Procedure World Competency The Next Generation Teaching and


























 2 nd year? • More time in the office. • Basic")



 POST-TEST (%) 1 68 85 2 57")

 – “…significant numbers of residents")




- Slides: 39
Procedure World & Competency: The Next Generation Teaching and Evaluating Procedural Skills
John Sheffield, MD Ellen Johnson, MD Penn State/Good Samaritan Family Practice Residency Program Lebanon, PA
Overview • Introduction • Nuts & Bolts - How we do it – Sessions – Models – Faculty • Evidence that it works • Resident satisfaction • Looking towards the future…Competency Evaluations
Introduction • Everyone agrees, “Family Medicine should include procedural training”, but…
Standards for teaching? There are none.
Number needed for competency? There are no numbers.
Consistency from one residency to another? There is none.
What does the ACGME say? “The primary responsibility for the determination of procedural competency rests with the program director and faculty. ” “At the time of program review, the program will need to demonstrate how It assesses competency of residents. ”
Penn State/GSH FP Residency • Two week procedural workshop rotation • Occurs in second half of September of second year • Each half-day session includes didactics plus hands-on practice • Most taught by our FP faculty • Two patient care sessions per week
Procedures We Teach • ALSO Course • Endometrial Sampling • Billing/Coding for • Episiotomy Repair Procedures • Breast Cyst Aspiration • IUD Insertion • Joint • Casting/Splinting Injection/Aspiration • Colonoscopy • Neonatal • Colpo with Biopsy Resuscitation Review • Dermatologic • Suturing Workshop Procedures • Umbilical Vein Cath.
Billing & Coding for Procedures • 60 -90 minute session • Objectives – Use of -25 modifier – Billing for materials – Cosmetic procedures not typically covered by payers • Pre- and Post tests
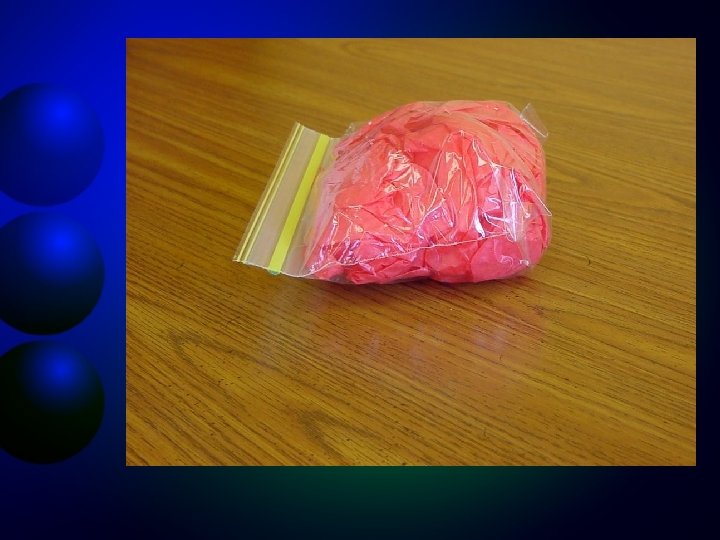
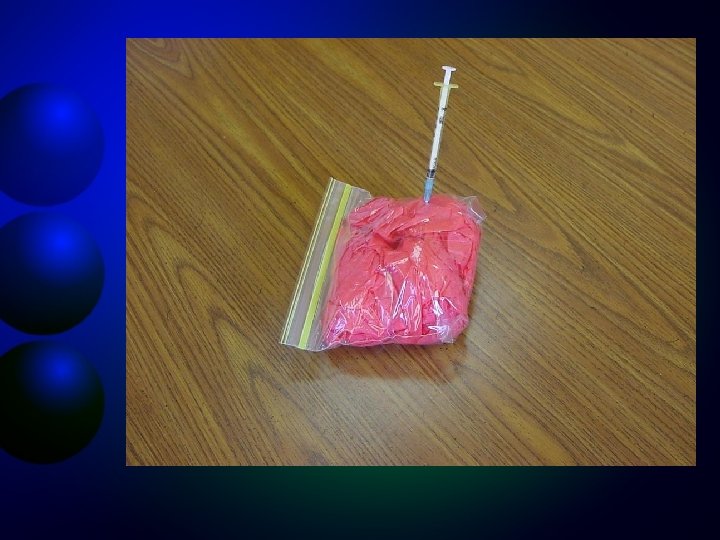
Breast Cyst Aspiration • Combine with Endometrial Sampling • Didactic session covers evaluation of breast mass • Model uses: – Ziploc sandwich bags – Wrapping tissue – Scented Bath beads
Casting/Splinting • Half-day session • Concentrates on splinting • Residents practice on each other
Colonoscopy • Half-day session • Didactics covers colon CA and screening • Accu. Touch Endoscopy Trainer
Colposcopy w/ Biopsy • Taught in 2 halfday sessions – Half-day of didactics – Half day of practice • Also covers cervical cryo
Colposcopy Model • Model uses: – Plastic cup – Hot Glue Gun – Piece of chuck steak – White-out – Freezer
Dermatologic Procedures • One half-day • Multiple procedures – Toenail removal – Electrocautery – Biopsy • Shave • Excision • Punch – Cryo – Anesthesia techniques
Endometrial Sampling • Half-day session with Breast cyst Aspiration • Didactic session covers: – Endometrial CA – Evaluation of Postmenopausal bleeding
