Prevention of OHSS Modern Techniques Shahar Kol IVF



, all had their embryos frozen")





 colloid fluids … at the time of")


 15, 000 IU u-h. CG")



















 20 15 10 5")
 50")

 Kol et al, RBMOnline 31: 633, 2015 37")


- Slides: 40
Prevention of OHSS: Modern Techniques Shahar Kol, IVF Unit Elisha hospital, Haifa, Israel Dead Sea, Jordan, May 2019
Content ● ● ● Scope of the problem Preventive strategies What really works Physiology of the agonist trigger Mechanism of luteolysis Side benefits
Severe OHSS: is it still a problem? Maternal deaths and rates per 100, 000 ART procedures, including IVF: United Kingdom: 1997– 2005 Number Rate 95% CI Number of treatment cycles 1997– 1999 20 19. 17 12. 41– 29. 61 104, 320 2000– 2002 8 7. 32 3. 71– 14. 44 109, 308 2003– 2005 12 10. 08 5. 76– 17. 61 119, 080 Deaths Year * Source Human Fertilisation and Embryology Authority • “In 2003– 2005, 4 deaths (of the 12) were due to OHSS” • ~3 OHSS-related deaths per 100, 000 ART cycles
Three OHSS-related deaths (3: 100, 000), all had their embryos frozen
Incidence and prediction of OHSS in women undergoing Gn. RH antagonist IVF cycles ● 2524 antagonist-based cycles (1801 patients) ● 53 patients (2%) were hospitalized because of OHSS – Conclusions: clinically significant OHSS is a limitation even in antagonist cycles “There is more than ever an urgent need for alternative final oocyte maturation – triggering medication”
Predictions: Severe OHSS “Severe OHSS will remain a complication of IVF cycles despite all attempts of prevention. ” R. G. Forman, 1999. “…None of the strategies currently employed to avert severe OHSS …completely prevents the condition”. P. E. Egbase, 2000.
Past predictions of the future • “We don’t like their sound, and guitar music is on the way out” Decca Recordings Co. rejecting the Beatles, 1962. • “Stocks have reached what looks like a permanently high plateau”. Irving Fisher, Professor of Economics. Yale University, 1929. • “$100 million is way too much to pay for Microsoft” IBM 1982. • “Who the hell wants to hear actors talks? ” H. M. Warner, Warner Brothers, 1927.
Preventive strategies: coasting ● There was no evidence to suggest any benefit of withholding gonadotrophins (coasting) after ovulation in IVF for the prevention of OHSS
Preventive strategies: cryopreservation ● There is not enough evidence to show whether using frozen embryos …can reduce OHSS in women who are at high risk
Preventive strategies: intravenous albumin ● Intravenous (iv) colloid fluids … at the time of oocyte retrieval may be beneficial for women with a high risk of developing OHSS ● Borderline evidence of benefit with the routine use of human albumin in the prevention of OHSS (1660 patients) ● Good evidence to support the use of hydroxyethyl starch in the prevention of OHSS (487 patients)
IV albumin for the prevention of severe OHSS: a systemic review and meta-analysis ● 1199 patients ● IV albumin does not appear to reduce the occurrence of severe OHSS
Preventive strategies: recombinant LH
