Prevention and Treatment of Sepsis induced AKI Joseph

 I hold a US patent on use of Type IV PDEI")












 0– 6 6– 72 0– 72")
 Intervention (n =")

 Basal Day 1 Day 2 Day 3 Day 4 NE-group")
, and biomarkers of acute")










")
 Canadian Trial group")
















- Slides: 55
Prevention and Treatment of Sepsis induced AKI Joseph A Carcillo Center for Critical Care Nephrology at Children’s Hospital of Pittsburgh and University of Pittsburgh
My Disclosures A) I hold a US patent on use of Type IV PDEI to prevent and treat sepsis induced renal injury B) I am the taskforce chair of the ACCM guidelines for hemodynamic support of newborn and pediatric septic shock C) I am a member of the Center of Critical Care Nephrology at the University of Pittsburgh
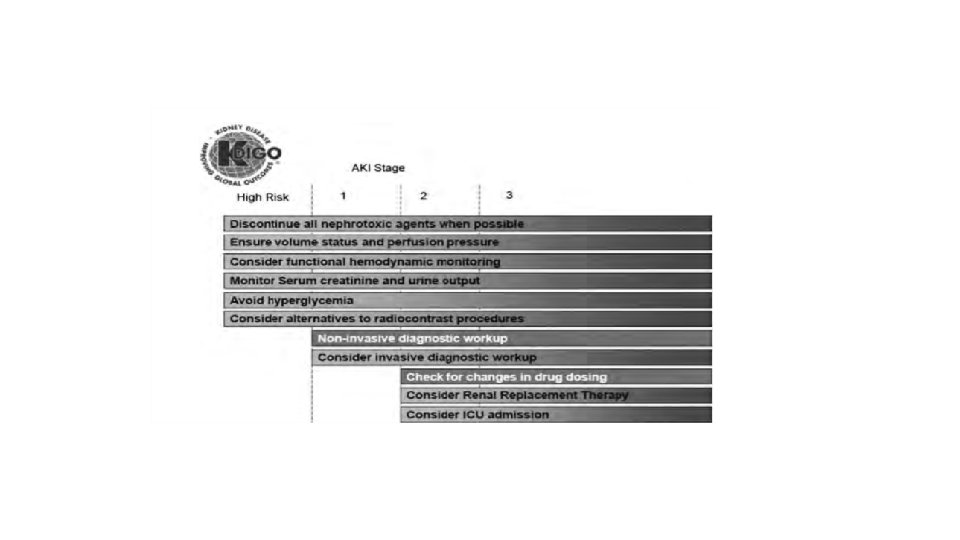
Role for the Intensivist to prevent kidney injury When do you get consulted? EGDT Normal Increased risk Optimize RRT Defend Blood Pressure Restore & Optimize Perfusion Use inotropes with care Mitigate Inflammatory Injury Damage Timing, Dose Drug dosing GFR Kidney failure Antecedents Intermediate Stage AKI Outcomes Death
Plasma exchange
Rapid Resuscitation Reduces the Development of Sepsis induced AKI in Children
Five time points evaluated for adherence from 2006 PALS algorithm. Raina Paul et al. Pediatrics 2012; 130: e 273 -e 280 © 2012 by American Academy of Pediatrics
Table IV. Comparison of patient outcomes before and after institution of the Septic Shock Resuscitation Protocol in Emergency Department Table IV. Comparison of patient outcomes before and after institution of the SSP Variables PRE SSP POST SSP P value AKI 53 (54%) 30 (29%) Risk 32 20 Injury 16 7 Failure 5 3 Severe AKI 21 (21%) 10 (9. 6%) . 03 RRT 4 (4%) 0 . 037 LOS, hospital, d 15. 3 ± 16. 9 6. 3 ± 5. 1 <. 001 LOS, PICU, d 4. 5 ± 7. 6 1. 9 ± 2. 3 <. 001 Mortality, n (%) 10 (10) 3 (3) . 037 <. 001 Resuscitation Bundle in Pediatric Shock Decreases Acute Kidney Injury and Improves Outcomes
Balanced solution vs Normal Saline?
