Prevention diagnosis and treatment of key Opportunistic Infections



























 • Most common bacterial OI in the developed world •")






")

- Slides: 37
Prevention, diagnosis, and treatment of key Opportunistic Infections in HIV Infection Theodoros Kelesidis UCLA CARE Center
The Late Phase of HIV-1 1400 Plasma viral titer by PCR or b. DNA assay Plasma viral titer by culture or p 24 antigen + Number of CD 4 cells 106 1200 104 800 103 600 102 400 101 200 1 2 9 CD 4+ Count Plasma Viremia 105 10 Time (Years) PCR=polymerase chain reaction; b. DNA=branched DNA. Adapted with permission from Saag. In: De. Vita et al, eds. AIDS: Etiology, Treatment and Prevention. 4 th ed. Lippincott-Raven Publishers; 1997: 203 -213.
Risk of Death Associated with ADEs Adjusted Hazard Ratio Herpes simplex 0. 97 Mycobacterial disease 5. 07 Toxoplasmosis 5. 10 Cryptococcosis 9. 00 PML 9. 56 Non-Hodgkin’s lymphoma 19. 31 Mocroft A, and ART Cohort Collaboration CROI 2007# 80.
33 YO with chest pain, fever and productive cough worsening over 3 d
Candidiasis • Oropharyngeal candidiasis is the most common opportunistic infection in persons infected with HIV • is usually associated with significant immunosuppression (CD 4 counts <200 cells/micro. L) • Topical therapy for the initial episode of oropharyngeal candidiasis in HIVinfected patients with mild disease. • For patients with recurrent infection, moderate to severe disease, or in those with advanced immunosuppression (CD 4 <100 cells/micro. L) (200 mg loading dose, followed by 100 to 200 mg daily for 7
37 YO HIV + male CD 4 76 as of six months ago, now has DOE, fever, dry cough, and pleuritic chest pain. His symptoms have been progressing over the last month despite 10 days of Levaquin. 38 C 120/70, HR 120, pulse ox is 69% on room air. Ill appearing, in mild respiratory distress
Pneumocystis • We now refer to the organism that causes human disease as pneumocystis jirovecii • In ‘ 80’s AIDS defining illness for 2/3 rds of patients • Ugandan study found 38. 6% of 83 pts admitted with pneumonia had PCP on BAL • Presentation: – Gradual onset dyspnea, fever, nonproductive cough, unremarkable lung exam, tachycardia – CXR: Diffuse bilateral interstitial infiltrates, is a leading cause of pneumothorax.
Diagnosis of PCP • hypoxemia, elevated LDH nonspecific • induced sputum • BAL • Specific dx should be sought in those with mod-severe disease
Treatment • TMP/SMZ treatment of choice • Steroids ASAP but at least within 72 hours if p. O 2<70 or Aa gradient >35 mm/Hg • Pentamidine is second choice for moderate to severe disease • Discontinue prophylaxis in patients who have responded to ARVs with a CD 4 cell >200 sustained for longer than 3
39 yo engineer from Belize with right sided weakness, tremor, expressive aphasia, and generalized seizure. Found to be HIV positive, CD 4= 32. No history of IVDU.
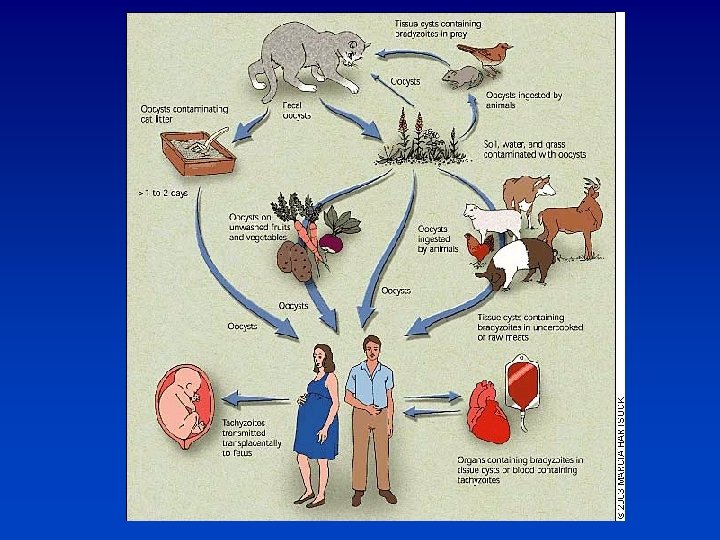
Toxoplasmosis • Most common cause of intracerebral lesions in persons with HIV. • 15 -30% of US population is seropositive • 50 -75% in some European countries. • Without prophylaxis 30% of seropositive with CD 4<50 will
Toxoplasmosis • Presentation: headache, fever, confusion, focal deficits, and seizures • Differential: CNS lymphoma, abscess, cryptococcoma, tuberculoma
DIAGNOSIS – CT or MRI with contrast are not specific, – Serum and CSF Ig. G/Ig. M – CSF PCR is specific 96 -100%, but sensitivity 50%
Toxoplasmosis-Treatment • Pyr + sulfadiazine + leucovorin • Preferred alternative Pyr+ clinda + leucovorin • TMP-SMX which is inexpensive and readily available in developing countries may be suitable first line therapy for acute TE
Toxoplasmosis treatment • Acute therapy for 6 weeks, until resolution of contrast enhancement • Adjunctive steroids for mass effect and edema • Chronic Maintenance therapy until CD 4>200 x 6 months – Sulfadiazine 2 -4 gm + Pyr 25 -50 +leucovorin 10 -25
Primary Prophylaxis • CD 4<100 and Toxoplasma Ig. G + • Discontinue ppx when CD 4>200 > 3 months • TMP-SMZ SS or DS qd • Alternatives – Dapsone + Pyrimethamine q week + Folinic acid q week – Mepron +/_ Pyrimethamine – ? Azithromycin
l 28 YO M, HIV status unknown, brought in by his wife with headache, vomiting and confusion worsening over 9 days. l 39. 4 C, combative, without obvious focal findings. l CT with contrast increased intracranial pressure.
Likely diagnoses include? a. Cryptococcal meningitis b. Tuberculous meningitis c. Cocci meningitis d. Lymphomatous meningitis e. Bacterial meningitis
