Primary Bone Marrow Triple Hit Follicular Lymphoma Jian

Primary Bone Marrow Triple Hit Follicular Lymphoma Jian Shen, MD Ph. D 1, Bhavana Dave, Ph. D 2, and Gabriel C. Caponetti, MD 1 1. CHI Creighton University Medical Center, Omaha, Nebraska, USA 2. University of Nebraska Medical Center, Omaha, Nebraska, USA
 • A 62 year-old male without any significant past medical")
Clinical Presentation (June 2014) • A 62 year-old male without any significant past medical history presents with numbness around his left lips, temporomandibular joint and burning eye pain. These symptoms progressively worsened until January 2015 when symptoms began to spontaneously improve. • A physical and neurological evaluation did not identify a specific reason for these symptoms. • Laboratory tests: CBC, TSH, B 12, rheumatoid factor, ACE inhibitor, ANA screening test, serum protein electrophoresis, liver and renal function tests, and electrolytes were all within normal limits.
 • Review of systems: no history of fevers, fatigue or")
Clinical Presentation (June 2014) • Review of systems: no history of fevers, fatigue or loss of appetite. Intentional weight loss of 40 kg over several months. • Physical exam: Unremarkable. lymphadenopathy. Without • The neurologic symptoms progressively worsened until January 2015 when they spontaneously began to improve.

Imaging Studies • April 2015: An MRI of the brain showed indeterminate marrow replacement of the left mandible, possibly osteitis or a neoplastic process. • May 2015: A whole body MRI showed multiple patchy areas of abnormal bone marrow signal throughout the cervical, thoracic and lumbar spine, the pelvis and both femurs. The findings were highly worrisome for a neoplastic process.
")
CBC (06/03/15)

06/03/15: Peripheral blood smear: Occasional small cleaved lymphoid cells
 H&E, 4 x")
Bone Marrow Biopsy (06/03/15) H&E, 4 x

H&E, 4 x

H&E, 20 x

H&E, 100 x

H&E, 100 x
")
CD 20 (4 x)

CD 20 CD 3 CD 10 BCL 6

BCL 2 Ki 67 MYC FOXP 1

Ki 67

Bone Marrow Immunohistochemistry • CD 20 and PAX 5: Positive (approximately 40% of all cells). Highlight the paratrabecular distribution of the lymphoma cells. • CD 3: Negative (highlights a large number of T-cells admixed with the lymphoma cells). • BCL 6: Positive • CD 10: Positive • BCL 2: Positive • Ki 67: Positive in up to 10% of the lymphoma cells. • FOXP 1: Positive • MYC: Positive in up to 10% of the lymphoma cells. • CD 34: Negative • Td. T: Negative • Cyclin D 1: negative
")
Reticulin stain (moderate diffuse, 2+/3+)

Bone Marrow Touch Imprints

Differential Cell Count on Bone Marrow Touch Imprints • • • Neutrophils 17 % (reference value 25 -40%). Metamyelocytes 0 % (reference value 5 -15%). Myelocytes 0. 5 % (reference value 10 -13%). Promyelocytes 0 % (reference value 2 -8%). Blasts 0 % (reference value 0 -3%). Basophils 0 % (reference value 0 -1%). Eosinophils 2 % (reference value 1 -5%). Monocytes 0. 5 % (reference value 0 -2. 6%). Lymphocytes 79 % (reference value 2. 5 -15%). Plasma cells 0 % (reference value 0 -3%). Early erythroid precursors 0 % (reference value 0 -2%). Late erythroid precursors 1. 5 % (reference value 15 -25%).

Bone Marrow Flow Cytometry INTERPRETATION: Monoclonal CD 10 -positive B-cell population identified. Comment: A mature B-cell population expressing low-density CD 19, low-density CD 20, lowdensity CD 10, low-density CD 38, CD 23, BCL 2 and low-density monotypic surface lambda immunoglobulin light chains is identified at 23% of the events in the lymphocyte gate (6% of leukocytes) (the monocyte gate does not contain any B-cells). This monoclonal population is likely of small size, based on its low forward light scatter signal. The T and NK cells are immunophenotypically unremarkable. These findings are consistent with a B-cell lymphoproliferative disorder and suggest a germinal center origin.