Figure 4. Hospital mortality for LR-any and NS groups matched within quartile of total crystalloid fluid volume. The x-axis categorizes patients based on quartile of total fluid crystalloid volume received after correcting by estimated weight for age (median total volume in Q 1 = 8 m. L/kg, Q 2 = 17 m. L/kg, Q 3 = 32 m. L/kg, and Q 4 = 68 m. L/kg). The y-axis shows the adjusted 30 -day mortality rate. Patients in the LR-any group were matched within volume quartile to patients who received only NS. There were no significant differences in mortality between the LR-any and NS groups within any of the total volume quartiles. Crystalloid Fluid Choice and Clinical Outcomes in Pediatric Sepsis: A Matched Retrospective Cohort Study. Weiss SL, Keele L, Balamuth F, Vendetti N, Ross R, Fitzgerald JC, Gerber JS. J Pediatr. 2017 Mar; 182: 304 -310. e 10. doi: 10. 1016/j. jpeds. 2016. 11. 075. Epub 2017 Jan 4.
Timely Antimicrobial Administration prevents of Sepsis induced AKI and Death
• Sean M. Bagshaw • Stephen Lapinsky • Sandra Dial • Yaseen Arabi • Peter Dodek • Gordon Wood • Paul Ellis • Jorge Guzman • John Marshall • Joseph E. Parrillo • Yoanna Skrobik • Anand Kumar Fig. 2 Cumulative effective antimicrobial therapy following onset of hypotension and associated incidence of AKI Intensive Care Medicine May 2009, Volume 35, Issue 5, pp 871– 881 Acute kidney injury in septic shock: clinical outcomes and impact of duration of hypotension prior to initiation of antimicrobial therapy
Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric Sepsis*. Weiss, Scott; Fitzgerald, Julie; MD, Ph. D; Balamuth, Fran; MD, Ph. D; Alpern, Elizabeth; MD, MSCE; Lavelle, Jane; Chilutti, Marianne; Grundmeier, Robert; Nadkarni, Vinay; MD, MS; Thomas, Neal; MD, MSc Critical Care Medicine. 42(11): 2409 -2417, November 2014. DOI: 10. 1097/CCM. 0000000509 Figure 1. Time from sepsis recognition to initial antimicrobial administration with survival fraction. Total number of patients at hourly intervals from sepsis recognition to administration of initial antimicrobial therapy. The shaded portion of each bar indicates the number of nonsurvivors in each time interval. Copyright © by 2014 by the Society of Critical Care Medicine and Wolters Kluwer Health, Inc. All Rights Reserved. Published by Lippincott Williams & Wilkins, Inc. 2
