Primair cystocoeleherstel Steven Weyers Vrouwenkliniek UZ Gent Symptomatologie






 • Is er een relatie tussen")

 WAARSCHIJNLIJK • Is er een relatie")

 • Is er een relatie tussen")
 • Elk instrument dat in de")

 • • Maat? Grootste dat nog")

 (1) • Eerst beschreven door Kelly in")
 °openen vaginale mucosa °vrijprepareren fascia °hechten defect in fascia °reseceren overtollige")
 • Complicaties: zeldzaam – intra-operatief: • hemorrhagie, heel zelden bloedtransfusie nodig")
 • Postoperatieve zorgen: – Hospitalisatie: • wiek 24 uur • blaassonde")
 • Resultaten: – weinig studies met lange FU, slechts enkele prospectief")
 Glazener CMA, Cooper K")
 (1) • Eerst beschreven door White")
 (2)")
 (3) • Complicaties: idem colporraphia anterior (CA) • Postoperatieve zorgen:")
 • Eerst beschreven door Raz")
 • Resultaten: – Raz et al, J Urol 1989;")
 • Idealiter: –")






- Slides: 35
Primair cystocoeleherstel Steven Weyers Vrouwenkliniek UZ Gent
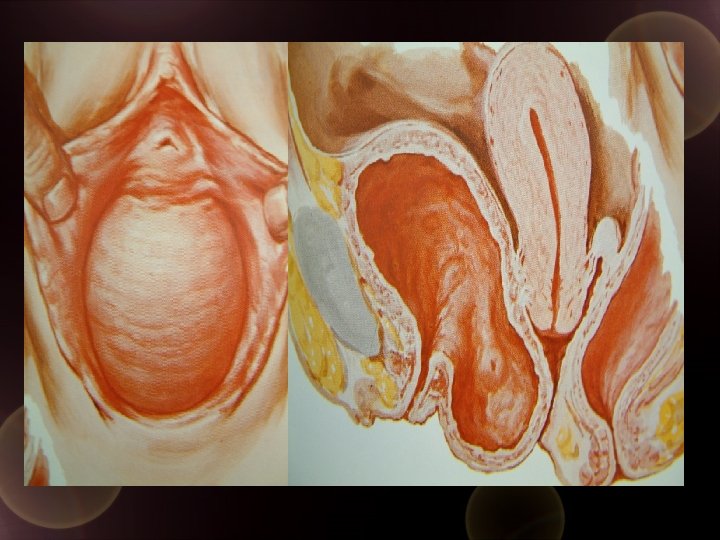
Symptomatologie • direct gerelateerd aan prolaps: • bolgevoel, massagevoel vaginaal, drukgevoel • lage rugpijn • coïtale problemen • geassocieerde klachten: • stressincontinentie • mictieproblemen (dysurie, nycturie, pollakisurie, urgency)
Diagnostiek • Klinisch onderzoek: • gynaecologische houding – met dorsale retraktor – in rust en na valsalva • staand • Diagnostische tests: • uroflow met residubepaling • urodynamisch onderzoek ± pessarium
Behandeling van cystocoele • waarde van conservatieve maatregelen – kiné – wijziging van levenspatroon – pessarium • chirurgische technieken
Conservatieve behandeling van genitale prolaps: kiné • geen enkele aanwijzing dat fysiotherapie van de bekkenbodem enige waarde heeft in de behandeling van genitale prolaps • ‘Conservative management of pelvic organ prolapse in women. ’The Cochrane Library, Issue 4, 2004. ‘Currently there is no rigorous evidence from randomised controlled trials regarding the use of conservative interventions in the management of pelvic organ prolapse. ’ • ICS 2003: 92% (n=333) of the respondents were assessing/treating women with pelvic organ prolapse.
