Primary Hyperparathyroidism in Iran and Other Developing Countries


 is characterized by: a) unregulated parathyroid hormone (PTH) secretion and")
 on the kidney and bone.")












 There were 7 published papers, Three in English (in international journals) and,")
 Six papers contained comprehensive informations regarding demographic, clinical, laboratory, radiological, and pathological")








 The vast majority of patients from developing countries present with severe bone disease.")
 Renal disease is considerably less frequent in patients with PHPT from developing counties.")
 Normocalcemic PHPT with bone and/or stone disease is an exception rather than the")









































- Slides: 74
Primary Hyperparathyroidism in Iran and Other Developing Countries Amir Bahrami MD Tabriz University of Medical Sciences
Primary Hyperparathyroidism (PHPT) is characterized by: a) unregulated parathyroid hormone (PTH) secretion and b) resulting hypercalcemia. Excess PTH leads to the potential for major complications at the level of target tissues mainly bones and kidneys.
Actions of parathyroid hormone (PTH) on the kidney and bone.
Albright and Reifenstein originally described primary hyperparathyroidism as a disease of "bones and stones". Osteitis fibrosa cystica reported to be the hallmark of hyperparathyroid bone disease.
kidney disease manifested by nephrolithiasis or rarely nephrocalcinosis was present in more than three fourth of patients at the time of diagnosis. Albright F, et al. JAMA 102: 1276 – 1287, 1934. Albright F, et al. Baltimore, Williams and Wilkins, 1948. Cope O. N Engl J Med 21: 1174 – 1182, 1966. Mallette LE, et al. Medicine (Baltimore) 53: 127 – 147, 1974.
In the West, the disease today bears little resemblance to the originally described severe disease of bones and stones. § Indeed PHPT has evolved over the last four decades from a severe disease to: § an asymptomatic condition or § a disorder with more subtle manifestations Heath H, et al. N Engl J Med 1980; 302: 189 – 193. Heath H III. J Bone Min Res 1991; 6: Supplement 2: S 63 – S 70. Mundy GR, et al. Lancet. 1980; 1: 1317 – 1320. Scholz DA, et al. Mayo Clin Proc 1981; 56: 473 Silverberg SJ. , et al. In: LJ. De. Groot and JL. Jameson, editors. Endocrinology: 4 th edition W. B. Saunders Company 1075 – 1093 2001.
the incidence of renal disease has been reduced from almost 50% - 70% common in the past to nearly 10% of patients currently. Silverberg SJ. , et al. In: LJ. De. Groot and JL. Jameson, editors. Endocrinology: 4 th edition W. B. Saunders Company 1075 – 1093 2001. Silverberg SJ, et al. Am J Med 89: 327 – 334, 1990.
Osteitis fibrosa cystica, the classic presentation of skeletal involvement in PHPT has been declined sharply in its relative frequency Heath H, et al. N Engl J Med 1980; 302: 189 – 193. Heath H III. J Bone Min Res 1991; 6: Supplement 2: S 63 – S 70. Mundy GR, et al. Lancet. 1980; 1: 1317 – 1320. Silverberg S. J. , et al. J Bone Mineral Res, 1989; 4: 282 – 291.
In essence, in the West, symptomatic disease is today the exception rather than the rule with nearly more than 80% of cases having no symptoms. Silverberg SJ. , et al. In: LJ. De. Groot and JL. Jameson, editors. Endocrinology: 4 th edition W. B. Saunders Company 1075 – 1093 2001. Silverberg S. J. , et al. J Bone Mineral Res, 1989; 4: 282 – 291. 11. Silverberg S. J. , et al. J Bone Mineral Res, 1989; 4: 282 – 291.