MAP-CVP and Sc. VO 2 targeted therapy decreases new AKI ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation (De Oliveira et al 2008 Intens Care Med)
ACCM/PALS haemodynamic support guidelines for paediatric septic shock: an outcomes comparison with and without monitoring central venous oxygen saturation (DE Oliveira et al 2008 Intens Care Med)
Fluids Hours after study entry Resuscitation fluids (ml/kg) 0– 6 6– 72 0– 72 Crystalloid Control group Intervention group 5 (0– 20) 28 (20– 40) 10 (0– 28) 0 (0– 20) 80 (45– 100) 90 (65– 114) p-value < 0. 0001 Red-cell transfusion (% of patients) Control group Intervention group 15. 7 45. 1 43. 1 31. 4 58. 8 68. 6 p-value< 0. 002 Addition of vasopressor (% of patients) Control group Intervention group 56. 9 49. 0 18. 4 23. 5 74. 6 72. 5 p-value = 0. 55 Addition of inotrope (% of patients) Control group Intervention group 7. 8 29. 4 22. 4 19. 6 29. 4 49. 0 p-value = 0. 07
Table 3 Organ dysfunction, morbidity and mortality Control (n = 51) Intervention (n = 51) pvalue Number of organ dysfunctions at admission 2. 0 (1. 0– 2. 0) 0. 97 c Organ (%) Respiratory Cardiovascular Renal Neurological Gastrointestinal Haematological Hepatological 47. 1 51. 0 11. 8 5. 9 0 25. 5 27. 4 43. 1 62. 7 11. 8 3. 9 0 25. 5 0. 84 a 0. 32 a 1. 00 a Number of new organ dysfunction during ICU stay Development of new organ dysfunction (%) 1. 0 (1. 0– 2. 0) Respiratory Cardiovascular Renal Neurological Gastrointestinal Haematological Hepatological 59. 3 92. 0 26. 7 10. 4 9. 8 31. 6 13. 5 1. 0 (0. 0– 2. 0) 48. 3 89. 5 6. 7 0 7. 8 15. 8 0. 03 0. 44 1. 00 0. 02 0. 03 1. 00 0. 18 1. 00 c a a a a
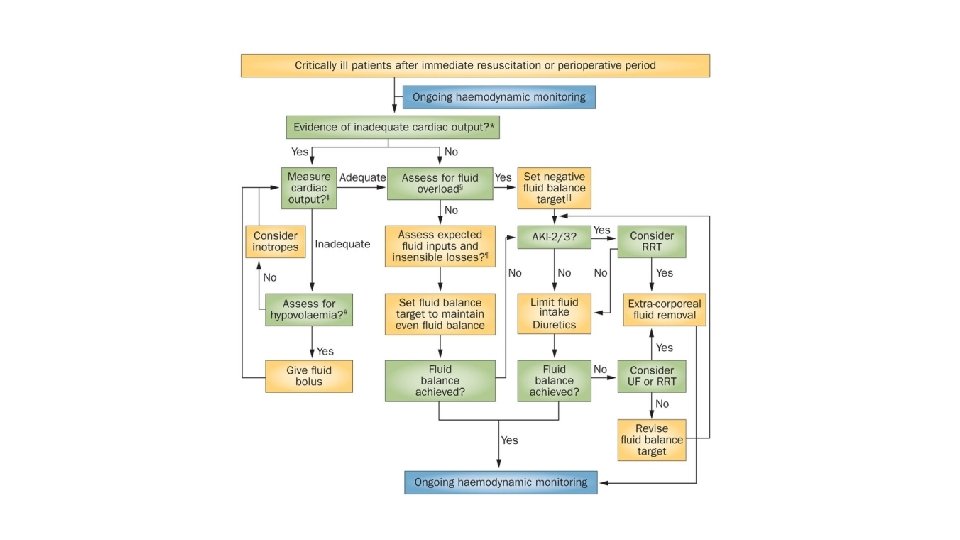
Managing fluid overload with norepinephrine, control of intraabdominal pressure, diuretics, and CRRT
Urine output (m. L/kg/hr) Basal Day 1 Day 2 Day 3 Day 4 NE-group 4. 3± 2. 9 4. 7± 1. 7 5. 1± 1. 7 4. 9± 1. 5 4. 5± 1. 2 Placebogroup 3. 5± 2. 2 3. 9± 1. 6 3. 8± 1. 0 4. 1± 1. 5 4. 5± 1. 5 * 0. 016 Jefferson Piva 1, Tamila Alquati 2, Pedro Celiny Garcia 23, Humberto Fiori 23, Paulo Einloft 23, Francisco Bruno 23 Norepinephrine infusion increases urine output in children under sedative and analgesic infusion. Rev. Assoc. Med. Bras. [online]. 2014, vol. 60, n. 3, pp. 208 -215. ISSN 0104 -4230.
