Principles of Neck Exploration and Aerodigestive Tract Injuries



















 l “Trapdoor” incision • Subclavian arteries l Collar")















 • May be passed")


















- Slides: 56
Principles of Neck Exploration and Aerodigestive Tract Injuries Niqui Kiffin, MD Operative Skills Conference 04 August 2009
Introduction Ø Only 5 -10% of traumas actually involve the neck l Ø Numerous vital structures are concentrated in a very small anatomic area l l Ø Penetrating most common Vascular Aerodigestive Vertebral Nerve Injury Generally, unprotected by bone or dense muscular covering
Contents Ø Anatomy l l “Zones” Platysma Initial Evaluation Ø Injury Management Ø Exposure Options Ø Aero-Digestive Injury Ø l l Trachea Esophagus
Anatomy Ø Borders l l Lower margin of the mandible Superior nuchal line of the occipital bone Suprasternal notch Upper border of the clavicle
Anatomy Ø Triangles l Anterior • Posterior belly of the digastric muscle • Anterior margin of the SCM • Sternohyoid muscle • Divide these structures with the inferior belly of the omohyoid muscle l l Carotid Triangle Muscular Triangle
Anatomy Ø Posterior l l Anterior border of the trapezius muscle Posterior border of the SCM Superior border of the clavicle Divide with the posterior belly of the omohyoid muscle • Occipital Triangle • Omoclavicular Triangle
Anatomy Ø Posterior Triangle Wounds l l Rarely involve the esophagus, airway or major vascular structure However, be aware that any penetrating wound that appears to enter in one triangle may traverse into another compartment of the neck and cause a lot of damage.
“Zones” of the Neck Ø Anterior Triangle Wounds l Zone I • • • “Base of the neck” Sternal notch Lower border of the cricoid cartilage • Highest mortality rate due to risk of major vascular and intrathoracic injury
“Zones” of the Neck l Zone II • Central/largest portion • Extends from the cricoid cartilage to the angle of the mandible • Most common • Lower mortality rate because injuries are usually apparent and exposure is easily accomplished
“Zones” of the Neck Ø Zone III l l l Above the angle of the mandible High risk of injury to the distal carotid artery, pharynx, and salivary glands Exposure can be exceedingly difficult
“Zones’ of the Neck Ø Zone I l Ø Zone II l Ø Thoracic outlet vasculature, vertebral and proximal carotid arteries, lung, trachea, esophagus, spinal cord, thoracic duct, and major cervical nerve trunks Jugular veins, vertebral and common carotid arteries, and external and internal carotid arteries Zone III l Pharynx, jugular veins, vertebral arteries and the distal internal carotid arteries
Platysma Ø Platysma l l Thin, broad muscle that lies just beneath the skin and covers the entire anterior triangle and the anteroinferior aspect of the posterior triangle. Wounds that do not penetrate the platysma are considered superficial and do not require additional work-up
Initial Evaluation Ø Secure an adequate airway l Preferably translaryngeal ETT • May require fiberoptic bronchoscopy l l l Cricothyroidotomy Emergent tracheostomy via neck wound Chest tubes as necessary • PTX, hemothorax Ø Circulatory Assessment/Stabilization l Significant hemorrhage • Direct pressure • Immediate transfer to the operating room • No role for blind clamping or tourniquets in penetrating neck trauma
Initial Evaluation Ø History/Physical l If patient is hemodynamically stable and able to participate
Injury Management Ø Depends on the status of the patient, the “zone” of injury, and the presence/absence of “hard” or “soft findings” of vascular or aero-digestive injury. Ø In the past, all Zone II injuries were surgically explored, however now with access to endoscopy, fluoroscopy, CT and angiography; it is not always necessary.