Table 1 – Changing profile of primary hyperparathyroidism* Study Cope Heath et al. (1965 – 1974) Symptomatology (1930 – 1965) Mallette et al. (1965 – 1972) Silverberg et al. (1984 – 1999) Nephrolithiasis (%) 57 51 37 17 Skeletal disease (%) 23 10 14 1. 4 Asymptomatic (%) 0. 6 18 22 80 * Silverberg SJ. , Bilezikian JP. Primary hyperparathyroidism. In: LJ. De. Groot and JL. Jameson, editors. Endocrinology: 4 th edition W. B. Saunders Company 1075 – 1093 2001.
The reason for this dramatic change in disease profile is almost certainly the improved diagnostic approaches. With the advent of the automated chemistry analyzers which routinely measure serum calcium level, the frequency of diagnosis of PHPT has increased dramatically, whereas the classic manifestations of the disease has become much less common. Heath H, et al. N Engl J Med 1980; 302: 189 – 193. Heath H III. J Bone Min Res 1991; 6: Supplement 2: S 63 – S 70. Mundy GR, et al. Lancet. 1980; 1: 1317 – 1320. Scholz DA, et al. Mayo Clin Proc 1981; 56: 473 Silverberg SJ. , et al. In: LJ. De. Groot and JL. Jameson, editors. Endocrinology: 4 th edition W. B. Saunders Company 1075 – 1093 2001.
The story is completely different in hyperparathyroid patients from Iran and other developing countries. There are clearly major differences between features of PHPT in patients from developing countries and those of subjects nations. reported from developed
These differences have led the authors of “The Parathyorids; Basic and clinical concepts, 2 nd ed. Academic Press” to describe the clinical presention of PHPT in developing countries in a separate chapter. CHAPTER 22 Clinical Presentation Hyperparathyroidism of Primary India, Brazil, and China AMBRISH MITHAL The Parathyroids, Basic and clinical concepts, 2 nd ed. Academic Press 2001 John P. Bilezikian et al
The aim of this review is: To analyze the Iranian experiences on the clinical, biochemical radiological and pathological features of PHPT, and To compare these findings with those of patients from developed and other developing countries.
Methods In an effort to obtain Iranian literature on the subject of PHPT, a search was made through multiple data sources including: Pub. Med, Embase, Ovid Medline, Science direct (Elsevier) Scholar Google, ISI, Iranmedex (Farsi) and Irandoc (Farsi) from 1980 – 2006.
Results (1) There were 7 published papers, Three in English (in international journals) and, Four in Persian (local medical journals).
Results (2) Six papers contained comprehensive informations regarding demographic, clinical, laboratory, radiological, and pathological findings in relatively large series of Iranian patients.
Iranian literature on the subject of PHPT 1. Mir Saeid Gazi AA. , Bostani I. , Nasri H. , Amiri Z. , Rahimi F. , et al. Primary hyperparathyroidism: Report of 30 cases. Journal of Research in Medicine (in Farsi) 2000; 23(4): 301 – 308 2. Nakhjavani M, Esteghamati AR, Alam Samimi M. Clinical manifestations and laboratory features of primary hyperparathyroidism; Comparison of 2 decades (1978 – 1988 vs 1988 – 1999) Imam Khomeini Hospital, Tehran. Journal of School of Medicine, Tehran University of Medical Sciences (in Farsi) 2002; 60 (6): 429 – 936 3. Atefi S. Report on patients who have undergone surgery for primary hyperparathyroidism in Shiraz: A 20 - year experience (in Farsi). Iranian J Endocrinol. Metabol 2001 3(4): 277 – 80 4. Bahrami A, Montazeri V, Barband AR, Poorzand A, Mobasseri M. Advanced bone disease as the most common clinical presentation of primary hyperparathyroidism in Iranians: Clinical and laboratory features of 62 patients from north–western Iran. Int J Endocrinol Metab 2006, 4: 19 -29 5. Hamidi S, Soltani A, Hedayat A, Kamalian N. primary hyperparathyroidism: A review of 177 cases. Med Sci Monit, 2006; 12 (2): CR 86 – 89 PMID: 1644995
