimal patency of the upper airway through manipulation of the mandible and cervical spine

• MONITORING ■Use pulse oximetry to measure oxygen saturation levels continuously. ■Measure heart rate continuously. ■Check blood pressure using a noninvasive device. ■Ensure the chest rises visibly.

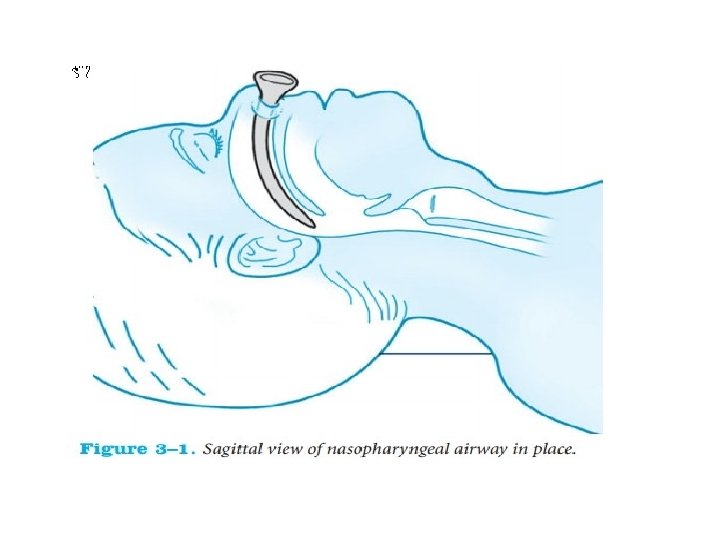
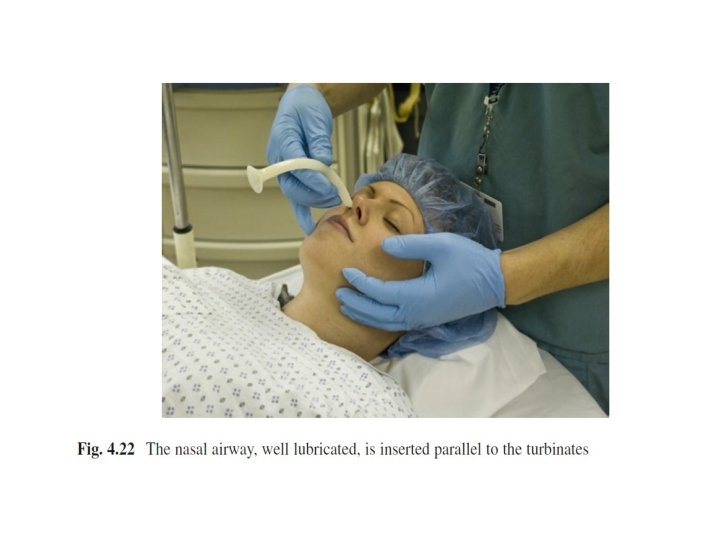
Nasopharyngeal airways • INDICATIONS ■Nasopharyngeal airways provide a conduit for airflow between the nares and the pharynx. ■Nasopharyngeal airways prevent mandibular tissue from obstructing the posterior pharynx. ■Nasopharyngeal airways may be used in conscious patients. ■Nasopharyngeal airways may be used in children with impaired consciousness or in neurologically impaired patients with poor pharyngeal tone leading to upper airway obstruction. ■Nasopharyngeal airways can be used to suction secretions

• CONTRAINDICATIONS • Absolute • ■Nasal airway occlusions. • ■Nasal fractures. • ■Coagulopathy (because of the risk of epistaxis). • ■Cerebrospinal fluid leak. • ■Basilar skull fracture. • ■Adenoidal hypertrophy

• COMPLICATIONS • ■If the nasopharyngeal airway is too long, it may cause bradycardia through vagal stimulation or it may injure the epiglottis or vocal cords. • ■Physical irritation of the larynx or lower pharynx may stimulate coughing, vomiting, or laryngospasm (if the tube is too long). • ■Nasopharyngeal airways can cause a pressor response with increased blood pressure.