“Soft Findings” Ø Dysphagia Ø Voice Change Ø Hemoptysis Ø Hematemesis Ø Widened Mediastinum
“Hard Findings” Ø Airway compromise Ø Shock/active bleeding Ø Pulsatile hematomas Ø Extensive subcutaneous emphysema
Management Ø If “hard findings” present: l Immediate operative exploration Ø If “soft findings” present: l l CT/CT Angio Bronchoscopy Esophageal Swallow +/- Endoscopy If these studies positive for injury, pt deserves an operative exploration
Exposure Options Ø Zone I l Supraclavicular incision • Distal subclavian artery l Left Thoracotomy • Proximal left subclavian artery • Distal Esophagus l Right Thoracotomy • Distal Trachea l Median Sternotomy • Innominate artery/proximal right subclavian artery l Removal of the head of the clavicle • Subclavian arteries
Exposure Options Ø Zone I (con’t) l “Trapdoor” incision • Subclavian arteries l Collar incision • Esophagus • Proximal Trachea l Midline • Trachea l Sternocleidomastoid • Esophagus • Carotid • Jugular Veins
Exposure Options Ø Zone III l l l Sternocleidomastoid Incision +/- extension May require disarticulation or partial mandibular resection Limited craniotomy
Exposure Options Ø Zone II l l Sternocleidomastoid Incision Collar Incision • Provides access to both sides of the neck
Aero-Digestive Injuries Ø 10% of penetrating neck injuries l Esophagus • < 1% of all traumatic injuries • <0. 1% are secondary to blunt trauma • >80% l l l Secondary to penetrating neck trauma However, 0. 5 -7% of penetrating neck injuries are associated with esophageal involvement Trachea • 3 -8% - injure cervical trachea • Only 4% of all injuries related to the cervical trachea are from blunt trauma l Both • May be as much as 28%
Pathophysiology Ø Penetrating l l Knife – cervical trachea GSW – cervical or intrathoracic • Intrathoracic – higher incidence when projectile crosses the mediastinum. Associated with injuries to great vessels, heart, and esophagus
Pathophysiology Ø Penetrating l l Stab Wounds Gunshot Wounds • Shotgun Wounds
Pathophysiology Ø Blunt l Direct Blows • • l “clothesline”-type injury Crushes the cervical trachea against the vertebrae May be called a “dashboard” injury May also occur secondary to a high-riding shoulder harness Rapid Hyperextension • Produces a traction and distraction injury • Most commonly results in laryngotracheal separation l Shear Stress • Creates damage at fixed points (cricoid and carina) l Burst Injury • • Rapid AP compression of the thorax Simultaneous expansion in the lateral thoracic diameter Closure of the glottis (increased intratracheal pressure) Results in linear tears within the membranous portion
Pathophysiology Ø Iatrogenic l Tracheostomy/Intubation • • Improper stilette use Erroneous choice of tube size Over-inflation of balloon Ill-positioned tracheostomy tube
Presentation SQ emphysema Ø PTX Ø l l Persistent Continuous air leak Pneumomediastinum Ø Hemoptysis Ø Dyspnea Ø Dysphonia Ø Difficulty with mechanical ventilation Ø
Presentation Ø Fallen Lung of Kumpe l Lung falling away from the hilum (laterally and posteriorly), in contrast to simple PTX which collapses towards the hilum Abnormal migration of ETT Ø Overdistention of the ETT outside the confines of the normal tracheal diameter Ø
Management
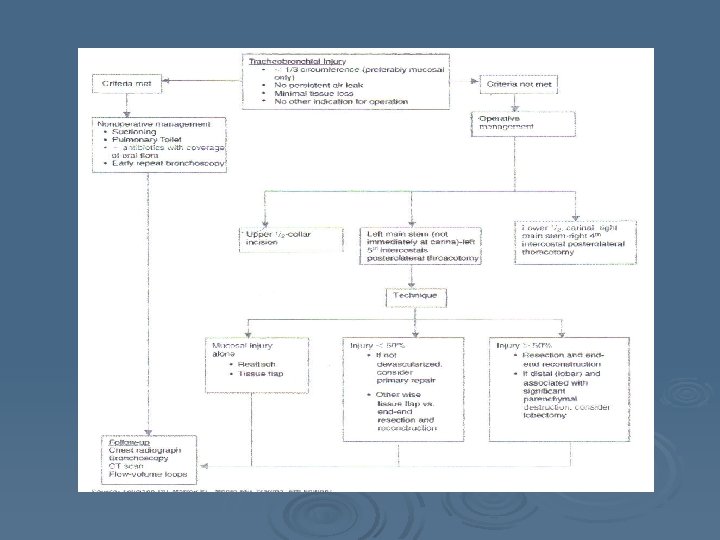
Nonoperative Management Ø When? l l l Small TBI < 1/3 circumference Well-opposed edges No tissue loss No associated injuries No need for PPV Ø Controversial……
Nonoperative Management Ø Ø Ø Retrospective Study 33 TBI 60% conservative/40% operative 5 deaths (none attributed to treatment choice) Selection Criteria l l Absence of major symptoms, no progressive SQ or mediastinal emphysema, no severe dyspnea requiring intubation, no difficulty with mechanical ventilation, no PTX with persistent air leak, no open tracheal injuries or mediastinitis Independent of injury length, location, diagnostic delay or pathogenesis J of Trauma, Vol 61 (6), 2006