Cryptococcosis • Pre. HAART occurred in 6 -10% of persons with AIDS in US, Europe & Australia • 7/1000 AIDS pts in 2000 in US • Cause of 20 -45% of cases of community acquired meningitis in South Africa, moving ahead of tuberculous meningitis
Cryptococcosis • Meningitis or meningoencephalitis is the most common manifestation • Presents with progressive headache, fever, AMS worsening over several weeks may have symptoms of increased ICP. • Meningismus, papillaedema, cranial nerve palsies not uncommon
Diagnosis • High organism load in HIV, so India ink usually positive in AIDS, (sensitivity 7585%) • Cryptococcal antigen high sensitivity 95% and specificity for diagnosis but little utility in assessing response to therapy • 75% with meningitis also have + blood cultures • opening pressure >200 mm Hg in 75% • CSF lymphocytic pleocytosis • elevated protein, low glucose
Use of Lumbar punctures • CT first, always check the opening pressure with each LP • Repeat LP for signs of increased ICP (HA, AMS, visual or hearing loss), may require lumbar drain • Daily LPs to achieve a closing pressure <20 or 50% of the opening pressure • If not improving or new symptoms repeat LP
Treatment Guidelines • Preferred induction regimen: 2 weeks of – Am. B + flucytosine – Consolidation if CSF culture neg – Fluconazole 400 mg/day x 8 weeks • Maintenance – Fluconazole 200 qd until CD 4>200 x 6 months • Combination fluconazole and 5 -FC, in small studies had response rates of 60– 80%, comparable to amp. Bbased regimens
SM • 59 YO Lebanese male admitted 9/30 with new onset seizures • PMH – pancytopenia with negative work up – PE word finding difficulty, flattening of R nasolabial fold • R hand decreased grip strength, decreased strength biceps • CT showed L frontal enhancing lesion with mass effect and a small R cerebellar enhancing lesion • CT of chest and abdomen showed 2. 3 x 1. 8 cm mass at the root of the mesentary along the superior
What tests do you want? • • HIV 1/2 serology Toxoplasma serology ppd Blood cultures
Mycobacterium avium complex (MAC) • Most common bacterial OI in the developed world • 10 -20% of persons with AIDS • independent predictor of mortality • Acquired through inhalation or ingestion, spreads through lymphatics • Fevers, night sweats, weight loss,
Prophylaxis and treatment • Prophylaxis: Start CD 4<50 Stop CD 4>100 x 3 months • Azithromycin 1200 q week • Combination therapy is essential resistance seen in 46% after 16 weeks on Clarithromycin alone • Clarithromycin + Ethambutol +/- Rifabutin or • 12 months of treatment and • CD 4>100 x more than 6 months
Fever in patient with CD 4<50 • 34 YO with fever to 102, weight loss, heartburn and diarrhea, no cough, no visual changes, no headache, no marked adenopathy. • Labs: Hct 29, LDH 255, LFTS normal • stool studies show a few red blood cells • Chest x-ray unremarkable
Fever in patient with CD 4<50 Mycobacterium avium complex Cytomegalovirus Cryptococcus M. tuberculosis Lymphoma Endemic mycoses
Epidemiology-CMV • Developed world 40 -70% healthy adults infected. • In persons with HIV especially IVDU and MSM, close to 100% are also seropositive for CMV • Autopsy studies show up to 90% of persons dying with HIV in pre. HAART era had CMV disease • 40% developed sight threatening disease after CD 4 dropped to <50
Cytomegalovirus Reactivation when CD 4<100 • 85% retinitis • 17% GI tract esophagitis, gastritis, duodenitis, colitis • 1% encephalitis, polyneuritis, polyradiculopathy • ? % pneumonitis
CMV Treatment • Ganciclovir- IV, PO or intravitreal • Foscarnet- IV, intravitreal • Cidofovir- IV • +/-Prophylaxis if CD 4<50 • Preemptive therapy for viremia? • Treatment of symptomatic disease with induction followed by maintenance therapy • In the absence of immune reconstitution drug resistance emerges with serial accumulation of
Summary of prophylaxis Infection Preferred drug Indications Pneumocystis carinii pneumonia Trimethoprimsulfamethoxazole (double-strength tablet daily) CD 4 count <200 cells/micro. L; thrush; unexplained fever for more than two weeks; history of PCP Toxoplasmosis Trimethoprimsulfamethoxazole (double-strength tablet daily) CD 4 count <100 cells/micro. L and Toxoplasma seropositive Mycobacterium avium complex Azithromycin (1200 CD 4 count <50 mg weekly) cells/micro. L
Take home messages • OIs are the most common presentations of AIDS/HIV • Usually occur when CD 4 < 200 • Most important: PCP, MAC, Cryptococcus, Toxoplasma, CMV • Candida infection is the most common OI and MAC is the most common bacterial OI • Life Threatening: PCP, Cryptococcus • Prophylaxis if CD 4 <200: bactrim,