• ■Failure of insertion. • ■Epistaxis (due to mucosal tears or avulsion of turbinates). • ■Submucosal tunneling and pressure sores. • ■Perforation of cartilage into the sinuses. • ■Stimulation of nasal secretions with obstruction of the tube. • ■Prolonged placement of a tight fitting tube may lead to nasal necrosis

endotracheal tube


• INDICATIONS • Respiratory • ■Apnea. • ■Acute respiratory failure (Pa. O 2 < 50 mm Hg and Pa. CO 2 > 55 mm Hg). • ■Need to control oxygen delivery (eg, institution of positive end-expiratory pressure [PEEP], accurate delivery of FIO 2 > 0. 5). • ■Need to control ventilation (eg, to decrease work of breathing, to control Pa. CO 2, to provide muscle relaxation).

• Neurologic • ■Inadequate chest wall function (eg, in patient with Guillain-Barré syndrome, poliomyelitis). • ■Absence of protective airway reflexes (eg, cough, gag). • ■Glasgow Coma Score ≤ 8. • Airway • • ■Upper airway obstruction. ■Infectious processes (eg, epiglottis, croup). ■Trauma to the airway. ■Burns (concern for airway edema)

• CONTRAINDICATIONS • Absolute • ■Nasotracheal intubation is contraindicated in patients with nasal fractures or basilar skull fractures

• RISKS • • ■Desaturation. ■Bradycardia. ■Inability to intubate. ■Tracheal tear or rupture

• Confirm Correct Position of Tube ■Auscultation for symmetric breath sounds. ■Good chest excursion. ■Effective oxygenation. ■Disposable colorimetric capnometer (color should change from purple to yellow if patient has a perfusing rhythm) or capnograph. • ■Obtain chest radiograph. • ■Absence of breath sounds over the upper abdomen. • ■If unilateral breath sounds are heard on the right, pull back the tube slowly while ventilating and listen for breath sounds on the left (probable intubation of right main bronchus) • •

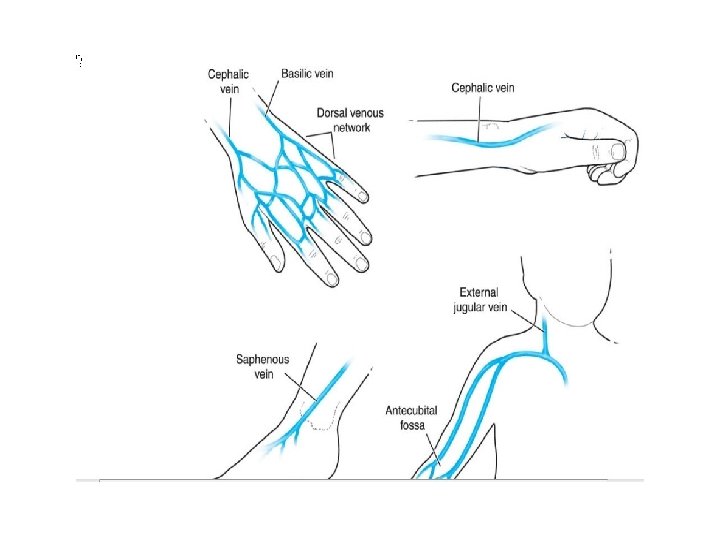
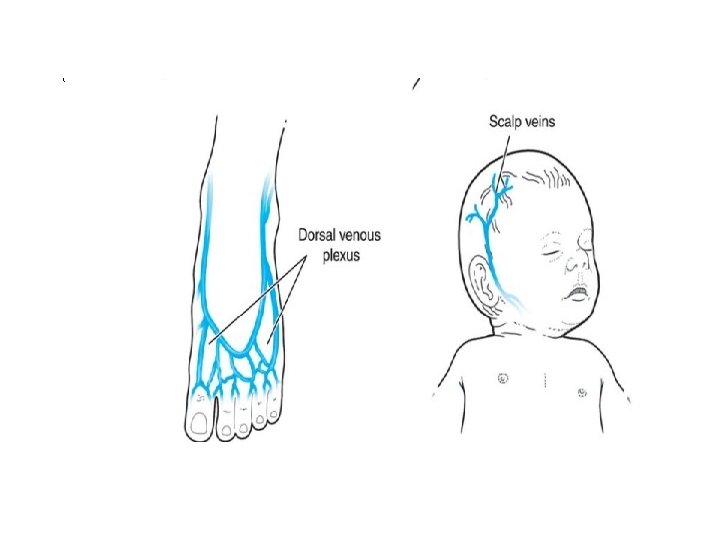
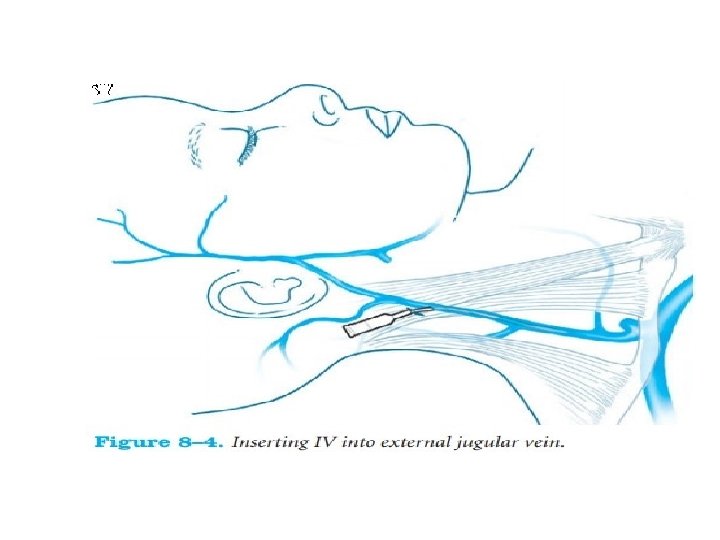
Peripheral IV Insertion • INDICATIONS • ■Vascular access in nonemergent situations • • or temporary access in emergent situations. ■Administration of fluids and electrolytes. ■Administration of intravenous medications. ■Administration of blood and blood products. ■Blood sampling