Nonoperative Management Ø What? l l l l Humidified air Voice rest Frequent suctioning Prophylactic abx PPI Close observation Bronchoscopy follow-up Intubation distal to lesion • If already intubated…
Operative Management Ø Airway Management l Single lumen ETT (long) • May be passed distal to injury l Proximal Injuries • May be passed into contralateral bronchus l l Distal Injuries Double lumen ETT • Allow for one lung ventilation • Larger size l l Cardiopulmonary Bypass High Frequency Jet Ventilation • Low airway pressures l ECMO
Operative Management Ø Exposure l Cervical Injuries • Transverse Collar Incision l May be extended up or down into median sternotomy if necessary • SCM Incision l Intrathoracic Injuries • Right posterolateral thoracotomy (avoids heart and aorta) l l l Intrathoracic trachea Right mainstem bronchus Proximal left mainstem bronchus • Left posterolateral thoracotomy l Distal left mainstem bronchus (>3 cm from carina)
Operative Management Ø Prophylactic Abx Ø Debridement Ø Repair l Primary • Interrupted • Absorbable Sutures l Some studies have shown effective repair with nonabsorbable sutures as well • Knots external to trachea
Operative Management l Resection • 4 -5 cm of trachea can be mobilized to obtain length after resection l Additional length can be obtained by cervical flexion • Dissection should be carried out anteriorly and posteriorly to avoid lateral pedicles (devascularize the trachea) • End to end anastomosis l l l Interrupted sutures Assure mucosa to mucosa approximation Suture line should be buttressed with pleural flap, intercostal muscle flap, or pericardial flap
Operative Management Ø Intercostal Muscle Flap l l If considered, should be preserved on entrance into the thoracic cavity An incision is made directly over the rib and the periosteum stripped off Incision is carried on through the posterior layer of the periosteum to enter the pleural space The muscle is then divided from the ribs above and below while sparing the blood supply and used as a flap to buttress your repair
Operative Management Ø Cervical Injuries l Tracheostomy +/ • Avoid placing your tracheostomy through the injury • End tracheostomy is performed only for extensive devitalization and contamination l Repair +/ • Simple anterior injuries may require repair only
Outcomes Ø Suture Granulomas l Ø Can usually be alleviated with laser or bronchoscopic intervention Stenosis l l l May present later with “asthma” Can be improved with serial dilatation and stents (rubber and metal) May require additional resection • 3 -6 months after initial repair Ø Occlusion l Ø May require additional resection, possible pulmonary resection Fistulas l l Tracheal/Innominate artery Tracheoesophageal
Post-Operative Management Ø Extubate immediately if possible l l If pt remains intubated, keep endotracheal balloon distal to suture line or proximal if injury is near the carina. Keep airway pressures low. Ø Aggressive pulmonary toilet Ø Repeated bronchoscopy as needed to evaluate repair
Highlights Ø Initial priority is airway stabilization l Ø Ø Ø May require fiberoptic bronchoscopy Penetrating injury predominantly affects the cervical trachea Blunt injury affects the distal trachea and carina Suspect the diagnosis in any patient with a significant air leak, SQ emphysema, and/or PTX despite chest tube placement Collar incision – upper half of the trachea Right 4 th ICS posterolateral thoracotomy – distal trachea Operative repair involves debridement of devitalized tissue, but in most cases simple reconstruction with absorbable interrupted sutures will suffice.