Conservatieve behandeling van genitale prolaps: invloed levenspatroon (1) • Is er een relatie tussen zware fysieke arbeid en genitale prolaps? • Is er een invloed van factoren zoals overgewicht, COPD, constipatie, . . . ?
Heavy lifting at work and risk of genital prolapse and herniated lumbar disc in assistant nurses S Jorgensen, HO Hein and F Gyntelberg Occupational Medicine 1994, Vol 44, Issue 1 47 -49 • Deense verpleegkundigen (28. 619) vs alg populatie (1. 652. 533) • OR 1. 6 op ingreep voor prolaps • Conclusie: tillen van zware lasten zou oorzaak kunnen zijn van meer prolaps in deze groep • Commentaar: belangrijke bias> toegankelijkheid chirurgie
Conservatieve behandeling van genitale prolaps: invloed levenspatroon (1) WAARSCHIJNLIJK • Is er een relatie tussen zware fysieke arbeid en genitale prolaps? • Is er een invloed van factoren zoals overgewicht, COPD, constipatie, . . . ?
Bowel dysfunction: a pathogenic factor in uterovaginal prolapse and urinary stress incontinence. Spence-Jones C, Kamm MA, Henry MM, Hudson CN. Br J Obstet Gynaecol. 1994 Feb; 101(2): 147 -52. • Observationele studie 23 prolaps/23 SI/27 controles • Vragenlijst • Moeizame stoelgang als jong volwassene >prolaps/SI • Stoelgangsfrequentie <2/week als jong volwassene >prolaps
Conservatieve behandeling van genitale prolaps: invloed levenspatroon (2) • Is er een relatie tussen zware fysieke arbeid en genitale prolaps. WAARSCHIJNLIJK • Is er een invloed van factoren zoals overgewicht, COPD, constipatie, . . WAARSCHIJNLIJK MAAR WIJZIGING VAN LEVENSPATROON HEEFT WELLICHT GEEN THERAPEUTISCH EFFECT OP EEN REEDS BESTAANDE PROLAPS
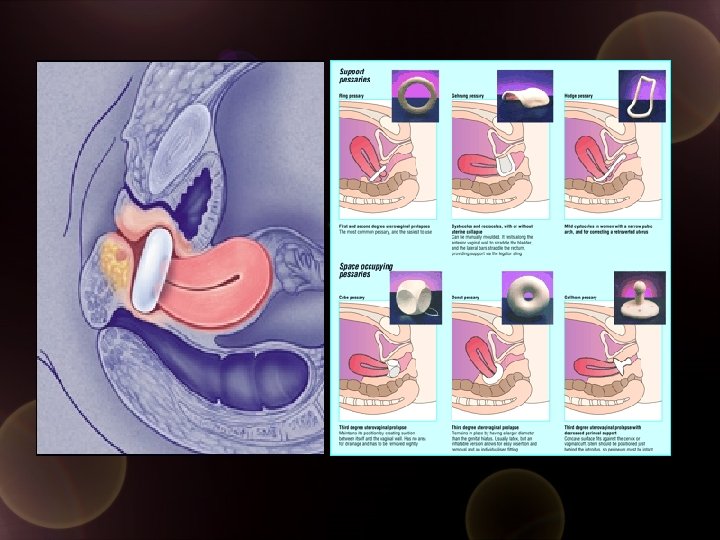
Conservatieve behandeling van genitale prolaps: het pessarium (1) • Elk instrument dat in de vagina wordt geplaatst ter ondersteuning van blaas, uterus en/of rectum • Acryl, silicone, latex • Diagnostisch/Symptomatisch/Palliatief • Niet therapeutisch • ‘Mechanical devices for pelvic organ prolapse in women. ’ The Cochrane Library, Issue 4, 2004 ‘Currently there is no evidence from randomised controlled trials upon which to base treatment of women with pelvic organ prolapse through the use of mechanical devices/pessaries. ’
Conservatieve behandeling van genitale prolaps: het pessarium (2) • • Maat? Grootste dat nog comfortabel zit (7 -9) Gezonde mucosa Wisselen (3 -4 maanden) Complicaties – erosie, incarceratie, fistelvorming – infektie, slechtruikende fluor, bloeding – UWI, stressincontinentie, urineretentie • Contra-indicaties – aktieve infectie, abnormaal bloedverlies
Heelkundige behandeling van cystocoele • Geen gouden standaard • Technieken: – Colporraphia anterior – (Vaginal) Paravaginal Repair ((V)PVR) – Raz 4 -courner repair • Gebruik van meshes