Table 2 - Results of published studies in PHPT patients from Iran Bahrami Tabriz Atefi Shiraz Gazi Tehran Nakhjavani Tehran Hamidi Tehran 1985 - 2002 1981 - 2000 1987 - 1993 1978 - 1988 1989 - 1998 1981 – 2003 No. of patients 62 40 30 - 47 177 Female to male ratio 5: 1 9: 1 5: 1 - 15: 1 5. 5: 1 Mean age of patients (y) 38. 6 34 36. 2 - 38 42 skeletal skeletal - Bone disease (%) 93. 5% 100% 68% 60% - Renal disease (%) 14. 5% 22. 5% 47% 6. 6% 17% - Asymptomatic hypercalcemia (%) 0 0 12% - Parameter Time period Most common form of presentation Bahrami et al. Int J Endocrinol Metab 2006, 4: 19 -29 Atefi. Iranian J Endocrinol. Metab 2001 3(4): 277 – 80 Gazi et al. Journal of Research in Medicine (in Farsi) 2000; 23(4): 301 – 308 Nakhjavani et al. Journal of School of Medicine, Tehran University of Medical Sciences (in Farsi) 2002; 60 (6): 429 – 936 Hamidi et al. Med Sci Monit, 2006; 12 (2): CR 86 – 89 PMID: 1644995
Demographie, Clinical, Biochemical, Radiological Findings and Parathyroid Gland Weights in Iranian Patients with PHPT Characteristic / Measurement Time period Total number of patients Gender ratio (F: M) Age at presentation (mean SD. Years) Bone disease Osteitis fibrosa cystica Palpable brown tumors Fractures Nephrolithiasis Nephrocalcinosis Serum Calcium /mg/d. L (mean SD) Normal serum calcium (< 10. 2 mg/d. L) Alkaline phosphatase / IU/L (mean SD) PTH / pg /m. L (mean SD) 24 -h Urinary Ca /mg/day (mean SD) Parathyroid gland weight g / mean (range) *reported in 177 cases Iran (Tehran- Shiraz-Tabriz) 1978 – 2003 356 8: 1 39 14 60 – 100% > 50% Frequent 14. 5 – 47% < 5% 11. 2 1. 1 4. 5 – 16. 5% 657 116 513 486 224 129 4. 1 (0. 8 – 25)*
Table 3. Comparison of Demographic Characteristics of Patients with PHPT from Different Countries Characteristic Time period Total number Gender ratio (F: M) Age at presentation (mean SD. Years) United States (New York) United States (Detroit) China (Beijing) India (North) Iran (Tehran- Shiraz. Tabriz) 1984 – 1999 1989 – 1999 1958 – 1993 1973 – 1999 1978 – 2003 143 346 134 93 354 3. 4: 1 3. 7: 1 2. 6: 1 1. 8: 1 55 12 61 14 37 13 35 16 39 14 Mithal et al. The parathyroids: Basic and clinical concepts. 2 nd ed. Academic Press, 2001; 375 – 86 Bahrami et al. Int J Endocrinol Metab 2006, 4: 19 -29 Atefi. Iranian J Endocrinol. Metab 2001 3(4): 277 – 80 Gazi et al. Journal of Research in Medicine (in Farsi) 2000; 23(4): 301 – 308 Nakhjavani et al. Journal of School of Medicine, Tehran University of Medical Sciences (in Farsi) 2002; 60 (6): 429 – 936 Hamidi et al. Med Sci Monit, 2006; 12 (2): CR 86 – 89 PMID: 1644995
Table 4. East – West Comparison of Relevant Clinical Manifestations of PHPT Variable West (historic) West (contemporary) East (historic and contemporary) Iran (Tehran- Shiraz-Tabriz) Bone disease 50 – 60% 10 – 20% 80 – 100% 60 – 100% Osteitis fibrosa cystica 25 – 50% < 2% > 50% Palpable brown tumors Infrequent Almost never Frequent Fractures Frequent Infrequent Frequent Nephrolithiasis 50 – 80% 5 – 20% 10 – 40% 6 – 47% Nephrocalcinosis 5 – 10% Almost never 5 – 10% < 5% Mithal et al. The parathyroids: Basic and clinical concepts. 2 nd ed. Academic Press, 2001; 375 – 86 Bahrami et al. Int J Endocrinol Metab 2006, 4: 19 -29 Atefi. Iranian J Endocrinol. Metab 2001 3(4): 277 – 80 Gazi et al. Journal of Research in Medicine (in Farsi) 2000; 23(4): 301 – 308 Nakhjavani et al. Journal of School of Medicine, Tehran University of Medical Sciences (in Farsi) 2002; 60 (6): 429 – 936 Hamidi et al. Med Sci Monit, 2006; 12 (2): CR 86 – 89 PMID: 1644995