Treatment arm Parameters examined 5000 IU rh. LH (n=39) 15, 000 IU u-h. CG (n=34) 30, 000 IU 15, 000 + 10, 000 IU rh. LH (n=39) u-h. CG (n=41) rh. LH (n=26) u-h. CG (n=22) rh. LH (n=25) u-h. CG (n=24) 15. 17 ± 8. 34 15. 46 ± 6. 75 14. 23 ± 5. 61 14. 00 ± 4. 90 a a 0. 3007 11. 84 ± 7. 53 11. 78 ± 6. 75 12. 62 ± 6. 22 10. 82 ± 5. 70 a a 0. 1702 a a 0. 183 p (linearity) No. of follicles >10 mm 14. 03 ± 5. 32 16. 44 ± 6. 95 No. of oocytes retrieved 10. 23 ± 4. 70 11. 74 ± 6. 27 Oocytes in metaphase II 85. 5% 77. 8% No. of oocytes inseminated 9. 82 ± 4. 74 11. 26 ± 5. 73 11. 63 ± 7. 52 11. 57 ± 6. 57 12. 38 ± 6. 25 10. 55 ± 5. 74 a a 0. 1687 No. of embryos 5. 42 ± 3. 33 7. 00 ± 4. 68 6. 65 ± 5. 02 6. 36 ± 4. 68 7. 67 ± 4. 34 6. 33 ± 5. 19 a a 0. 0983 No. of embryos transferred 2. 39 ± 0. 60 2. 48 ± 0. 85 2. 58 ± 0. 6 2. 52 ± 0. 62 2. 78 ± 0. 8 2. 67 ± 0. 73 a a 0. 4310 Implantation rate 6. 0 ± 0. 16% 15. 0 ± 0. 31% 6. 0 ± 0. 19% 9. 0 ± 0. 24% 11. 0 ± 0. 26% 3. 0 ± 0. 09% 19. 0 ± 0. 33% 17. 0 ± 0. 33% 0. 1373 Pregnancy (total) 15. 4% (n=6) 26. 5% (n=9) 10. 3% (n=4) 24. 4% (n=10) 23. 1% (n=6) 13. 6% (n=3) 32. 0% (n=8) 37. 5% (n=9) 0. 2689 Clinical pregnancy 10. 3% (n=4) 23. 5% (n=8) 7. 7% (n=3) 14. 6% (n=6) 15. 4% (n=4) 13. 6% (n=3) 28. 0% (n=7) 25. 0% (n=6) 0. 1479 Live birth 5. 1% (n=2) 17. 6% (n=6) 7. 7% (n=3) 12. 2% (n=5) 15. 4% (n=4) 4. 5% (n=1) 20. 0% (n=5) 16. 7% (n=4) 0. 0606 Cryopreserved embryos 4. 42 ± 2. 65 6. 81 ± 3. 67 7. 93 ± 4. 18 4. 90 ± 3. 24 6. 27 ± 2. 96 4. 80 ± 3. 19 5. 75 ± 2. 49 9. 89 ± 3. 22 0. 2645 Cryopreserved embryos transferred 3. 42 ± 1. 83 5. 67 ± 2. 65 3. 50 ± 1. 84 3. 27 ± 1. 49 3. 00 ± 1. 41 2. 17 ± 0. 98 2. 50 ± 0. 71 4. 75 ± 2. 43 0. 9092 Pregnancy from cryopreserved embryos (total) 16. 7% (n=2/12) 0. 0% (n=0/9) 50. 0% (n=5/10) 27. 3% (n=3/11) 62. 5% (n=5/8) 33. 3% (n=2/6) 0. 0% (n=0/2) 0. 0% (n=0/8) b Clinical pregnancy from cryopreserved embryos 8. 3% (n=1/12) 0. 0% (n=0/9) 40. 0% (n=4/10) 27. 3% (n=3/11) 50. 0% (n=4/8) 16. 7% (n=1/6) 0. 0% (n=0/2) 0. 0% (n=0/8) b Live birth from cryopreserved embryos 8. 3% (n=1/12) 0. 0% (n=0/9) 30. 0% (n=3/10) 18. 2% (n=2/11) 12. 5% (n=1/8) 0. 0% (n=0/6) 0. 0% (n=0/2) 0. 0% (n=0/8) b a. The IVF data of days u-h. CG/rh. LH 0– 4 of patients from group 15, 000 90. 8% 88. 6% 57. 6% 84. 5% + 10, 000 IU were pooled with those from group 15, 000 IU b. Because the numbers were small, no statistical comparison was performed on these data ● 15, 000 + 10, 000 IU gave 20% live birth rate but with a 12% OHSS rate
Preventive strategies: lowering h. CG dose ● Reducing the dose of h. CG does not eliminate the risk of OHS a high-risk group
Preventive strategies: dopamine agonists OHSS incidence D agonist=7 events control=13 events OHSS severity D agonist=20 events control=43 events
What really works: ● Gn. RH agonist versus h. CG for oocyte triggering in Gn. RH antagonist ART cycles Gn. RH a =0 events h. CG=21 events