Heelkundige behandeling van cystocoele: Colporraphia anterior (CA) (1) • Eerst beschreven door Kelly in 1913 • Objectief: herstellen van het defect in de fascia pubocervicalis • Techniek: hydrodissectie onder de mucosa (1: 200. 000 adrenaline) openen van de vaginale mucosa op de middellijn vaginatop/cervix tot aan de urethrovesicale junktie (ongeveer 2 -3 cm onder meatus), vrijprepareren van de mucosa van de fascia (op de blaas laten) met schaar of bistouri, approximatie van de fascia op de middellijn, eventueel resektie van overtollige vaginale mucosa en sluiten ervan • Opm. : wellicht enkel efficiënt voor centraal defect in fascia
Colporraphia anterior (2) °openen vaginale mucosa °vrijprepareren fascia °hechten defect in fascia °reseceren overtollige mucosa °sluiten van de mucosa
Colporraphia anterior (3) • Complicaties: zeldzaam – intra-operatief: • hemorrhagie, heel zelden bloedtransfusie nodig • blaas- urether- of urethraletsel – postoperatief: • • • cystitis (10%) hematoomvorming (wiek) urineretentie fistelvorming <dyspareunie
Colporraphia anterior (4) • Postoperatieve zorgen: – Hospitalisatie: • wiek 24 uur • blaassonde 1 -5 dagen • eventueel residubepaling tot <100 cc – Thuis: geen
Colporraphia anterior (5) • Resultaten: – weinig studies met lange FU, slechts enkele prospectief vergelijkende studie tussen ‘verschillende technieken’ – Weber et al, Obstetrics and Gynecology 1997; 89: 311 -18 • Medline review 1966 -1995 • Recurrence van 0 (mean FU 1, 2 y) tot 20% (FU 5 -20 y) – Maher et al, Int Urogynecol J 2006; 17: 195 -201 • Medline review 1966 -2004 • Recurrence van 0 tot 40% (Weber 2001, FU 1 y) – niet geschikt als techniek voor SI
Anterior vaginal repair for urinary incontinence in women (Cochrane Review) Glazener CMA, Cooper K Objectives: To determine the effects of anterior vaginal repair (anterior colporrhaphy) on urinary incontinence in comparison with other management options. Selection criteria: Randomised or quasi-randomised trials that included anterior vaginal repair for the treatment of urinary incontinence. Reviewers' conclusions: There were not enough data to allow comparison of anterior vaginal repair with physical therapy or needle suspension for primary urinary stress incontinence in women. Open abdominal retropubic suspension appeared to be better than anterior vaginal repair judged on subjective cure rates in eight trials, even in women who had prolapse in addition to stress incontinence (six trials). The need for repeat incontinence surgery was also less after the abdominal operation. However, there was not enough information about post-operative complications and morbidity. Citation: Glazener CMA, Cooper K. Anterior vaginal repair for urinary incontinence in women (Cochrane Review). In: The Cochrane Library, Issue 4, 2004. Chichester, UK: John Wiley & Sons, Ltd.