Figure 1. Correlation between current renal function, intra-abdominal pressure (IAP), and biomarkers of acute kidney injury (AKI). Patient n° 1 (dashed line): in presence of effective myogenic response, an acute increase in IAP is associated to a slight decrease in renal function (tract 0–C). A further increase of IAP may lead to biomarkers increase (subclinical AKI, tract C–D). When IAP overcomes the intrarenal autoregulation, glomerular hypoperfusion occurs and a picture of clinical AKI becomes manifest (above point D). Patient n° 2 (solid line): in presence of compromised myogenic response, an acute increase in IAP is associated with a strong reduction in renal function until the development of clinical functional AKI (tract A–B). If IAP further increases, the inflammatory and ischemic insults may lead to the kidney parenchymal damage detectable by biomarkers (above point B). Front Physiol. 2016 Feb 23; 7: 55. doi: 10. 3389/fphys. 2016. 00055. e. Collection 2016. The Pathophysiological Hypothesis of Kidney Damage during Intra-Abdominal Hypertension. Villa G 1, Samoni S 2, De Rosa S 3, Ronco C 4.
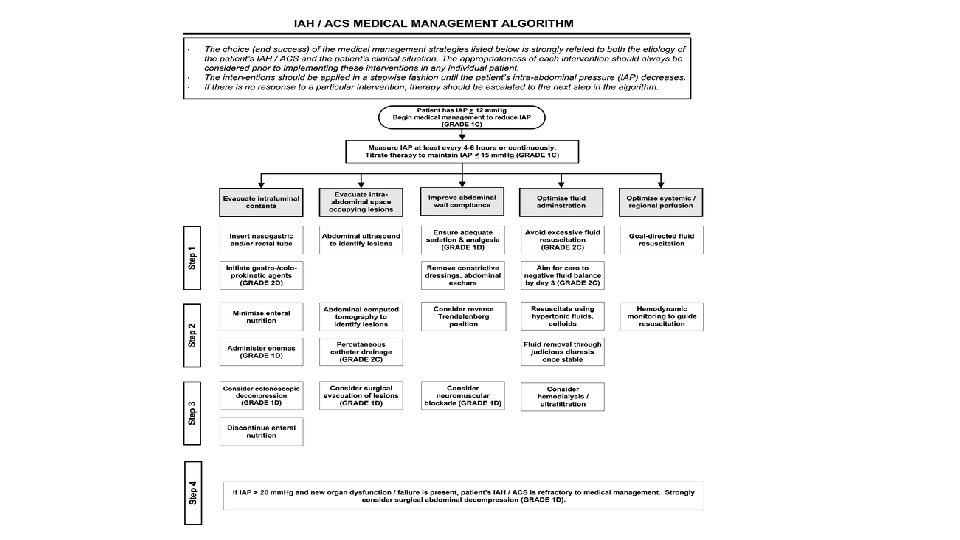
ADEQUATE PERFUSION PRESSURE SEQUENTIAL DIURETIC BLOCKADE Dopexamine MAP – CVP Amiloride Metalozone MAP– IAP Aminophylline 1 mg/kg q 6 hours Continuous Furosemide infusion 0. 04 -0. 16 mg /kg /h INCREASED DIURESIS Hydrochlorothiazide 5 -10 mg/kg q 12 hours
Recommendations • KDIGO Guidelines : Start CRRT at RIFLE injury/failure level • Weight gain at initiation of RRT has been associated with a poor outcome. • Awaiting further trials, the early use of CRRT is a reasonable yet not generally accepted approach to control fluid homeostasis
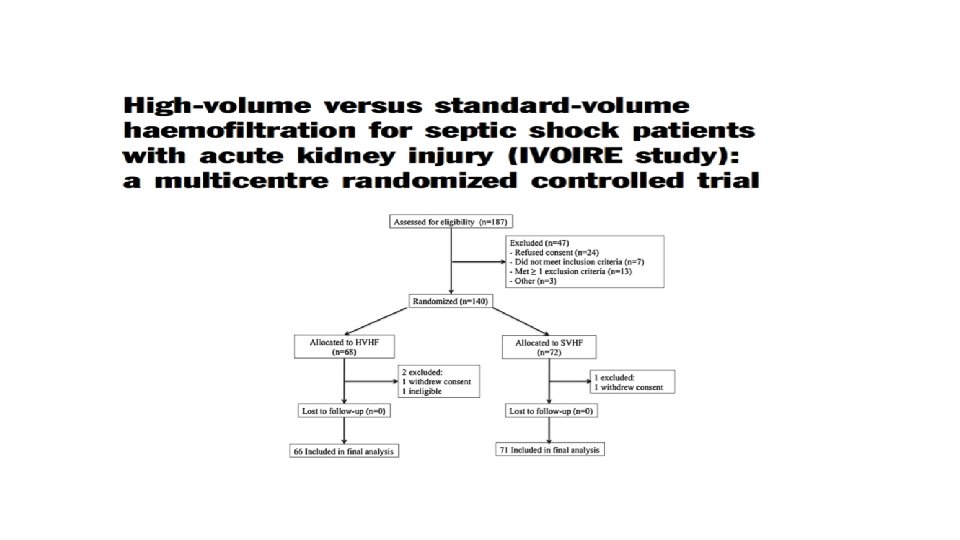
Is haemofiltration beneficial in sepsis? • Mortality benefit in sepsis ? • With or with kidney injury ? • What mechanism ? • Dialysis dose benefit ? Disease Sepsis Disease Modification OUTCOME Apoptosis Severity of illness AKI Cell death Haemofiltration Target /Goal Indication CVVH Timing CVVH Efficiency Complications
Cytokine Peak Concentration Hypothesis Just need to Balance the Cytokine scales Annu. Rev. Pathol. Mech. Dis. 2006. 1: 467– 96