Pharynx and Esophagus Ø Esophageal injuries l l l 5% of patients with penetrating neck wounds Blunt - < 10% of all esophageal perforations If suspected, it must be ruled out… • • l l Direct visualization (OR) Esophagraphy – sensitivity 50 -90% Endoscopy – sensitivity 29 -100% Combined – accuracy of almost 100% It must be suspected in any patient with a penetrating neck wound, a hyperextended neck or a blast injury If diagnosis delayed, mortality increases exponentially…. based on length of time from diagnosis to treatment.
Clinical Presentation Ø Ø Ø Ø May be suggested by mechanism of injury Dx can be suggested or obscured by the presence of associated injuries Hoarseness Hemoptysis Subcutaneous air Anterior tracheal deviation Extra-esophageal NGT Late Presentation l l l Fever Erythema Abscess Mediastinitis Sepsis
Diagnosis Ø Gastrograffin Swallow l If negative, should be followed by barium • Confirms leak • Gives location (right or left) • False negative 10% Ø Esophagoscopy l Ø CT Scan l Ø Can miss 15 -40% of injuries May show track of penetrating trauma, contrast/air around the mediastinum, pleural effusions, or as a follow-up Esophagram + Esophagoscopy l Sensitivity - Nearly 100%
Operative Repair Ø Collar Incision l Particularly useful if bilateral injuries present Ø Sternocleidomastoid Incision l “Carotid” incision Ø Right posterolateral thoracotomy l Upper 2/3 of the thoracic esophagus Ø Left posterolateral thoracotomy l Distal thoracic esophagus
Management Ø Ø Control leak Adequate drainage Esophageal debridement Primary repair l l l Ø Buttress repair l l Ø Ø Single vs. double layer closure Absorbable suture internally, may use nonabsorbable for external layer Interrupted vs. running repair SCM Intercostal muscle Pleural flap Pericardial flap Nutritional Support Early use of Abx
Operative Management Ø If in doubt…. . operate on the side of the wound or the leak. Ø Most injuries can be repaired primarily, l If not possible, (large defects, extensive tissue damage, or delayed diagnosis) may consider: • • • Tissue flaps, T-tube drainage, End-to-end anastomosis, or Diversion with cervical esophagostomy Esophagectomy
Complications Ø Leaks after repair may heal spontaneously if drained adequately and antibiotic support provided. l l l Thoracic leaks may require radiographically placed drains Consider stents for mid-esophageal leaks Unstable or septic patients require re-operation Post-operative stenosis can usually be managed with repeated endoscopic dilatation Ø Fistula Ø l Tracheoesophageal • • New onset cough or pneumonia Repeated aspiration Usually avoided if repair is buttressed adequately Requires operative repair
Highlights Ø Signs and symptoms are nonspecific l Must have a high degree of suspicion Ø Most injuries require a simple repair Ø All repairs should be buttressed by local tissue Ø Outcome is critically affected by delay in diagnosis
References… Ø Trauma David V. Feliciano, Kenneth L. Mattox, Ernest E. Moore CH 23 Management of Acute Neck Injuries CH 27 Esophagus, Trachea and Bronchus Ø ACS Surgery: Principles and Practice CH 7 Trauma and Thermal Injury Sect 4 Injuries to the Neck