Principles of management Pediatric Fractures Objectives Statistics about

Principles of management Pediatric Fractures

Objectives • • Statistics about fractures in children How children’s bones are different Outline principles of management Point out specific precautions Acknowledgement and recommendation Lynn T Staheli

introduction • In Middle East ~60% of population are < 20 yrs. • Fractures account for ~15% of all injuries in children. • Different from adult fractures • Vary in various age groups ( Infants, children, adolescents )

Statistics • ~ 50% of boys and 25% of girls, expected to have a fracture during childhood. • Boys > girls • Rate increases with age. Mizulta, 1987

Statistics • ~ 50% of boys and 25% of girls, expected to have a fracture during childhood. • Boys > girls • Rate increases with age. • Physeal injuries with age. Mizulta, 1987
")
Statistics Most frequent sites (sample of 923 children, Mizulta, 1987)

Why are children’s fractures different? Children have different physiology and anatomy • • Growth plate. Bone. Cartilage. Periosteum. Ligaments. Age-related physiology

Why are children’s fractures different? Children have different physiology and anatomy • Growth plate: – In infants, GP is stronger than bone increased diaphyseal fractures – Provides perfect remodeling power. – Injury of growth plate causes deformity. – A fracture might lead to overgrowth.

Why are children’s fractures different? Children have different physiology and anatomy • Bone: – Increased collagen: bone ratio - lowers modulus of elasticity

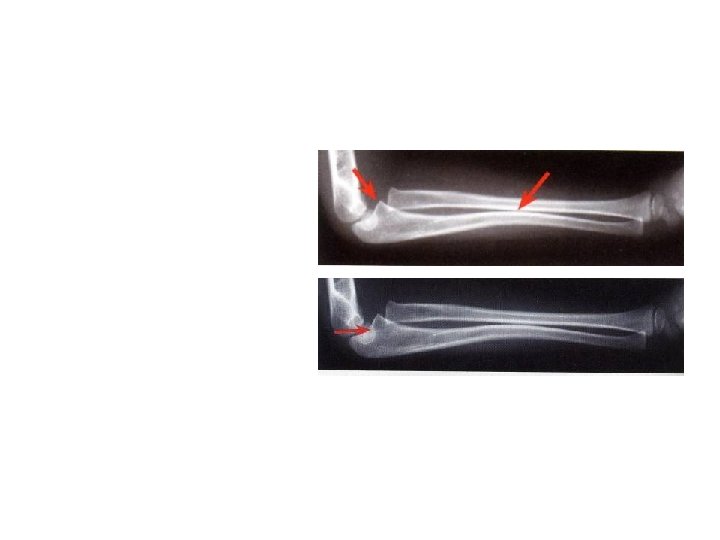
Why are children’s fractures different? Children have different physiology and anatomy • Bone: – Increased collagen: bone ratio - lowers modulus of elasticity – Increased cancellous bone - reduces tensile strength - reduces tendency of fracture to propagate less comminuted fractures – Bone fails on both tension and compression - commonly seen “buckle” fracture

Why are children’s fractures different? Children have different physiology and anatomy • Cartilage: – Increased ratio of cartilage to bone - better resilience - difficult x-ray evaluation - size of articular fragment often under-estimated

Why are children’s fractures different? Children have different physiology and anatomy • Periosteum: – Metabolically active • more callus, rapid union, increased remodeling – Thickness and strength • Intact periosteal hinge affects fracture pattern • May aid reduction

Why are children’s fractures different? Children have different physiology and anatomy • Age related fracture pattern: – Infants: diaphyseal fractures – Children: metaphyseal fractures – Adolescents: epiphyseal injuries

Why are children’s fractures different? Children have different physiology and anatomy • Physiology – Better blood supply rare incidence of delayed and non-union

Physeal injuries • • • Account for ~25% of all children’s fractures. More in boys. More in upper limb. Most heal well rapidly with good remodeling. Growth may be affected.

Physeal injuries Classification: Salter-Harris, Peterson, Ogden

Physeal injuries • Less than 1% cause physeal bridging affecting growth. – Small bridges (<10%) may lyse spontaneously. – Central bridges more likely to lyse. – Peripheral bridges more likely to cause deformity – Avoid injury to physis during fixation. – Monitor growth over a long period. – Image suspected physeal bar (CT, MRI)

