Private Practice with a Focus on Eating Disorder











 & Credentialing NPI: Which https: //nppes.")


















 Disorder characterized by behaviors that")


















, Guide to Private Practice (Academy), Counselling")

- Slides: 52
Private Practice with a Focus on Eating Disorder Treatment Nicole Lefever, MS RDN LDN
Intro- Nicole in a Nutshell ED Treatment Experience Remuda Ranch Private Practice Experience Mid Atlantic Nutrition Specialists, LLC Disordered Eating Pediatrics PCOS Other Nutrition Experience Bariatrics & Weight Management Lancaster General Health Heart of Lancaster Regional Medical Center
Now it’s your turn…. Brand New RDNs? Outpatient nutrition counseling in a hospital or clinic setting? Private Practice RDNs? Want to be a private practice RDN, but haven’t taken the leap yet? RDNs who don’t want to touch eating disorder treatment with a 10 foot pole?
Objectives for Today Overview Basics of Private Practice- is it for you? of treating clients with eating disorders
Private Practice
You might be a private practice RDN if… You love the idea of getting paid for empowering clients to change their lives You have a “the sky’s the limit” mentality You aren’t scared to take risks You can handle uncertainty with income and benefits You are ready to be the boss (and the billing specialist, and the receptionist, and the janitor…)
PROS & CONS PROS Set your own hours Unlimited earning potential Limited Red Tape YOU are the decision maker CONS You do EVERYTHING PTO? What’s that? Limited checks & balances Healthcare benefits, etc. Professional Isolation
Consider when you’re getting started… Physical Location Prices/Rates Reimbursementinsurance vs. self pay Referral Sources Specialties Hours/Schedule Marketing Accounting Business Policies Medical Records Your Insurance
Private Practice Location Options • Doctor/Provider’s Office • Office Share/ Sublet • In Home (yours or theirs) • Private Office • Other Company: gym, spa
Rates & Reimbursement How to set your rates? Consider your Expenses: Rent Phone/Internet Marketing Materials & Business Supplies Professional Insurance, Dues, CEUs Private Pay Model vs. Insurance Reimbursement
Private Pay Cash/Credit/Check Pay. Pal Square Traditional Super Credit Card Machine bill/Medical Receipt
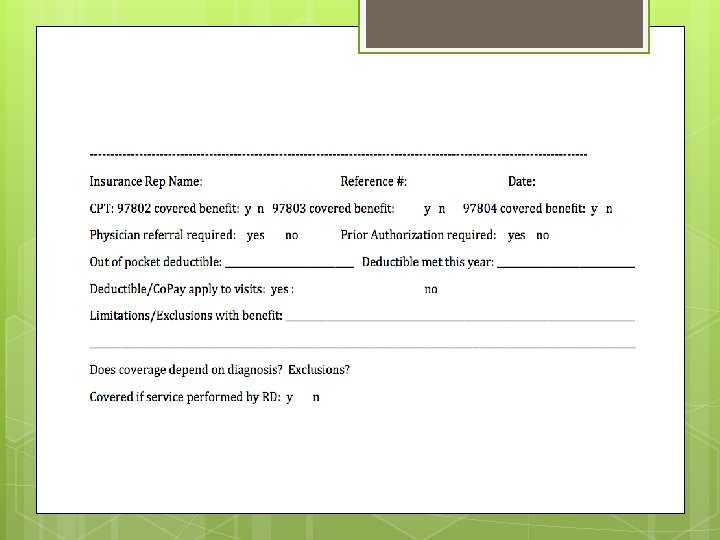
Insurance Reimbursement CAQH Pro. View (proview. caqh. org) & Credentialing NPI: Which https: //nppes. cms. hhs. gov/NPPES companies cover MNT? What are the CPT Codes? 97802, 97803, 97804 ICD-9/ICD-10 - October 1, 2015!!!! Verifying Benefits/Coverage Submitting Claims & Handling Denials
ICD-10 F 5000 AN, unspecified F 502 BN, unspecified F 509 Eating Disorder, unspecified E 509 Vitamin A Deficiency E 559 Vitamin D Deficiency 282 PCOS ER 635 Abnormal Weight Gain R 634 Abnormal Weight Loss E 669 Obesity, unspecified E 663 Overweight E 6601 Morbid (severe) obesity due to excess calories
ICD-10, cont. Z 6851 BMI, Pediatric less than 5%ile for age Z 6852 BMI, Pediatric, 5%ile-85%ile for age Z 6853 BMI, Pediatric, 85%ile- less than 95%ile for age Z 6854 BMI, Pediatric, Greater than or equal to 95%ile for age Z 681 BMI 19 or less, adult Z 6820 BMI 20 -20. 9, adult Z 6821 BMI 21 -21. 9, adult… Z 6839 BMI 39 -39. 9, adult Z 6841 BMI 40 -44. 9, adult Z 6842 BMI 45 -49. 9, adult Z 6843 BMI 50 -59. 9, adult Z 6844 BMI 60 -69. 9, adult
Academy ICD-10 Resource http: //www. eatrightpro. org/~/media/eatrightpro %20 files/practice/getting%20 paid/icd-10 -cmcodes-for-rdns. ashx
Referrals Are referrals needed? Establishing referral sources Example marketing packet Does this work? ?
Establishing Specialties Find your niche Refer to other RDNs! Collaborate with other professionals