Table 5. Comparison of Relevant Biochemical Findings in Patients with PHPT from Different Countries North America (New York and Detroit) South America and Far East (Brazil, China, and North India) Iran Calcium (mg/d. L) 10. 6 0. 60 11. 5 1. 04 11. 2 1. 1 25 -Hydroxyvitamin D (ng/m. L) 20. 0 10. 0 11. 1 6. 2 - Alkaline phosphatase (IU/L) 110 60 1497 1864 PTH (pg/m. L) 128 96 1024 555 513 486 24 -h Urinary Ca (mg) 249 122 320 160 224 129 Measurement 657 116 Mithal et al. The parathyroids: Basic and clinical concepts. 2 nd ed. Academic Press, 2001; 375 – 86 Bahrami et al. Int J Endocrinol Metab 2006, 4: 19 -29 Atefi. Iranian J Endocrinol. Metab 2001 3(4): 277 – 80 Gazi et al. Journal of Research in Medicine (in Farsi) 2000; 23(4): 301 – 308 Nakhjavani et al. Journal of School of Medicine, Tehran University of Medical Sciences (in Farsi) 2002; 60 (6): 429 – 936 Hamidi et al. Med Sci Monit, 2006; 12 (2): CR 86 – 89 PMID: 1644995
There are clearly major differences between features of PHPT in patients from developing countries and those of subjects nations. reported from developed
The differences are: • In the West PHPT mainly affects middle aged females with a peak incidence in the fifth to sixth decades of life and a female to male ratio, of 2– 3: 1. In developing countries, the peak incidence among both sexes reported to be in the fourth decade of life. In other word, the patients from developing countries belonged to younger age groups. Cheung PSY, et al. Surgery 1988; 103: 558 – 62. Fouda MA. Ann. Saudi Med 1999; 19(2): 110 – 115 1999 Kapur MM, et al. Ind J Med Res 1985; 81: 607 – 12. Harinarayan CV, et al. Clin Endocrinol 1995; 43: 351 – 8. Mishra SK, et al. Br J Surg. 2001; 88: 708 – 714 Atefi S. Iranian J Endocrinol. Metabol 2001 3(4): 277 – 80 Bhonsali A. , et al. Ann Saudi Med 2005; 25: 29 – 35 Arshad MS, et al. 13 th Asia-Oceania Congress of Endocrinology. 2006, May 10– 12, Tehran Iran Pp 170 -71(P-172) Bahrami A, et al. Int J Endocrinol Metab 2006, 4: 19 -29
2) The vast majority of patients from developing countries present with severe bone disease. Experiences, from several developing countries including our owns show a high percentage of advanced bone disease in patients with PHPT. Cheung PSY, et al. Surgery 1988; 103: 558 – 62. Fouda MA. Ann. Saudi Med 1999; 19(2): 110 – 115 1999 Kapur MM, et al. Ind J Med Res 1985; 81: 607 – 12. Harinarayan CV, et al. Clin Endocrinol 1995; 43: 351 – 8. Mishra SK, et al. Br J Surg. 2001; 88: 708 – 714 Atefi S. Iranian J Endocrinol. Metabol 2001 3(4): 277 – 80 Bhonsali A. , et al. Ann Saudi Med 2005; 25: 29 – 35 Arshad MS, et al. 13 th Asia-Oceania Congress of Endocrinology. 2006, May 10– 12, Tehran Iran Pp 170 -71(P-172) Bahrami A, et al. Int J Endocrinol Metab 2006, 4: 19 -29
3) Renal disease is considerably less frequent in patients with PHPT from developing counties. This is in sharp contrast to the results reported from Western countries, where prior to the introduction of routine serum calcium measurement, renal disease was the most common clinical form of PHPT. Cope O. N Engl J Med 21: 1174 – 1182, 1966. Mallette LE, et al. Medicine (Baltimore) 53: 127 – 147, 1974. Heath H, et al. N Engl J Med 1980; 302: 189 – 193.