CONTRAINDICATIONS • • Absolute ■Do not insert through an infected site. ■Do not insert through a burn. ■Do not insert in an injured site. Relative ■Avoid a paralyzed extremity. ■Do not insert in a massively edematous extremity. ■Avoid joint area

RISKS • ■Infection. • ■Hematoma. • ■Extravasation. . • ■Severe vasoconstriction if vasoactive medications are infused through a peripheral IV and extravasate. • ■Venous thrombosis. • ■Embolization of air or catheter fragment

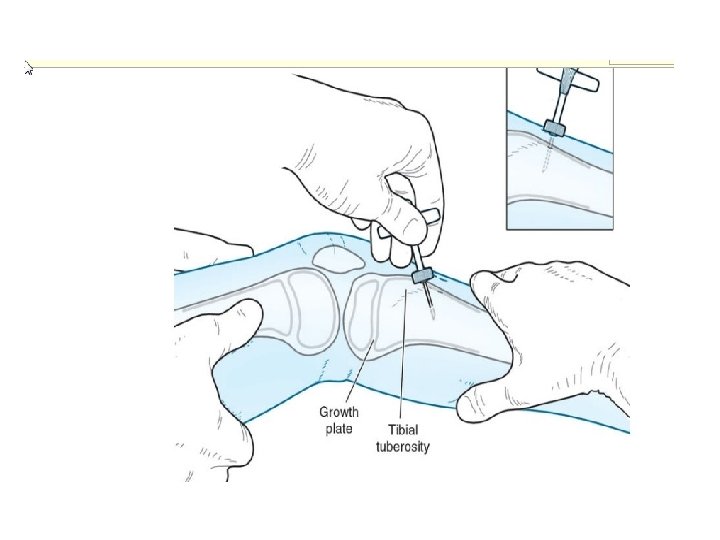
Intraosseous Line Insertion • INDICATIONS • ■Emergent temporary vascular access during cardiopulmonary resuscitation or during the treatment of uncompensated shock when unable to insert an intravenous line. • ■Volume resuscitation. • ■Administration of blood and blood products. • ■Administration of fluids and electrolytes. • ■Administration of medications. • ■Infusion of inotropes and pressors. • ■Sampling of blood and bone marrow.