Hours & Schedule Who do you treat? When are they available? Work/Life Balance Set Boundaries!
Marketing Business Cards Website Logo Design Promotional Materials Online Presence Media Presence
Accounting and Business Entity Types Sole Proprietor Partnership Corporation C Corp S Corp LLC
Business Policies/Forms Referral Form Intake Sheet Patient Demographics HIPAA Client Agreement/Policies Communication Session Forms/Packets Fax Coversheets Consent for Release of Healthcare Information
Medical Records EMR through a service/company Office Ally Practice Fusion EMR via your own set up Paper charts
Your Insurance Liability Insurance Malpractice Insurance Life/Health/Dental, etc.
Office Flow: Client Initiates Phone Call/Email Contact MD Insurance Verification Inform Client & Schedule Begin Treatment
Office Flow: Referral Receive Referral Contact Client Insurance Verification Inform & Schedule with Client Begin Treatment
Eating Disorder Treatment Basics
Role of the RDN Varies with level of care Varies from client to client Nutrition THERAPIST
ED Types: AN Anorexia Nervosa Restriction of energy intake, leading to significantly low body weight Intense fear of gaining weight Disturbance in the way body shape is evaluated or perceived
ED Types: BN Bulimia Nervosa Recurrent episodes of binge eating characterized by both: Eating in a discrete amt. of time (2 hr. ) large amounts of food Sense of lack of control over eating during a binge Recurrent compensatory behavior to prevent weight gain Binge and Purge both occur, on average, 1/wk. for 3 months Self evaluation unduly influenced by body shape/weigh Disturbance does not occur exclusively during episodes of AN
ED Types: BED Binge Eating Disorder Recurrent episodes of binge eating Binge eating associated with 3 or more of these: Eating more rapidly than normal Eating until uncomfortably full Eating large amounts of food when not hungry Eating alone because of feeling embarrassed by quantity Feeling disgusted with oneself, depressed, or guilty afterwards Distress regarding binge eating Occurs, on average, at least 1/wk. for 3 months Not associated with compensatory behavior or occur exclusively with AN or BN
ED Types: Otherwise Specified Feeding or Eating Disorder (OSFED/EDNOS) Disorder characterized by behaviors that don’t necessarily fall into another specific diagnosis Atypical AN: All criteria of AN met except despite weight loss, weight is within or above normal range BN low frequency: All criteria of BN met except bxs occur less than 1/wk. or less than 3 months BED low frequency: All criteria of BED met except bxs occur less than 1/wk. or less than 3 months Purging Disorder: Recurrent purging behavior in absence of binging behavior
Dieting & ED Statistics In US, 20 million women and 10 million men suffer from an ED in their lifetime 40 -60% of elementary school girls (ages 6 -12) are concerned about their weight or becoming too fat. For females between 15 and 24 yoa who suffer from AN, the mortality rate is 12 X higher than the death rate of all other causes of death There has been a rise in incidence of AN in women ages 15 -39 in each decade since 1930 Incidence of BN is 10 -39 yoa women TRIPLED between 1988 and 1993. In college aged men, rate of EDs is 4 -10%
Dieting & ED Statistics Girls who diet frequently are 12 times as likely to binge as girls who don’t diet 35 -57% of adolescent girls engage in crash dieting, fasting, SIV, diet pills or laxative use 95% of all dieters will regain their lost weight in 1 -5 years 35% of “normal dieters” progress to pathological dieting. Of those, 20 -25% progress to partial or full eating disorders.
