Principles in Biomedical and Islamic Medical Ethics Shahid

Principles in Biomedical and Islamic Medical Ethics Shahid Athar, MD, FACP Past Chair, Medical Ethics Islamic Medical Association of North America www. IMANA. org Presented at IMANA/ Hofstra University Sept. 18 , 2010

The Disclaimer 1. I am on speaker’s bureau of several pharmaceutical companies, however, this CME presentation is not financially supported by any of them. 2. I am not a mufti (Islamic scholar qualified to give fatwa or religious decree).


“Blessed is He, in Whose Hands is the Sovereignty , and He is able to all things. Who has created death and life that He may test you , which of you is best in conduct and He is the Mighty and the Forgiving. ” Qura n 67: 1 -2

Presentation Objectives • • • Principles of Biomedical Ethics Principles of Islamic Medical Ethics IMANA’s position on End of Life issues An interfaith perspective on EOL issues Case presentations and discussions

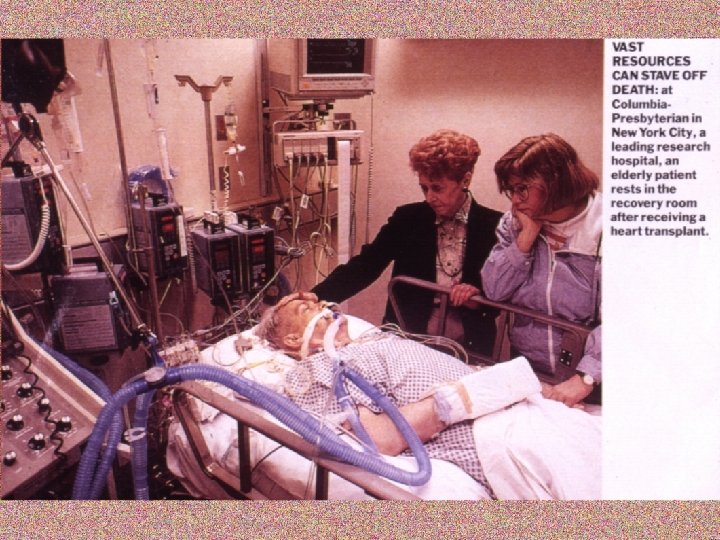
End of Life Concerns …. . • When can we stop medical care? • Life support of patients on dialysis, chemotherapy and ventilators? • Withholding of tube feeding and TPN? • Organ donation and transplantation? • Palliative care (pain medications, sedation) in terminally ill patients? • Need for Living Will and Advance Directive

What is Medical Ethics? “Medical Ethics is a decision making process , not all black or all white, or all right or all wrong, but in gray areas, choosing a better option over a worse one. The difference between what can be done and what should be done is the reason for Medical Ethics”

Questions in Ethics • Ethics vs. Morality – are both same? • Religious vs Secular Ethics • If the patient is unable to speak for himself - then who guards his interest? (family, MD, State) • When the family and caregiver’s views clash –whose views be taken? • When caregiver and the patient have different faith/ values- how do they reconcile?

The Principles of Medical Ethics • • Preserve life Promote and restore health Alleviate suffering Respect patient’s autonomy Distributive justice Tell the truth Do no harm

Some Ethical Terms Explained… • Respect for autonomy: “ people are autonomous in decision making for themselves if they are able to understand the options and do it voluntarily. This principle requires informed consent”

Beneficence • This principle obliges persons to benefit or help others. It requires positive action: to prevent what is bad or harmful; to remove what is bad or harmful; and to do or promote what is good or beneficial.

Nonmaleficence • This principle obliges persons to refrain from harming others, including to refrain from cruelty and torture. • This is a principle of non-intervention. It requires persons to exercise due care that they do not unintentionally harm others through their actions such reckless interventions or procedures.

Distributive Justice • This principle requires a fair distribution of benefits and burdens. It requires that persons receive that which they deserve. This principle is involved in decisions to allocate scarce health resources such as use of ICU beds and ventilators in case of a pandemic.
 Terms. . • Darura (necessity): over rides prohibition • Fitra :")
Some Arabic (Islamic) Terms. . • Darura (necessity): over rides prohibition • Fitra : (the built in good human nature) • Istihsan : (juristic preference between two or more valid judgments. • Maslaha (public good) • Marsalih al mursala (public good derived from reasoning) • Sunnah (traditions of Prophet Mohammad)
 “ Moaz ibn Jabal (r) was asked by Prophet")
The Place of Ijtehad (reasoning) “ Moaz ibn Jabal (r) was asked by Prophet Muhammad (p) before sending him to Yemen , “on what basis he will judge cases ? ”, he replied “Quran”. The Prophet asked ”and if you cannot find the answer in Quran, then ? ”, Moaz said “ the sunnah of the messenger of Allah”. The Prophet asked" and if you cannot find the answer there either”, Moaz said , “Then I will make every attempt with my own opinion to make a right decision”. The Prophet (p) was delighted and said “ Praise be to Allah who has guided the envoy of the messenger of Allah”
: • Preservation and protection of life • Preservation and")
Goals of Shariah (Islamic Laws): • Preservation and protection of life • Preservation and protection of mind • Preservation and protection of private ownership • Protection of the freedom of religion • Protection and preservation of progeny

Rules of Islamic Medical Ethics • Necessity overrides the prohibition • Accept the lessor of the two harms if both cannot be avoided • Public interest overrides individual interest • Harm has to be removed

The rule of “No harm, no harassment” (la dararar was la dirar fi al- Islam) • Actions are judged on intentions- hadith • Hardship necessitates relief • One needs certainty: how was the present doubtful situation resolved in the past? • Harm has to be removed/ take lesser of two evils • Local customs determine the course of action