CONTRAINDICATIONS • Absolute • • ■Do not insert in a recently fractured bone. ■Do not insert through an infected site. ■Osteogenesis imperfecta. ■Osteopetrosis. • Relative • ■Osteoporosis or osteopenia. • ■Cystic bones.
 is")
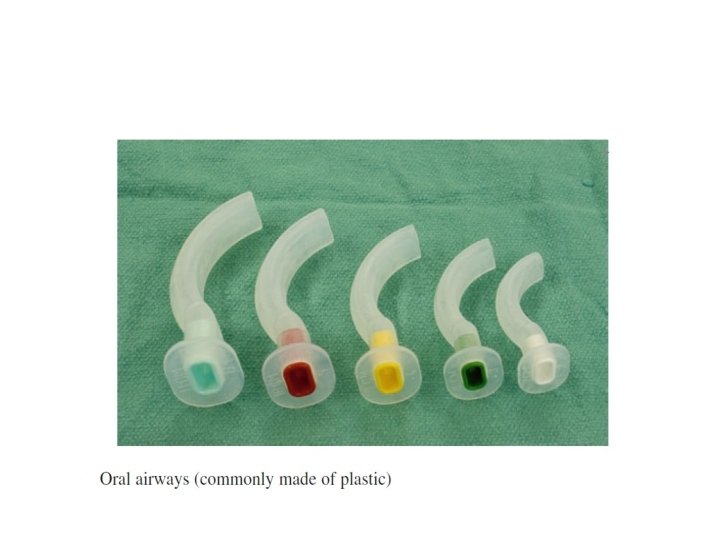
Oropharyngeal airway • An oropharyngeal airway (also known as an oral airway, OPA) is a medical device called an airway adjunct used to maintain a patent (open) airway. It does this by preventing the tongue from covering the epiglottis,

Indications • Airway maintenance in the unconscious patient • Protects an Endotracheal Tube from being bitten • Facilitates Airway Suctioning

Complications • Oral Airway too long – Obstructs Larynx by forcing down epiglottis • Oral Airway too short – Tongue obstruction of airway • Vomiting and laryngospasm in the awake patient

• Contraindications for an OPA • would be; 1. Patient is conscious. 2. Patient has a gag reflex. 3. There is some foreign body that is blocking the airway, such as food, dentures, etc that should be removed first.

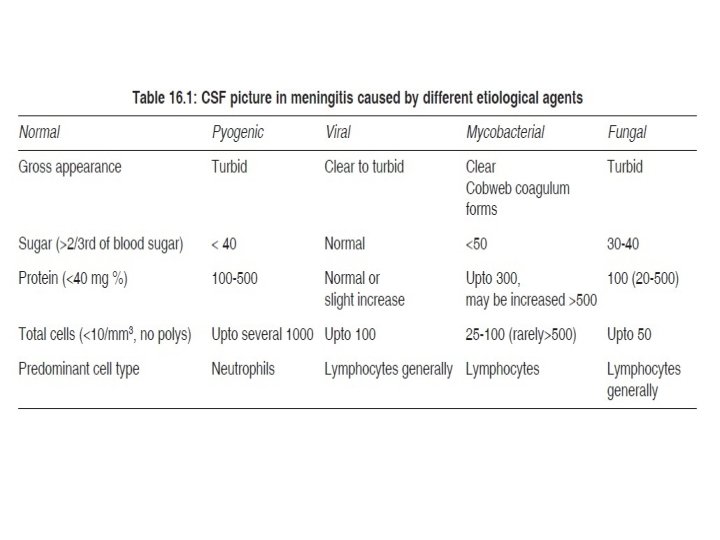
LP
 Bleeding diathesis Skin infection at puncture site")
Contraindications • • increased intracranial pressure (ICP) Bleeding diathesis Skin infection at puncture site Sever ill child