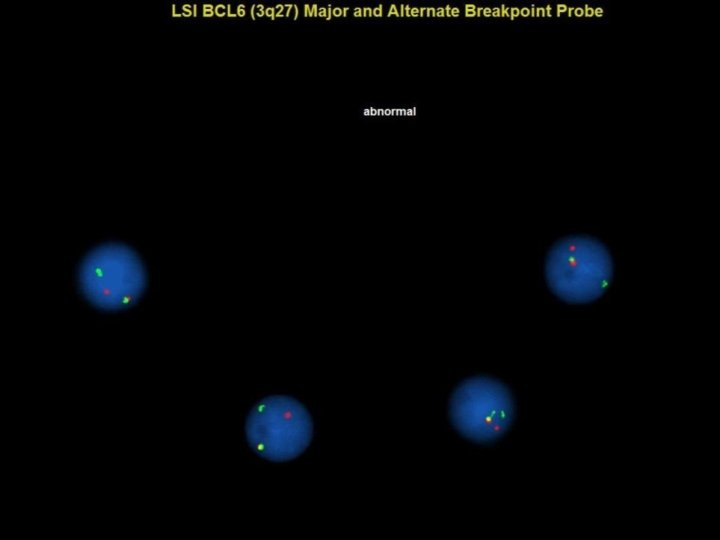
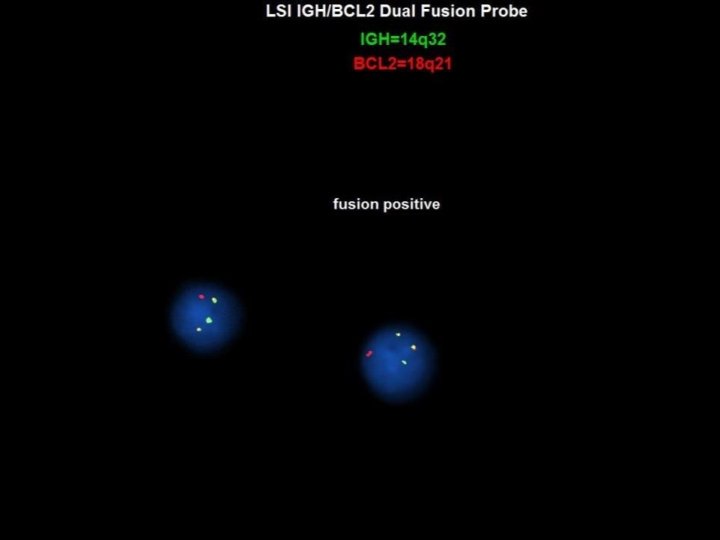
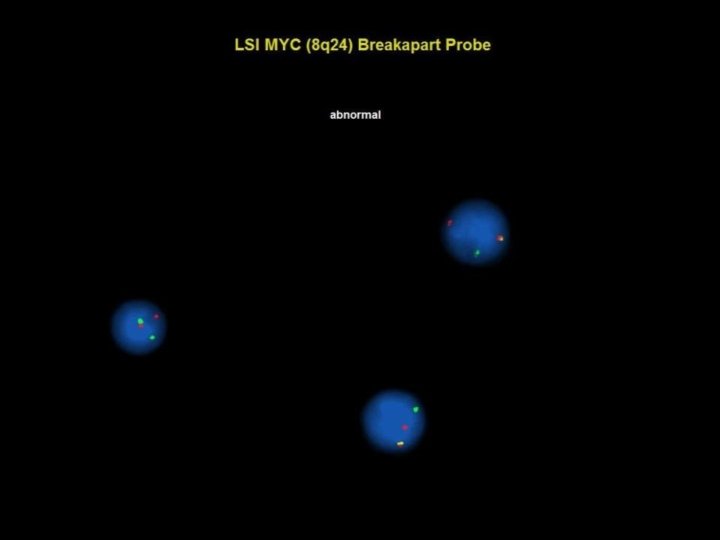
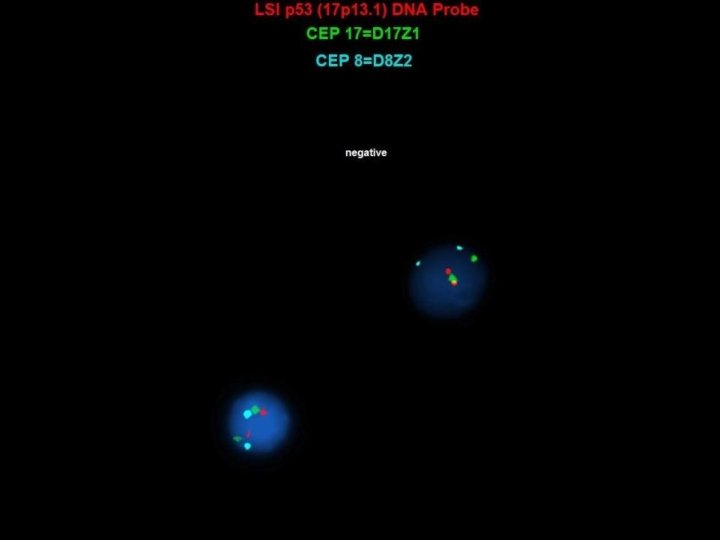
Bone Marrow Cytogenetic Studies • FISH cytogenetic findings indicative of a “triple-hit” lymphoma: § Positive for IGH/BCL 2 fusion (10. 5% of the interphase cells ) § Positive for rearrangement of the BCL 6 (3 q 27) major and alternate breakpoint locus (14% of the interphase cells) § Positive for rearrangement of the MYC (8 q 24) locus (20% of the interphase cells) § Negative for deletion of 17 p 13. 1 • Karyotype: normal male complement: 46, XY [20 cells analyzed, 3 karyotyped]
 • June 2015:")
Staging PET/CT Scan (done after the diagnosis of bone marrow lymphoma) • June 2015: Whole body PET/CT showed extensive axial, and hypermetabolic bone marrow lesions. The findings were consistent with bone marrow neoplastic process. However, no solid organ hypermetabolic lymph nodes, masses or lesions were identified.

