Priority 5 Plan Do Individual plan of care












 v. Breathlessness v. Nausea/vomiting")





 Dolopus 2 A Faces Rating")










 Tablet (Sevredol) Injection (Morphine Sulphate)")












 Haloperidol as an anti emetic (Also")


 Environment–room temp, ventilation, reassurance Consider whether")


- Slides: 49
Priority 5 - Plan & Do. Individual plan of care delivered with compassion Jacquie Upton Hospice at Home Lead
Planning Care v. Early opportunity to discuss, record and update patients wishes and preferences as apart of individualised care planning v. Extent of dying persons, their families/carers wishes for involvement v. Views, beliefs and values respected v. Remember a person is deemed to have capacity unless proven otherwise v. Individual plan of care “agreed, communicated, adhered to and regularly reviewed” by all involved
Assessment v. Undertake a holistic assessment for end of life needs and preferences in partnership with the patient, family/carers. v. Integrated approach with other health and social care professionals involved
Assess and respond sensitively to: v Physical needs v Emotional v Social v Psychological v Spiritual needs v Cultural and religious
Continual Assessment Assessing v. Assessment never stops! v. Subtle changes are significant and important v. Need to listen to family and carers they know their loved one v. Communicate, share, record and document changes and actions taken with clear rationale so all involved have an understanding v. Explanation to patient and family crucial
Food and Drink v There will come a point when a patient will not safely be able to eat or drink. v Informed choice - The patient may continue to try eating and drinking and risk aspiration, choking if they have capacity this needs to be respected v Family and friends understanding benefits and burdens around dehydration at the end stages of life v General Medical Council 2010 guidance – Treatment and care towards the end of life: good practice in decision making and relevant clinical guidelines.
Symptom Control Southern Health and Solent NHS have medicines administration orders for Syringe drivers and PRN medication These are supposed to be universal across the areas to minimise drug administration error A clear rationale needs to be assessed and recorded prior to administration Honouring of DNACPR by professionals Referring to SPCT as needed
Anticipatory medications at End of Life Anticipatory –foresee, act in advance of Generally -only drugs needed are: Analgesics for pain Anti-emetics for nausea & vomiting Anti-cholinergics for resp secretions or ‘death rattle’ Sedatives/anti-convulsants for agitation Explain to patient and family Important Conversations
Indications for a syringe driver: Patient unable to take oral medication and has been symptomatic Nausea and vomiting Unable to swallow Weakness Confusion Coma Poor alimentary absorption Medication more effective given by alt. route Bowel obstruction
IMPORTANT !!!!!! Medications need to be regularly reviewed and adjusted to give optimum effect and alleviate risk of toxicity.
A Symptom v Is a subjective and abnormal feeling or sensation which the patient experiences. v Is a feeling of something being 'not quite right' about one's body and is usually uncomfortable or, at least, unwanted. v May occur suddenly or be present for a while. v May occur intermittently or may become progressively worse. v A patient may experience several symptoms at the same time. v The symptom (including its severity) is something that only the patient can truly know
Underlying Symptoms v Several symptoms may be inter-related and by treating one you may well relieve others v A patient may be in such pain that he or she is unable to move around, and needs to take regular codeine for pain relief. v Constipation (if a laxative is not taken at the same time. ) v The patient’s pain allowing them to move around more freely, thus improving their bowel movements
Most commonly reported symptoms… v. Pain (often several types simultaneously) v. Breathlessness v. Nausea/vomiting v. Respiratory secretions v. Noisy breathing v. Pressure area damage v. Confusion v. Agitation/restlessness v. Elimination problems-Urinary incontinence/retention v. Dry/sore mouth v. Fatigue
Importance of accurate assessment Unrelieved pain causes unnecessary harm and suffering Pain diminishes activity, appetite, sleep and quality of life Pain further debilitates already weakened patients Full pain assessment/ using a pain tool validates the patients pain, helps patient to describe pain more accurately, increases the reporting Provides understanding of the personal experience of pain and the impact that pain Measuring severity of pain helps to understand the effectiveness of our intervention