Ovulation trigger RCT, high risk Oocyte source Own Engamnn, et al 2008 RCT, high risk Own Gn. RHa h. CG Acevedo, et al 2006 RCT Donors Gn. RHa h. CG Bodri, et al 2009 Retrospective Donors Gn. RHa h. CG Griesinger, et al 2010 Observational, High risk RCT Own Gn. RHa Own Retrospective, case- Own controlled, high risk Reference Trial type Babayof, et al 2006 • 16 publications • Agonist: 2005 patients, not a single Humaidan, et al 2009 case of OHSS! Engmann, et al 2006 • h. CG: 92 cases in 1810 patients, 5. 1% Manzanares, et al 2009 Retrospective case- Own control, high risk n OHSS % (n) 15 13 33 32 30 30 1046 1031 0 (0/13) 31(4/13) 0 (0/33) 31 (10/32) 0 (0/30) 17 (5/30) 0 (0/1046) 1. 3 (13/1031) 40 0 (0/40) Gn. RHa h. CG 152 150 0 (0/152) 2 (3/150) Gn. RHa h. CG 23 23 0 (0/23) 4 (1/23) 42 0 (0/42) 254 175 82 69 0 (0/254) 6 (10/175) 0 (0/82) 7 (5/69) 32 42 0 (0/32) 1 (1/42) 44 44 0 (0/44) 7 (3/44) 12 8 (1/12) 106 50 50 4 45 0 (0/106) 8 (9/106) 0 (0/50) 16(8/50) 0 (0/45) 15 (33) Gn. RHa h. CG - cancelled Hernandez, et al 2009 Retrospective Donors Gn. RHa h. CG Orvieto, et al 2006 Retrospective, high risk: agonist arm only RCT Own Gn. RHa h. CG Donors Gn. RHa h. CG Shapiro, et al 2007 Sismanoglu, et al 2009 Gn. RH, luteal rescue with h. CG 1500 IU Gn. RHa h. CG Humaidan, et al 2009 Observational, high Own risk Galindo, et al 2009 RCT Donors Melo, et al 2009 RCT Donors Gn. RHa h. CG Shahrokh, et al 2010 RCT, high risk Own Gn. RHa h. CG
Induction of preovulatory luteinizing hormone surge and prevention of ovarian hyperstimulation syndrome by gonadotropin-releasing hormone agonist. “A bolus of Gn. RH-a is able to trigger an adequate midcycle LH/FSH surge…and may prevent the clinical manifestation of ovarian hyperstimulation syndrome” Itskovitz et al, Fertil Steril. 1991 , 56: 213 -20.
Use of a single bolus of Gn. RH agonist triptorelin to trigger ovulation after Gn. RH antagonist ganirelix treatment in women undergoing ovarian stimulation for assisted reproduction, with special reference to the prevention of ovarian hyperstimulation syndrome: preliminary report: Short communication J. Itskovitz-Eldor et al HR, 2000 20
Treatment scheme for high responders Day 2 -3 menses Day 6 r. FSH High responder triptorelin 0. 2 mg Rec FSH OPU ganirelix ET Progesterone 21
Stimulation characteristics of 8 women with increased risk for developing OHSS and who received 0. 2 mg triptorelin for triggering ovulation Sub. r. FSH (IU) Foll 11 mm E 2 pg/ml Oocytes %MII 7 1350 33 39 22 2980 29 100 1500 21 3660 14 100 1950 24 3350 30 90 108 a 1875 22 6410 1 100 109 1275 28 7670 52 54 112 1575 34 4050 30 93 126 2175 22 3690 15 67 158 1575 28 3020 16 56 No OHSS !!! 22
A safe and OHSS-free clinical environment 23
“The concept of an OHSS-Free Clinic has become a reality. This approach should include pituitary down-regulation using a Gn. RH antagonist, ovulation triggering with a Gn. RH agonist and vitrification of oocytes or embryos” “…luteal phase supplementation with low-dose h. CG has to be fine tuned. ” Hum Reprod. 2011; 26: 2593
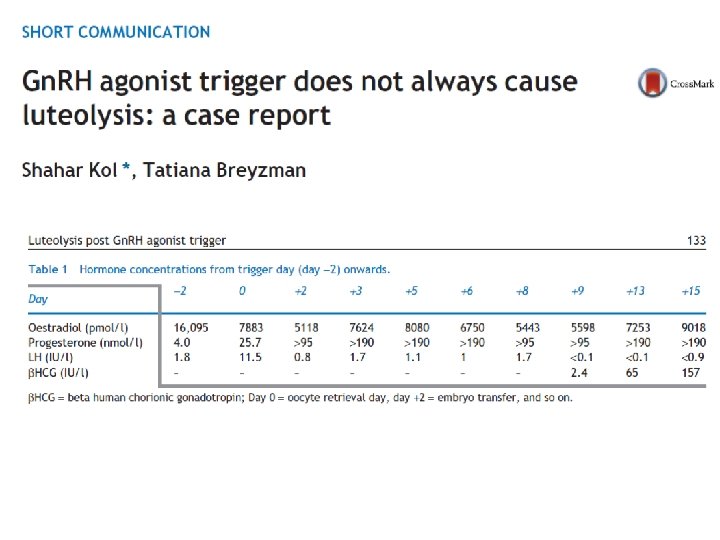
Failures? Very rarely luteolysis is not achieved. Fertil Steril. 101: 1008 -11, 2014
The physiology of agonist trigger LH surge 1 FSH surge 2
What happens after agonist trigger? Complete luteolysis! Luteal phase Natural cycle Day 7– 9 = 75 pg/m. L vs 18 Natural cycle Day 7– 9 = 750 pg/m. L vs 84 Nevo et al, F&S 2003; 79: 1123 -8.