4) Normocalcemic PHPT with bone and/or stone disease is an exception rather than the rule in the West. In contrast, the prevalence of normocalcemic hyperparathyroidism has been reported from 3 – 50% in developing countries Frame, B. , et al. Annals of Internal Medicine 1970, 73: 253 – 257. Wills, M. R. , et al. Am J Med 1969, 47: 384 – 391. Fouda MA. Ann. Saudi Med 1999; 19(2): 110 – 115 1999 Kapur MM, et al. Ind J Med Res 1985; 81: 607 – 12. Harinarayan CV, et al. Clin Endocrinol 1995; 43: 351 – 8. Mishra SK, et al. Br J Surg. 2001; 88: 708 – 714 Atefi S. Iranian J Endocrinol. Metabol 2001 3(4): 277 – 80 Bhonsali A. , et al. Ann Saudi Med 2005; 25: 29 – 35 Arshad MS, et al. 13 th Asia-Oceania Congress of Endocrinology. 2006, May 10– 12, Tehran Iran Pp 170 -71(P-172) Bahrami A, et al. Int J Endocrinol Metab 2006, 4: 19 -29
The Qeustion is: What are the main responsible factors for many of the major differences in presentation of PHPT between patients from developing nations and those from developed countries?
The reason why patients from developing nations present at a younger age is not clear. Obviously delay in diagnosis is not a logical explanation. If the basis for advanced disease in the developing countries were due mainly to a delay in diagnosis, one would have expected a greater mean age rather than lower. Further more, long term follow up of patients with mild asymptomatic hyperparathyroidism has not been associated with progression of the disease to advanced form
Could vitamin D deficiency be the main responsible factor for many of the major differences in presentation of PHPT between patients from developing nations and those from developed countries?
Some investigators explained the high percentage of bone involvement with florid presentation by the: common coexistence of vitamin D deficiency prolonged PHPT, and low calcium intake Harinarayan CV, et al. Clin Endocrinol 1995; 43: 351 – 8. Woodhouse NJ, et al. Lancet 1971, 7: 283 -6. Lumb GA, et al. Am J Med 1974, 56: 833 -9 Nordenstrom E, et al. World Surg 2002, 26: 1463 -7.
Results of some investigations have shown that vitamin D status might influence the clinical and biochemical features of PHPT. Woodhouse NJ, et al. Lancet 1971, 7: 283 -6. Lumb GA, et al. Am J Med 1974, 56: 833 -9 Nordenstrom E, et al. World Surg 2002, 26: 1463 -7.
Low serum vitamin D level in patients with PHPT was associated with worsening: laboratory, densitometric and histomorphometric indices of bone involvement and high risk of fractures. Roa DS, et al. J Clin Endocrinol Metab 2000, 85: 1054 -8 Roa DS, et al. J Bone Miner Res 2002, 17(Suppl 2): N 75 -80.
Results of many studies have shown that coexisting vitamin D deficiency might result in advanced osteitis fibrosa cystica. Silverberg SJ, et al. Am J Med. 1999, 107: 561 – 567. Parfitt AM, et al. Am J Clin Nutr 1982, Suppl 5: 1014 – 1031. Insogna, K, L. , et al. New England Journal of Medicine 1985, 313: 1126 – 1130. Dent. CE. , et al. Lancet 1961, ii, 336 – 338.