How would you assess or recognise a persons pain?
Assessment of Pain Psychological: • Anger at delay in diagnosis • Anger at therapeutic failure • Disfigurement • Fears of pain • Fears of helplessness Source: Twycross & Wilcock (2001) Physical: • Other symptoms • Adverse effects of treatment • Insomnia and chronic fatigue TOTAL PAIN Social: • Worry about family • Job + prestige loss • Loss of social status • Family role loss • Isolation • Abandonment Spiritual: • Why has this happened to me? • Why has God allowed this? • What’s the point of it all? • Is there any meaning or purpose to this? • Can I be forgiven for past wrongdoing?
• Sore mouth • Earache • Difficulty in going to the toilet • Painful joints • Painful sores • Uncut fingers or toes • Being in same position for a Physical long time • Being moved uncomfortably Emotional • Loss of home • Loss of confidence • Loss of self esteem • Loss of loved ones • Anger and frustration Social • Where are my family • Where are my friends • Loss of independence • Loss of confidence • Loss of social networks • Loss of role or job Spiritual • How do I belong here? • Loss of abilities in relation to activities I love • Why me?
Pain Tools There a variety of pain assessment tools to choose from. Here a few v. Visual Analogue Scale: patient is asked to mark a point on the line to represent the intensity of the pain from none to worst pain v. Numerical Rating Scale: patient is asked to score the pain from 0 to 10 where 0 represents no pain and 10 represents worst pain v. Descriptive Words Scale: a patient is asked to use a list of adjectives to describe pain intensity ranging from none to worst
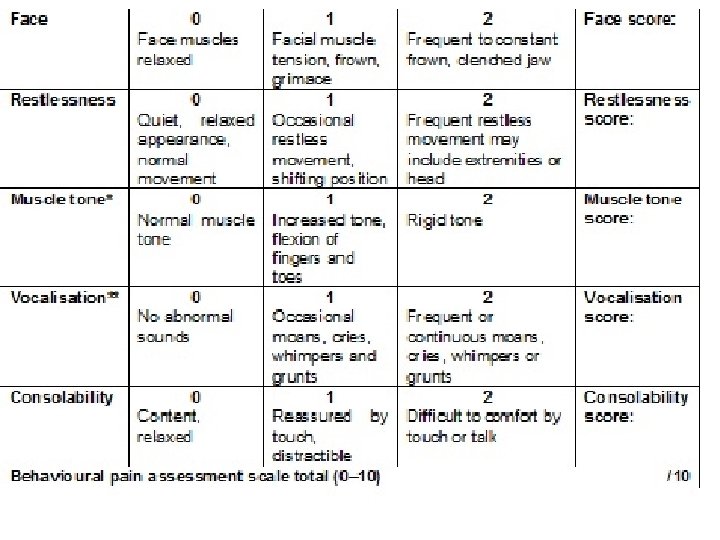
Pain Tools The Pain Assessment in Advanced Dementia (PAINAD) Dolopus 2 A Faces Rating Scale Abbey pain tool Disdat
PPQRST Pain Assessment Tool. Factors…. So ask… So consider… P Palliative What makes it better? What improves it? Heat pads, distraction etc. P Provokes What makes it worse? Movement, deep breathing. Q Quality R Radiation Does it spread? Where? Referred pain. S Severity How bad is it? How does it affect your life? T Timing Is there a Can we change pattern, time the an activity to pain comes on? help? What makes it worse What is it like? Be Sharp, stabbing, descriptive dull, ache.
Pain Assessment Tools
Pain assessment tools
Example
Summary of pain assessment v. Good pain management requires the patient to give a good history of their pain v. Try to optimise the patient’s own ability to report and describe pain v. Take collateral histories from carers if necessary
Things that lower the pain threshold v. Insomnia v. Fatigue v. Anxiety v. Fear v. Anger v. Boredom v. Sadness v. Depression v. Social isolation v. Social abandonment
Pain- Not all patients will experience pain, so be mindful of creating an expectation!
The WHO Analgesic Ladder
Starting Opioids – To gain control of the pain v. Usually start with immediate release morphine Every 4 hours, 2. 5 mg -10 mg, with the prn equal to the 4 hrly dose v. If using modified release morphine, give 10 mg 30 mgbd, depending on previous weak opioid,
General Principles of using Strong Opioids v. Start low and titrate up v. Regular dose of IR (immediate release) preparation and PRN (1/6 th of total) v. Prescribe a laxative – opioids nearly always cause constipation! v. Watch for nausea/vomiting (usually wears off after a few days)drowsiness, confusion/hallucinations
Strong Opioids Immediate Release Modified Release Morphine Liquid (Oramorph) Tablet (Sevredol) Injection (Morphine Sulphate) Usually capsules but some preparations are tablets Diamorphine Injection None available Oxycodone Liquid (Oxynorm) Capsule (Oxynorm) Injection (Oxynorm) Tablets (Oxycontin) Fentanyl Injection Lozenges (Actiq) Buccal and sublingual preps Patch – dose expressed in mcg/hr, changed every 72 hours Buprenorphine Sub lingual tablets Patch – dose expressed as mcg/hr, some patches changed every 72 hours, others every week Methadone Liquid, tablets, Injection. Due to different pharmacokinetic properties, as stored in fat cells, no immediate release preparation
Oral morphine to sc morphine v. Calculate daily dose of oral morphine v. Divide total oral dose by 2 Sub cut morphine is 2 x as strong as oral morphine v. This is the equivalent daily (24 hr) dose of morphine
Reasons for Switching Opioids v. Insufficient analgesia v. Cognitive impairment v. Sedation v. Nausea v. Constipation – fentanyl and buprenorphine are less constipating v. Renal impairment – morphine is excreted by the kidneys, so may accumulate in renal failure v. Pruritus v. Myoclonus