Episiotomy Repair • Half-day session • Model borrowed from Family Centered Maternity Care
IUD Insertion • • Mirena • Had 2 -hour session with all residents (new procedure for us) • Used company’s models.
Joint Injection/Aspiration • Half-day session • Didactics covers multiple joint anatomy • Use Sawbones Models – Beeps when joint entered • Residents often practice on each other
Sawbones Models
Neonatal Resuscitation Review • Taught by our IM/Peds Faculty member • Reviews Umbilical Vein Catheterization
Why (wait until) 2 nd year? • More time in the office. • Basic rotations completed. • Still have 2 years to “practice” doing procedures. • Able to pay more attention to subtle nuances of the office (i. e. , billing and coding).
Why the ALSO Course? • Resident take the course for the first time during Orientation (July of first year). • Much more learned after 2 months of OB rotation.
Why not send them out to a conference? • Residents learn to do procedure in your setting with your equipment. • Residents learn how to bill and code on your encounter forms. • Residents learn from the faculty who will be supervising them.
Other benefits… • Only 6 residents – More one-on-one teaching • Residents get to spend time together as a class – Good for morale and bonding • Half-day sessions allow thorough review of each procedure.
Do they really learn? RESIDENT PRETEST (%) POST-TEST (%) 1 68 85 2 57 83 3 78 95 4 70 92 5 63 93 6 57 93
One year later… RESIDENT 2004 2005 1 87 % 85 % 2 95 % 87 % 3 80 % 77 % 4 93 % 70 % 5 80 % 6 88 % 83 %
Resident Satisfaction • Study from 2003 (Sharp, et al) – “…significant numbers of residents are not being taught certain procedures in a manner that results in residents feeling competent to perform them”.
Comfort Level – We ask our residents to rate this statement: I now feel comfortable doing this procedure under supervision • Average rating is 1. 27 (Likert scale with 1 = Strongly agree to 5 = strongly disagree) • Lowest rating is for Flexible sigmoidoscopy – Score of 2 – Procedure that definitely requires practice
Comments from Residents • My level of confidence was really elevated with this 2 -week procedure learning. • Excellent workshop; learned a lot of things that are very important for FP. • Cleared up a lot of confusion with billing and the 25 modifier. • I am better prepared to do procedures.
Practical Skills Assessment • Incorporate practical section of testing – Would include evaluation of “critical steps” needed to do each procedure correctly. – Done with the same models used in workshop – Set up in “stations”.
Competency Checklists • Detailed list of critical steps necessary to competently perform each procedure. • Each step rated as: – Not competent – little/no knowledge – Partially competent – able to perform with prompting – Fully competent – needs little/no prompting