Complete luteolysis ü Great for OHSS prevention. ü For fresh transfer we need to provide enough P 4 and E 2 to the system. ü How? ü …But first, let us consider the mechanism of luteolysis post Gn. RH agonist trigger.
The mechanism of luteolysis post agonist trigger? ü…. Surprise… not known…although used for many years üHypothesis: Loss of LH pulsatility? üStudy: 10 IVF hyper-responder patients, who received Gn. RHa as trigger, with no further support üRepeated blood sampling, every 20 minutes üFive patients on the day of oocyte retrieval üFive patients 48 hours later, on embryo transfer day. 29
2017 ; 33: 741 -745. 30
Natural cycle luteal LH Filicori et al JCI 73: 1638, 1984 31
32
Natural cycle LH change in the day of embryo transfer Post agonist trigger Mean LH 21. 5 0. 6 Pulse number 2 -3 1. 2 3 Pulse amplitude 12. 3 0. 44 2. 5 LH (U/l) 2 1. 5 1 0. 5 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 Patient 6 0. 830. 650. 570. 710. 510. 620. 420. 380. 34 0. 3 0. 240. 230. 210. 180. 171. 26 Patient 7 2. 172. 580. 921. 15 1. 040. 951. 010. 780. 660. 750. 720. 610. 650. 620. 851. 12 Patient 8 1. 321. 381. 070. 920. 770. 660. 530. 42 0. 5 0. 370. 36 0. 3 1. 151. 011. 21 0. 9 0. 72 Patient 9 0. 73 0. 6 0. 52 0. 5 0. 660. 570. 510. 410. 340. 310. 340. 410. 450. 370. 310. 280. 78 Patient 10 0. 870. 460. 47 0. 5 0. 410. 350. 280. 250. 230. 210. 190. 170. 16 0. 5 0. 450. 350. 29 Time points Tannus et al, Gyn Endocrinol 33: 741, 2017 Patient 6 Patient 7 Patient 8 Patient 9 Patient 10 33
Very early luteal phase: Gradual P increase 25 P (nmol/l) 20 15 10 5 0 20 40 60 80 100 120 140 160 180 200 220 240 260 280 300 320 340 Time (minutes) Plasma P levels (mean ± SEM) in the day of oocyte retrieval. There is a significant increase in P values over time. R=0. 53, P= 0. 023 Tannus et al, Gyn Endocrinol 33: 741, 2017 34
Day 2 post OPU: peak P, and decline 65 60 55 P (nmol/l) 50 45 40 35 30 25 20 0 20 40 60 80 100 120 140 160 180 200 220 240 260 280 300 320 340 Time (minutes) Plasma P throughout the study in the day of embryo transfer, 48 hrs post OPU (Mean ± SEM). There is a significant constant decline in P values over time. R= -0. 94, P<0. 00001 Tannus et al, Gyn Endocrinol 33: 741, 2017 35
Conclusions ü Mean LH concentrations and LH pulse amplitude are lower than those described for a natural cycle. ü The process of luteolysis starts 48 hrs after oocyte retrieval. Tannus et al, Gyn Endocrinol 33: 741, 2017 36
Luteolysis kinetics (P) Kol et al, RBMOnline 31: 633, 2015 37
Side benefits ● Agonist trigger: more MII oocytes compared with h. CG trigger 1 -4 ● Potential benefit of FSH surge: 5 -9 – Promotes LH receptor formation in luteinizing granulosa cells – Promotes nuclear maturation (i. e. resumption of meiosis) – Promotes cumulus expansion
Crystal ball: where are we heading? In Out Antagonist-based protocols ‘Long agonist’ protocols Agonist trigger h. CG trigger LH activity-based luteal support Progesterone-based luteal support Total OHSS elimination 1– 2% severe OHSS Total OHSS elimination OHSS-related death rate: 3: 100, 000 Patient-friendly luteal phase Painful P injections or leaky, messy vaginal P