Myths about Morphine v. Respiratory depression valmost never a problem in cancer pain if used sensibly v. Addiction valmost never a problem in cancer pain v. Only for the terminal phase vdefinitely has a role for severe pain at any stage in the disease trajectory v. Hastens death v – NOT if used appropriately and sensibly
signs of toxicity v. Drowsiness v. Confusion v. Pin point pupils v. Myoclonic jerks v. Nausea/vomiting v. Hallucinations (auditory/visual) v. Respiratory depression
Other Approaches Complementary therapies v. Acupuncture v. Touch/massage v. Reflexology v. Aromatherapy v. Art therapy/music therapy Psychological support v. Reassurance v. Good communication v. Spiritual counselling
Case Scenario Think about a time when you have witnessed someone struggling with a symptom. What happened?
Agitation What symptoms or factors can cause agitation?
Agitation Look for reversible cause and treat if appropriate Pain Urinary retention Drugs Infection Constipation Haemorrhage Anxiety Terminal agitation
Management of Terminal Agitation Multi-professional approach if terminal agitation need to work together as a team to manage this affectively Assess the patient rule out what factors are exacerbating the agitation i. e. place a catheter in for retention Listen to patients and relatives is there an opportunity to discuss anger, fear or guilt issues. Can the chaplain or their own religious leader facilitate? Drug therapy assess which medication would be beneficial for their agitation. Rule out other symptoms such as pain or breathlessness first.
What medications help with terminal agitation/restlessness? Midazolam a short acting benzodiazepine which helps to reduce anxiety and aggression, relaxes muscles, suppresses seizures and sedates. Levomepromazine an antipsychotic which has a longer action for sedation in terminal agitation. It can act as an anti-emetic Haloperidol an antipsychotic for agitated delirium. Also acts as a anti-emetic
Non-Pharmaceutical Interventions Aromatherapy: there are certain essential oils which can aid grief and distress for both patient and family Soothing music: enquire from patient or relatives what kind of music they like Environment: is the room too hot or cold? Spiritual care: does the Chaplain or Vicar need to come in to perform a religious intervention or does a figure head from another religion need consulting? “Unfinished business” Reassurance: touch, voice, calmness, need to talk
Nausea & Vomiting - Key points on management Identify the cause of nausea and vomiting Treat the cause if possible and appropriate Target the antiemetic to the specific cause Use the oral route if mild nausea Use the subcutaneous route with severe nausea, or if vomiting
What medications help with Nausea & Vomiting (EOL) Haloperidol as an anti emetic (Also acts as a antipsychotic for agitated delirium) May cause jerking Review dosage after 24 hours. If two or more PRN doses given, then consider syringe driver Levomepromazine as an anti emetic (Also acts as a antipsychotic) May cause hypotension, drowsiness, dry mouth and other anticholinergic effects Cyclizine antihistamine with anticholinergic action (Avoid in heart failure) Can irritate the skin needs to be mixed with WATER and not Saline
Don’t forget… Mouth – coated tongue, candida etc Environment – sights, smells, bad tastes, tablet burden Anxiety - ? use of lorazepam esp. if anticipatory N&V Memory, fears
Breathing - Secretions ‘Death rattle’ Try repositioning patient Stop infusion or NG feed Anticholinergics can reduce volume of secretions if given in time Hyoscine Butylbromide 20 mg – 120 mg via syringe driver over 24 hrs, 20 mgs upwards PRN Hyoscine Hydrobromide (sedation effect) 400 mcg – 2. 4 mg via syringe driver over 24 hrs, 400 mcg sc prn Breathlessness 1. 0 -2. 5 mg of immediate release oral morphine 4 hourly prn & titrate upwards Explain to family – Be clear about what the “noise is”
Medications to consider with sensation of Breathlessness (EOL) Environment–room temp, ventilation, reassurance Consider whether patient is already taking oral morphine for breathlessness If the patient is not already taking morphine ensure prn morphine Sulphate 5 -10 mgs or diamorphine 2. 5 - 5 mgs prn is prescribed If patient is already taking morphine ensure appropriate prn dose sc morphine prescribed Convert to syringe driver with appropriate dose morphine/diamorphine Lorazepam 0. 5 -1 mg S/L(quick acting) for acute crisis and panic attacks
Summary : Symptoms at End of Life Potential symptoms are multiple Assess and ensure PRN meds available Identify and plan care Rule out reversible causes Include spiritual & social assessment Evaluate effect of any interventions Communicate plan with Next of Kin Always document and record rationale
Thank you