End of Life issues An Interfaith Perspective “Most Religions believe in life and health as gifts from God and uphold the sanctity of human life as well as dignity for the dying person” (Lancet Sept. 2005)

Diversity is the recognition and respect for the values of the Other “Our first task in approaching another people, another culture and another religion is to take off our shoes first for the place we are approaching is holy, else we may find ourselves treading on another’s dream. More seriously still, we may forget that God was there before we arrived”

End of life-the Buddhist view • Death is an integral part of life by virtue of belief in incarnation • Death is an experience that everyone will go through many times. • Brain death is not accepted by all Buddhists especially Japanese • Nutrition and hydration should continue in persistent vegetative state • Euthanasia is rejected by most Buddhists • Withdrawal of intervention when end is near is not immoral

End of life-a Hindu view • Life is a transition between previous one and next one • Karma explains inequity and suffering in this life and affects next life. • A good death is on right time , in right place , prepared and mind on God • The family has a sacred duty to help the dying before and after death. • Suicide is frowned upon but voluntary euthanasia for spiritually advanced is accepted • Involuntary euthanasia is justified to prevent extreme suffering

End of life- a Jewish perspective • The body belongs to God • Humans have both permission and obligation to heal. • Humans have no right to commit suicide or enlist the aid of others in the act. • A patient has a right to pray to God for death to end his/her suffering • Criteria for death is cessation of breathing and heart beat. • Heroic measures are allowed if there is hope for cure , comfort care must continue • Visiting the sick is an obligation.

End of life –a Catholic view • Life is a sacred gift from God and has an intrinsic worth • Understanding of sickness and death is grounded in belief that Jesus suffered, died and was resurrected • Human dignity and interdependence are of supreme value • The value of stewardship and creativity holds us accountable to God • The value of charity demands us to respond to others in need especially the poor.

End of life issues-a traditional Christian view • The pursuit of eternal life through repentance and pursuit of holiness through humble submission to God • Values within traditional Christians are diverse • Intending and causing death is not allowed • Salvation through Jesus is a core belief

End of life- a secular view • Atheists regard God as a human creation • Care is directed towards need of the individual • Ignoring need is a form of discrimination • This life is all there is and death is the end of life • Keep religion out of health care and hospital environment
 • A")
Case 1: DNR and family conflict (JAMA 2009 ; 11: 582 -588) • A 63 year old visitor from Lebanon here for an elective surgery had MI and coded. He is on MV now. The neurologist does not think he will recover. His son signs a DNR but his elder brother back home does not agree and wants full code. Patient’s wife back home is not informed of what is her husband’s condition. • What should his (non Muslim) physician do?

Case : 2 • 70 year old lady had surgery for a ruptured appendix 2 years ago • Diagnosed 1 month earlier with poorly differentiated adenocarcinoma of the right lung with significant bilateral paratracheal adenopathy • She elected no chemo or radiation therapy

Case 2 continued. • Properly executed a DNR form stating no tubes in throat and no Mechanical Ventilation • Copy placed on chart • Presented with fever, tachycardia, abdominal pain, significant abdominal distension • Mechanical intestinal obstruction • Surgeon recommended immediate laporotomy

Case 2 continued • Anesthesiologist: patient would require GA, intubation and likely MV; possible treatment of arrhythmia and hypotension – i. e. resuscitative measures • Surgeon: problem is temporary and can be corrected • How should we respond to the conflict between anesthesiologist and surgeon? • How should we address patient’s autonomy?

Case # 3 - Who can consent? DM , a 25 year old , pregnant immigrant woman , is brought to ER in acute abdominal pain. She is examined in the presence of her husband a tubal pregnancy is diagnosed. Although , she can speak English , her husband answers all the questions and when it comes to taking consent before the treatment (operation vs medical) , he insists he should give the consent saying “ I speak for her ”

Q. After a massive brain hemorrhage, my mother is in a coma and is on artificial life support. Her physician says there is no hope of survival and wants to pull the plug. We love her very much. What should we do?

Question from a physician. “ As a physician, when I find out that my patient has a terminal illness and will die very soon. should I tell the truth to my patient and his family as soon as I know myself? ”. My patient is from Middle East where they do not tell diagnosis to an elderly dying person

Q, My grandfather never took care of his diabetes. Now he has developed gangrene in his foot. Doctors recommend amputation to save the rest of his leg. He refuses. What should we do?

For the wind that blows the sail is the mind But the faith in the heart is the compass to guide And what is the eyesight if heart is blind? Lo! We all look so good. But what is inside? Who is right? Who is wrong? Only God will decide Late Dr. Hassan Hathout, the Islamic ethicist

“To Allah belongs the East & the West”

Selected References 3. Hassan Hathout , “Reading The Muslim Mind” 4. Abdulaziz Sachedina: Islamic Biomedical Ethics 5. Shahid Athar, “Islamic Perspectives in Medicine” 6. Shahid Athar, “Health Concerns for Believers” 7. Islamic Code Of Medical Ethics (IOMS-Kuwait) 8. 2002 year book on Ethics published by FIMA.

Websites for Islamic Medicine • • • www. imana. org www. IIIM. org www. islamset. com (IOMS website) www. islamonline. net www. islamicmedicine. org www. islam-usa. com (sathar 3624@aol. com)

The Disclaimer I am on speaker’s bureau of several pharmaceutical companies, however, this CME presentation is not financially supported by any of them
")
Shalom (Salaam, Peace)
- Slides: 42