Some investigators have reported that: parathyroid gland weight was greater in patients with PHPT who had coexisting vitamin D deficiency and severe bone disease Roa DS, et al. J Clin Endocrinol Metab 2000, 85: 1054 -8 Moosgaard, et al. Clin Endocrinol (Oxf) 2005, 63: 506 -13.
On the other hand, supplementation with calcium and vitamin D was associated with a significant increase in bone mineral density in PHPT patients with coexisting vitamin D deficiency. Bilezikian JP, et al. J Bone Miner Res 2002, 17: N 2 -11.
Such observations have led an expert panel to offer vitamin D supplements to asymptomatic PHPT patients with coexisting vitamin D deficiency. Bilezikian JP, et al. J Bone Miner Res 2002, 17: N 2 -11.
The studies carried out in the preceding two decades have shown a high prevalence of vitamin D deficiency in developing countries including: China, Turkey, India, Iran and Saudi Arabia, which varied between 30% and 93%. Sedrani SH. Ann Nutr Metab 1984, 28: 181 – 185. Sedrani SH, et al. Am J Clin Nutr 1983, 38: 129 – 132. Azizi F, et al. Research in Medicine ( in Farsi) 2000, 4: 291 – 303 Taha S, et al. Pediatr Res 1984, 18: 739 – 741 Fonseca V, et al. Postgrad Med J 1984, 60: 589 – 591. Gowami R, et al. Am J Clin Nutr 2000, 72: 422 – 475. Sima Hashemipour, et al. BMC Public Health 2004, 4: 38.
Recent studies performed in our country showed high prevalence of vitamin D deficiency in adult urban populations of both sexes. Sima Hashemipour, et al. BMC Public Health 2004, 4: 38. Bahrami A. , et al First International Seminar on Prevention, Diagnosis and Treatment of Osteoporosis. Pp 29 – 30, September 23 – 24, 2004 Tehran Iran
Due to a widely prevalent vitamin D deficiency in developing countries, highly prevalent and advanced bone disease in hyperparathyroid patients can be attributed to a coexisting vitamin D deficiency. Sedrani SH. Ann Nutr Metab 1984, 28: 181 – 185. Sedrani SH, et al. Am J Clin Nutr 1983, 38: 129 – 132. Azizi F, et al. Research in Medicine ( in Farsi) 2000, 4: 291 – 303 Taha S, et al. Pediatr Res 1984, 18: 739 – 741 Fonseca V, et al. Postgrad Med J 1984, 60: 589 – 591. Gowami R, et al. Am J Clin Nutr 2000, 72: 422 – 475. Sima Hashemipour, et al. BMC Public Health 2004, 4: 38. Bahrami A. , et al First International Seminar on Prevention, Diagnosis and Treatment of Osteoporosis. Pp 29 – 30, September 23 – 24, 2004 Tehran Iran
Obviously vitamin D deficiency is not the only factor in determining the severity of bone involvement in hyperparathyroid patients from developing nations. Other but yet unknown, pathogenetic factors may have contributory role.
In conclusion: PHPT is a severe, symptomatic disease with serious complications and high morbidity in developing countries. § Advanced skeletal disease is the most common pattern of presentation at a young age. § Vitamin D deficiency might influence the clinical and biochemical expression of PHPT.