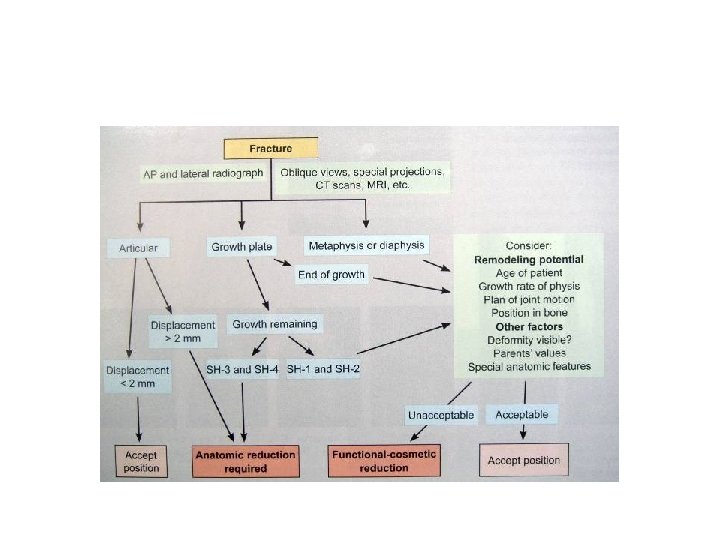
The power of remodeling • Tremendous power of remodeling • Can accept more angulation and displacement • Rotational mal-alignment ? does not remodel

The power of remodeling Factors affecting remodeling potential • Years of remaining growth – most important factor • Position in the bone – the nearer to physis the better • Plane of motion – greatest in sagittal, the frontal, and least for transverse plane • Physeal status – if damaged, less potential for correction • Growth potential of adjacent physis e. g. upper humerus better than lower humerus

The power of remodeling Factors affecting remodeling potential • Growth potential of adjacent physis e. g. upper humerus better than lower humerus

Indications for operative fixation • Open fractures • Displaced intra articular fractures ( Salter-Harris III-IV ) • fractures with vascular injury • ? Compartment syndrome • Fractures not reduced by closed reduction ( soft tissue interposition, button-holing of periosteum ) • If reduction could be only maintained in an abnormal position

Indications for operative fixation

Methods of fixation • Casting - still the commonest

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • K- wires could be replaced by absorbable rods

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • K- wires could be replaced by absorbable rods Preoperative immediate 6 months 12 months Hope et al , JBJS 73 B(6) , 1991

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails – Very useful – Diaphyseal fractures

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails – Very useful – Diaphyseal fractures • Screws

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails – Very useful – Diaphyseal fractures • Screws

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails – Very useful – Diaphyseal fractures • Screws • Plates – multiple trauma

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails – Very useful – Diaphyseal fractures • Screws • Plates – multiple trauma • IMN - adolescents only (injury to growth)

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails • • – Very useful – Diaphyseal fractures Screws Plates – multiple trauma IMN - adolescents Ex-fix – usually in open fractures

Methods of fixation • Casting - still the commonest • K-wires – most commonly used – Metaphyseal fractures • Intramedullary wires, elastic nails • • – Very useful – Diaphyseal fractures Screws Plates – multiple trauma n o IMN - adolescents i t a n Ex-fix i b m o C

Fixation and stability • Fixation methods provide varying degrees of stability. • Ideal fixation should provide adequate stability and allow normal flexibility. • Often combination methods are best.
 •")
Complications • Ma-lunion is not usually a problem ( except cubitus varus ) • Non-union is hardly seen ( except in the lateral condyle ) • Growth disturbance – epiphyseal damage • Vascular – volkmann’s ischemia • Infection - rare

Beware! Non-accidental injuries

Beware! Non-accidental injuries • • ? Multiple At various levels of healing Unclear history – mismatching with injury Circumstantial evidence

Beware! Non-accidental injuries • Circumstantial evidence • • Soft tissue injuries - bruising, burns Intraabdominal injuries Intracranial injuries Delay in seeking treatment

Beware! Non-accidental injuries • Specific pattern – Posterior ribs – Skull
")
Beware! Non-accidental injuries • Specific pattern – Corner fractures (traction & rotation)
")
Beware! Non-accidental injuries • Specific pattern – Bucket handle fractures (traction & rotation)

Beware! Non-accidental injuries • Specific pattern – Femur shaft fracture • <1 year of age ( 60 -70% non accidental) • Transverse fracture – Humeral shaft fracture <3 years of age – Sternal fractures

Beware! Malignant tumours • • Can present as injury. History of trauma usual. • 12 y old girl • History of trauma • mild tenderness • Periosteal reaction • 2 m later, still tender • Ewings sarcoma

Special considerations During resuscitation

summary Children’s bones are different

summary • • About 60% of population in ME are children! Fractures in children are common. Children’s bones are different Outline principles of management. Specific treatment plans (combinations possible) Specific precautions. Beware – Non-accidental trauma – Malignant tumors

- Slides: 49