Heelkundige behandeling van cystocoele: Vaginal Paravaginal Repair (VPVR) (1) • Eerst beschreven door White in 1909 • Objectief: herstellen van de aanhechting van de laterale vagina aan de arcus tendineus fascia pelvis (ATFP of white line)= site specific repair; kan vaginaal of abdominaal • Techniek: zoals CA met vrijprepareren (>stomp) van retropubische ruimte en lateraal tot aan de spina ischiadica, vervolgens 3 à 4 onoplosbare hechtingen doorheen de ATFP musculus obturator internus vertrekkend net boven spina en eindigend thv de urethrovesicale junktie en vervolgens doorheen de fascia vagina (epitheel intact laten, zoals bij SSF)
Vaginal Paravaginal Repair (VPVR) (2)
Vaginal Paravaginal Repair (VPVR) (3) • Complicaties: idem colporraphia anterior (CA) • Postoperatieve zorgen: idem CA • Resultaten: alleen studies met korte FU – White, Am J Obst Dis Women Child 1912; 65: 286 -290 • 100% success rate tot 3 jaar (19 patients) – Weber et al, Obstet Gynecol 1997; 89: 311 -18 • Medline review 1966 -1995 • recurrence 0 (FU <3 y) tot 7% (mean FU 1, 6 y) via vaginale route • recurrence 3 (mean FU 1, 7 y) tot 5% (FU <4 y) via abdominale route – Maher et al, Int Urogynecol J 2006; 17: 195 -201 • Medline review van 1966 -2004 • recurrence 0 (FU <3 y) tot 33% (mean FU 1, 6 y) via vaginale route • recurrence 3 (FU 1, 7 y) tot 24% (FU 17 m) via abdominale route
Heelkundige behandeling van cystocoele: Raz 4 -courner repair (1) • Eerst beschreven door Raz in 1989 • Objectief: Ophanging van de vagina door permanente hechtingen doorheen de fascia van de rectusspieren • Techniek: variant op de Raz blaashalssuspensie ter behandeling van stress-incontinentie, gecombineerde vaginaal -abdominale techniek. 2 para-urethrale hechtingen en 2 meer craniaal en lateraal doorheen de fascia pubocervicalis met niet-resorbeerbare draad, deze dmv suprapubisch ingebrachte naald doorheen de fascia van de rectusspieren halen en knopen op deze fascia met minimale tensie.
Raz 4 -courner repair (2) • Resultaten: – Raz et al, J Urol 1989; 142: 712 -715 • recurrence 2% (FU 2 y, 107 patients) – Weber et al, Obstet Gynecol 1997; 89: 311 -18 • Medline review 1966 -1995 • recurrence 2 (FU 2 y) tot 59% (FU 3, 5 -4 y) – Maher et al, Int Urogynecol J 2006; 17: 195 -201 • Medline review van 1966 -2004 • recurrence 2 (FU 2 y) tot 57% (FU 4 y)
Heelkundige behandeling van genitale prolaps: zin en onzin van meshes (1) • Idealiter: – maximale steun – soepel – minimale rejectie, infektie en erosie • Types: – synthetisch – biomateriaal: autograft xenograft
Anterior colporrhaphy: a randomized trial of 3 surgical techniques. Weber Anne M et al, AJOG 2001; 185: 1299 -1306 Objective: compare outcomes of 3 different techniques Study design: 109 women with anterior vaginal prolapse were randomly assigned to undergo anterior repair by one of 3 techniques: standard, standard plus polyglactin 910 mesh (Vicryl), or ultralateral anterior colporrhaphy. Results: • At a median length of follow-up of 23. 3 months, • endpoint: satisfactory or optimal anatomic results • 10 of 33 patients (30%) in the standard anterior colporrhaphy group • 11 of 26 patients (42%) with standard plus mesh • 11 of 24 patients (46%) with ultralateral anterior colporrhaphy (ns). • The severity of symptoms that were related to prolapse improved markedly (preoperative score, 6. 9 ± 2. 7; postoperative score, 1. 1 ± 0. 8) • 26 patients were lost to FU. Conclusions: These 3 techniques of anterior colporrhaphy provided similar anatomic cure rates and symptom resolution. The addition of polyglactin 910 mesh did not improve the cure rate compared with standard anterior colporrhaphy (small groups)
Prsopective randomized trial of polyglactin 910 mesh to prevent recurrence of cystoceles and rectoceles. Sand Peter K. et al, AJOG 2001; 184: 1357 -64 Objective: evaluate efficacy of polyglactin 910 mesh in preventing recurrent cystoceles and rectoceles Study design: prospective randomized controlled trial in 161 patients having cystoceles upto and beyond the hymenal ring and treated with CA with or without polyglactin mesh Results: • after 1 year • 30/70 (43%) without mesh and • 18/73 (25%) with mesh had recurrent cystoceles grade 1 (P=0, 02) • 8/70 (11%) without vs • 2/73 (3%) with mesh recurrent cystoceles grade 2 (P=0, 04) Conclusions: polyglactin 910 mesh significantly reduces recurrence of cystoceles after one year.