June 2015: A PET/CT scans showed only hypermetabolic bone marrow lesions.

Proposed Diagnosis Primary Bone Marrow Triple Hit Follicular Lymphoma

Interesting findings • Isolated bone marrow involvement by a morphologically low grade B-cell lymphoma with cytogenetic abnormalities typically associated with an aggressive clinical course. • In follicular lymphoma, MYC rearrangement can be seen in a few cases of extramedullary recurrent disease. However, in the present case there is no evidence of nodal disease.

Discussion • Although the FISH cytogenetic findings in this case indicate the presence of a "triple hit" lymphoma, there is no morphologic evidence of transformation to a large cell or blastoid process, and the ki 67 is low. • The patient is currently asymptomatic and not being treated (“watch and wait” approach). • The literature indicates that most double and triple hit lymphomas are most commonly associated with an aggressive clinical course. However, a few double and triple hit follicular lymphomas with a low grade morphology, relatively low ki 67, and an indolent clinical course have been described (see references).

Discussion • MYC rearrangements can be seen in a small fraction of follicular lymphomas that transform to aggressive lymphomas but not in the corresponding antecedent follicular lymphomas. This suggests that acquisition of a MYC rearrangement is in some cases associated with the transformation event. • BCL 2 rearrangements are thought to be mediated by aberrant RAG 1/2 activity during VDJ recombination in the bone marrow, whereas MYC rearrangements probably occur in germinal center B-cells due to aberrant somatic hypermutation or illegitimate class switch recombination mediated by AICD (activation induced cytidine deaminase). • However, the current case raises the possibility that MYC rearrangements also occur in the bone marrow. Alternatively, it is possible that in a few cases of follicular lymphoma, the lymphoma cells with a BCL 2 rearrangement exit the bone marrow, acquire a MYC rearrangement in the germinal centers without necessarily causing nodal disease, and then return to the bone marrow where they proliferate and infiltrate.
 Aukema et al. Double-hit B-cell lymphomas. Blood. 2011. 24; 117(8): 2319 -31.")
References 1) Aukema et al. Double-hit B-cell lymphomas. Blood. 2011. 24; 117(8): 2319 -31. 2) Wang et al. Triple-hit B-cell Lymphoma With MYC, BCL 2, and BCL 6 Translocations/Rearrangements: Clinicopathologic Features of 11 Cases. Am J Surg Pathol. 2015; 39(8): 1132 -9. 3) Koduru et al. Acquisition of a t(11; 14)(q 13; q 32) in clonal evolution in a follicular lymphoma with a t(14; 18)(q 32; q 21) and t(3; 22)(q 27; q 11. 2). Cancer Genet. 2015; 208(6): 303 -9. 4) Christie et al. C-MYC translocation in t(14; 18) positive follicular lymphoma at presentation: An adverse prognostic indicator? Leuk Lymphoma. 2008; 49(3): 4706. 5) Yano T, Jaffe ES, Longo DL, Raffeld M. MYC rearrangements in histologically progressed follicular lymphomas. Blood. 1992; 1; 80(3): 758 -67.
- Slides: 32