Goals for MNT Establishing Ideal Weight Initial Meal Plan Cessation of ED behaviors Overcoming Fear Foods Make Peace with Numbers/Body Image Intuitive Eating
IBW Weight History Family Report BMI HAMWI Body Compositions Resolution of Menses, when applicable Natural Set Point
Meal Plan Formats Determining Calorie Needs Calorie Counts Exchanges Daily/Weekly Servings per meal Main and sides/Items
Meal Plan Increases: Wt. Gain Supplement v Food 250 -350 kcal/week Wt. Gain goal: outpatient ½-2#/week
Eating Disorder Behaviors Restriction Binging Purging: SIV Laxatives Diuretics Over Exercise Food Rituals Caffeine Abuse Chewing & Spitting Gum Chewing Self Harm Drugs/Alcohol Medication/Insulin Abuse
Fear Foods: You tell them to eat WHAT? ? Exposure Response Prevention Therapy Hierarchy of Fear Foods Systematically challenge fear foods 1: 1 Restaurant Challenge/Snack Challenge Independently
Volunteer for Activity
Make Peace with Numbers Coordinate with therapist Understand significance of specific numbers to the client Awareness of Weight
Intuitive/Normal Eating Tribole & Resch Ellyn Satter Eat the foods you truly want when you’re hungry, stop when you’re full. Allow yourself access to food the next time you’re hungry. Neutral emotion in response food.
First Session: Assessment Medical History ED History Behaviors: current/history Onset Triggering Event Function Treatment History Food likes/dislikes (fears? ) Motivation Assessment Family of origin Current core family Attitudes about food Weight relationship Food Recall Anthropometric Data Built Rapport
Follow Up Sessions Frequency Length of Time Average Length of Treatment
Useful Tools & Assignments Eat 26 Hierarchy of Fear Foods Food Rules Lists ED Pros/Cons Victory List/Challenge Calendar Thought Challenging Food Logs/Hunger & Emotion Tracking Hunger Scale Weight Life Story Normal Eating definition Exercise Prescription Behavior Analysis
Coordination of Care Doctor/NP/PA specializing in ED care Therapist/Counselor Psychiatrist RDN Coaches, Teachers, Support People Family
Barriers to MNT Readiness for change Underlying need still present Co-morbidities Difficult relationships
Tips for the Tough Ones Reflective Statements & Motivational Interviewing Agreeing on Common Goals Confronting. Directly. Repeatedly. What is the next small step? Assess a higher level of care
Client Resources Apps: Recovery Record Books: Life Without Ed, Intuitive Eating
Professional Resources Books: Intuitive Eating (Tribole & Resch), Guide to Private Practice (Academy), Counselling for Eating Disorders (Sara Gilbert), Eating Disorders: A Clinical Guide to Counseling and Treatment (Woolsey), How to Get your Child to Eat…but not too Much (Satter) Websites: nationaleatingdisorders. org (NEDA)
Thank you! Questions?