Porcine dermis xenograft as reinforcement for cystocoele stage 3 repair: a prospective randomized controlled trial De Ridder Dirk et al, abstract in Neurourology and urodynamics 2004 Objective: evaluate the potential advantages of biomaterials in cystocoele correction Study design: 134 patients were randomly assigned to Raz 4 point defect repair (sling) with a mesh of porcine dermis (Pelvicol) or with a mesh of polyglactin 910 (Vicryl). Primary endpoint was recurrence of cystocoele grade 2 or more at 24 months Results: cumulative recurrence rate at 24 months rate in the Pelvicol group was 9, 5% vs 30, 6% in the Vicryl group Conclusion: the use of porcine dermis xenograft results in a significant decrease of cystocoele recurrence using the Raz 4 -defect repair at 2 years FU compared to polyglactin mesh
Long-term anatomical and fuctional assessment of transvaginal cystocele repair using a tension-free polypropylene mesh de Tayrac Renaud et al, Int Urogynecol J 2006; 17: 483 -488 Objective: to report on the results of cystocele repair using a non-resorbable mesh Study-design: descriptive case series on 63 women undergoing cystocele-repair for cystocele grade 2 -4 using a polypropylene mesh (Gynemesh, Gynecare, Ethicon, France) in a tension-free way. Primary endpoint was anatomical result, secondary endpoints were functional result, sexual function and complications. Results: • mean follow-up of 37 months • 89, 1% anatomically cured (<stage 2) • 10, 9% recurrence: 9, 1% stage 1 cystocele 1, 8% stage 2 cystocele • 96, 4% significant improvement in quality of life • 16, 7% dyspareunia • 9, 1% erosion/granuloma formation
Prolift-mesh for pelvic organ prolapse surgical treatment: a retrospective study on 687 patients Cosson Michel et al, abstract in Neurourology and urodynamics 2005 Objective: to report on the results of prolapse repair using a non-resorbable mesh Study-design: descriptive case series on 687 women undergoing prolapse-repair using a polypropylene mesh (Prolift, Gynecare, Ethicon, France). Results: • evaluation at mean of 3, 6 months • 50, 3% had simultaneous hysterectomy • 5, 3% recurrence • 5, 4% de novo SI • 6, 7% erosion/granuloma formation • no information on dyspareunia Conclusion: short-term outcome rather disappointing with 5, 3% recurrence and 6, 7% erosion/granuloma formation at 3, 6 months
Conclusies • kiné of wijziging van levenspatroon geen nut in behandeling van prolaps • pessarium enkel diagnostisch en symptomatisch te gebruiken • aantal recidieven na cystocoelecorrectie is hoog bij alle gebruikte technieken • gebruik van meshes kan het aantal recidieven wellicht verminderen (<10%? ), echter bij gebruik van synthetische meshes is het aantal complicaties voorlopig nog steeds te hoog • « It is probably true that every honest surgeon of extensive and long experience will have to admit that he is not entirely satisfied with his long-term results of his operations for prolapse and allied conditions » Te Linde 1966