Recommondations § Routine measurement of serum calcium at least in high risk subjects (middle aged females), Investigation of vitamin D status in PHPT patients in Iran vitamin D supplementation and, awareness of protean manifestation of the disease
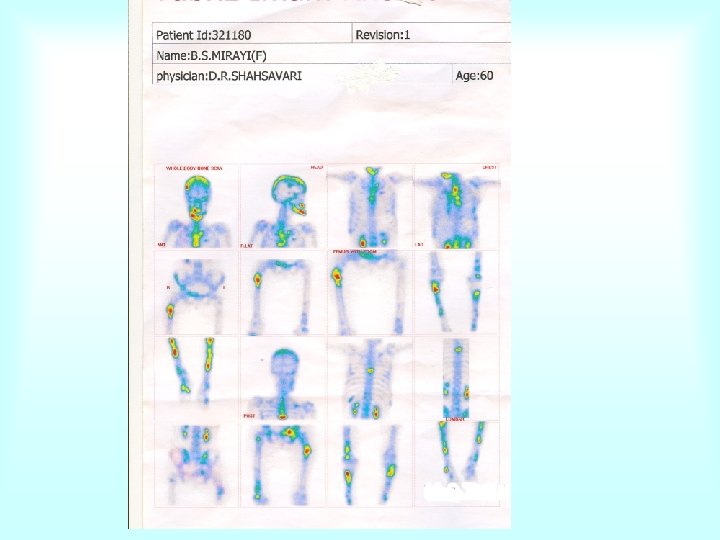
Primary Hyperparathyroidism in Developing Countries A breif report of a case from Iran Mrs. Simin Miraei A 41 year old female admitted at hospital with: bone pains, bony deformities and multiple fractures
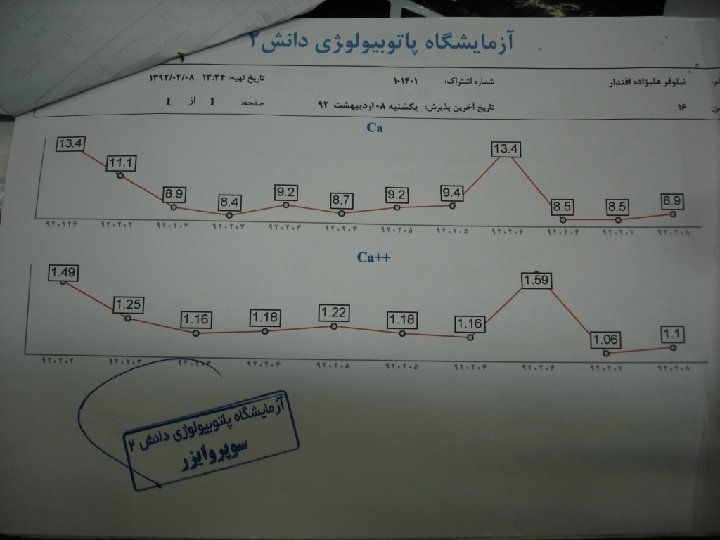
Biochemical profile Hb = 10. 6 g / d. L Serum creatinine = 0. 8 mg / d. L Serum Na+ = 141 m. Eq / L Serum K+ = 3. 9 m. Eq / L Serum TSH = 2. 6 m. IU / L Serum Mg = 2. 3 mg / d. L Serum ionized ca++ = 1. 58 – 1. 75 mmol / L ( N = 1. 1 – 1. 3) Serum phosphorus = 1. 9 – 2. 2 mg / d. L Alk. phosphatase = 633 IU /L (N = 64 – 306) Serum PTH = 4400 pg / m. L 24 hour urinary calcium = 436 mg / day
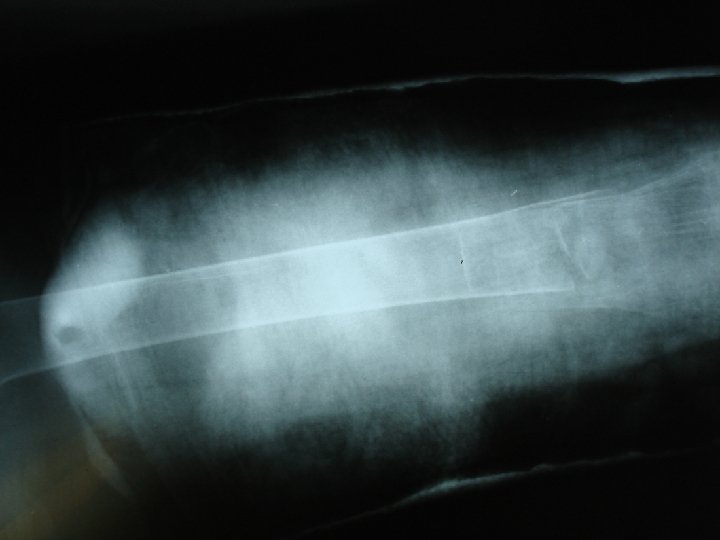
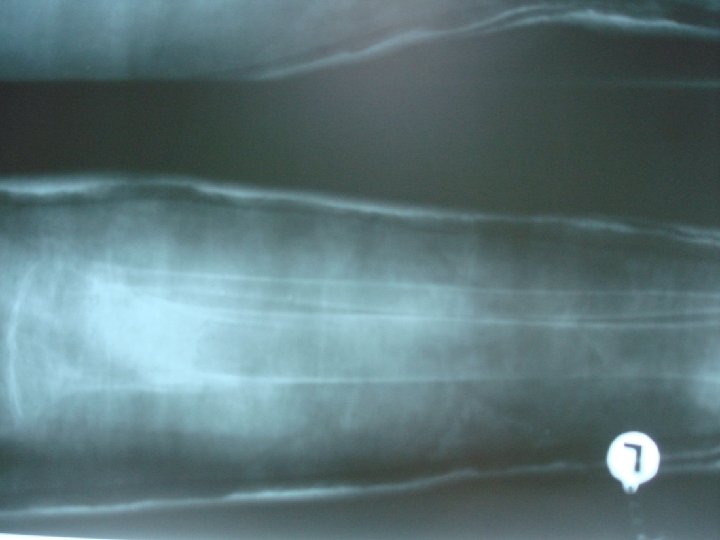
Radiological Findings Multiple bone cysts, Multiple bony fractures involving: Hip Femur Tibia ¨ Spines KUB: Bilateral renal stone disease
Jaw tumor
Limb deformity due to proximal tibial fracture
Brown tumor
pathologic fracture
Lytic lesions
Multiple bone cysts and fractures
Bilateral kidney stones
Compression fracture of a thoracic spine
Proximal femural fracture
Bilateral proximal tibial fractures
Bone scan Multiple lytic lesions involving almost all the skeletal system
Surgical Finding Large left upper parathyroid adenoma