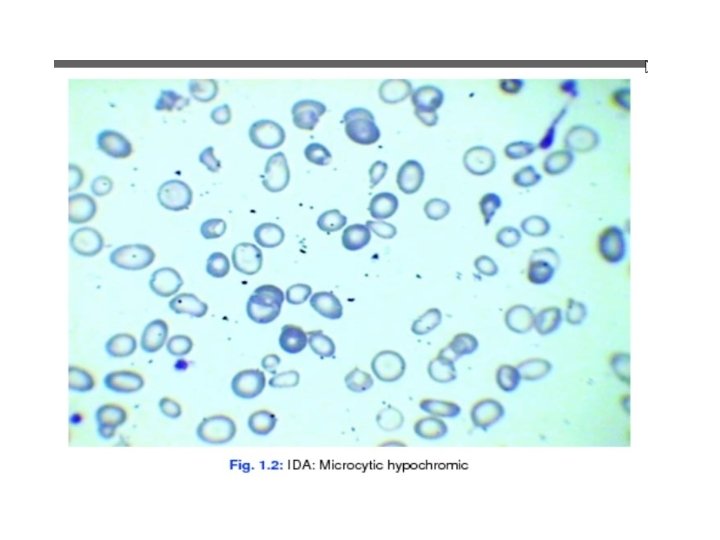
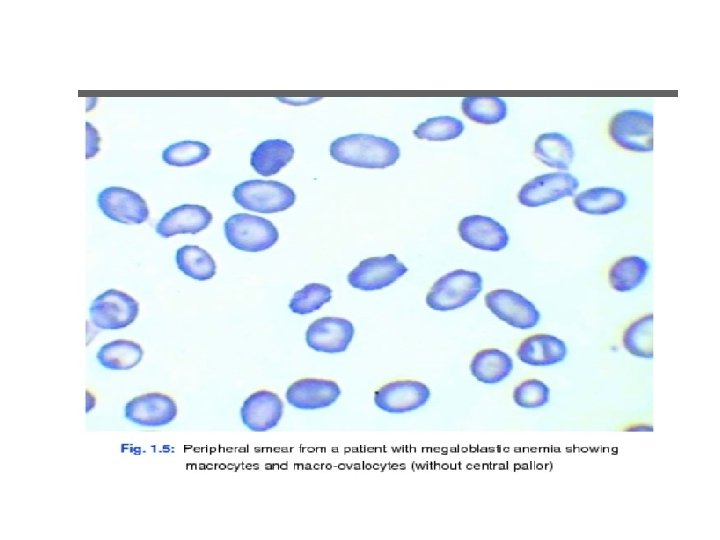
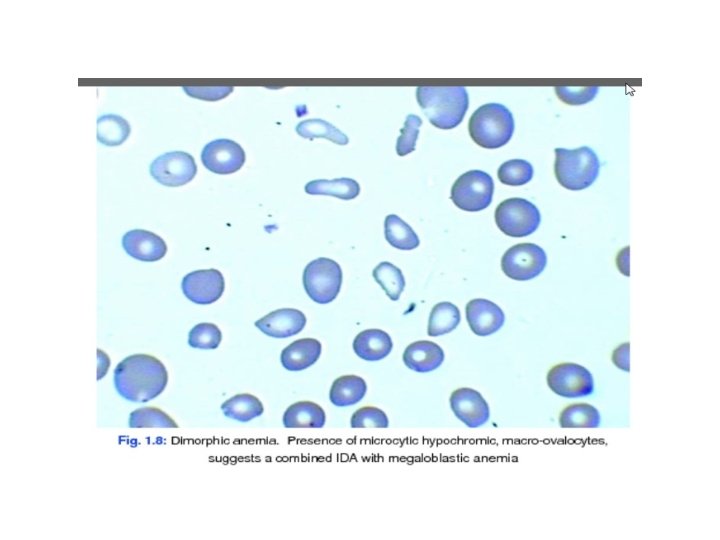
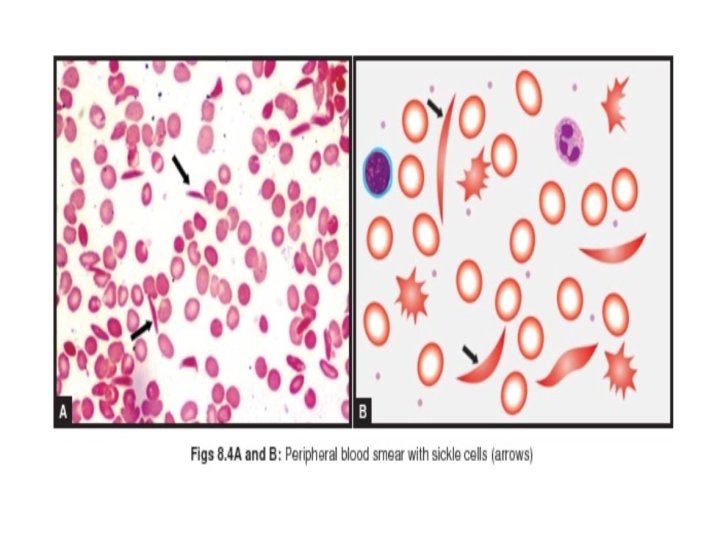
Blood films

Thank you
- Slides: 44