Postoperative Course Hypocalcemic crisis Serum PTH = 11. 6 pg / m. L Serum calcium = 6. 5 mg / d. L Serum phosphorus = 2. 6 mg / d. L
Thank you for your attention
1. Azizi F, Rais-Zadeh F, Mir Said Ghazi A; Vitamin D deficiency in a group of Tehran population. Research in Medicine ( in Farsi) 2000, 4: 291 – 303 2. Mirsaeid Ghazi AA, Rais Zadeh F, Pezeshk P, Azizi F: Seasonal variation of serum 25 hydroxy D 3 in residents of Tehran. J Endocrinol Invest, 2004; 27(7): 676 – 79 3. Moussavi M, Heidarpour R, Aminorroaya A et al: Prevalence of Vitamin D Deficiency in Isfahani High School Students in 2004. Horm Res, 2005; 64(3): 144 – 48 4. Bahrami A. , Pourdolati S. , Bolandi A. , Nikniaz AR Koosha A Sohrabi H. Prevalence of vitamin D deficiency in an urban adult population. Proceedings of First International Seminar on Prevention, Diagnosis and Treatment of Osteoporosis. Pp 29 – 30, September 23 – 24, 2004 Tehran Iran 5. Hashemipour S, Bagher Larijani, Hossein Adibi, et al: vitamin D deficiency and causative factors in the population of Tehran. BMC Public Health 2004, 4: 38.
Table 6. Comparison of Biochemical Findings and Parathyroid Gland Weights in Patients from the US and India with Comparable Serum Levels of 25 -OH Vitamin D United States (Detroit) India (Dehli and Lucknow) P 51 27 - 62 14 36 18 < 0. 001 25 -Hydroxyvitamin D (ng/m. L) 9. 29 3. 79 10. 22 6. 17 0. 412 Parathyroid gland weight (g) 1. 66 1. 75 7. 21 7. 48 < 0. 001 PTH (pg/m. L) 172 192 1024 565 < 0. 001 Alkaline phosphatase (IU/L) 141 113 963 1456 < 0. 001 Measurement Number of patients Age (years)