Fluid overload before continuous hemofiltration and survival in critically ill children: A retrospective analysis *. Foland, Jason; Fortenberry, James; MD, FAAP; Warshaw, Barry; MD, FAAP; Pettignano, Robert; MD, FAAP; Merritt, Robert; Heard, Micheal; Rogers, Kris; Reid, Chris; Tanner, April; Easley, Kirk Critical Care Medicine. 32(8): 1771 -1776, August 2004. DOI: 10. 1097/01. CCM. 0000132897. 52737. 49 © 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
Fluid overload before continuous hemofiltration and survival in critically ill children: A retrospective analysis *. Foland, Jason; Fortenberry, James; MD, FAAP; Warshaw, Barry; MD, FAAP; Pettignano, Robert; MD, FAAP; Merritt, Robert; Heard, Micheal; Rogers, Kris; Reid, Chris; Tanner, April; Easley, Kirk Critical Care Medicine. 32(8): 1771 -1776, August 2004. DOI: 10. 1097/01. CCM. 0000132897. 52737. 49 © 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
Figure 1. Box plot of the median, the 25 th and 75 th percentiles, range, and individual data values for percent fluid overload by survival status for all patients, patients with multiple organ dysfunction syndrome (MODS), and patients with >=3 -organ MODS. The middle line within the box represents the median, the top line represents the 75 th percentile, and the bottom line represents the 25 th percentile. The bottom and top bars represent the 10 th and 90 th percentiles, respectively. *p =. 02; **p =. 01 compared with survivors for each group. Fluid overload before continuous hemofiltration and survival in critically ill children: A retrospective analysis *. Foland, Jason; Fortenberry, James; MD, FAAP; Warshaw, Barry; MD, FAAP; Pettignano, Robert; MD, FAAP; Merritt, Robert; Heard, Micheal; Rogers, Kris; Reid, Chris; Tanner, April; Easley, Kirk Critical Care Medicine. 32(8): 1771 -1776, August 2004. DOI: 10. 1097/01. CCM. 0000132897. 52737. 49 © 2004 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 2
• Median interval between the start of EGDT and commencement of CRRT - 26. 4 hours • 28 day mortality for all patients – 43. 3% • 28 - day all-cause mortality rate : Early CRRT – 7. 9 hours Late CRRT – 61. 5 hours Late CRRT 56. 7% Early CRRT 30. 0% Higher mortality risk in the late group remained significant even after adjusting for diabetes mellitus, liver failure, and APACHE II scores (hazard ratio, 2. 461) Early initiation of CRRT stratified by the interval between the time of EGDT enrollment and start of CRRT was an independent predictor of increased patient survival. J Crit Care. 2016 Oct; 35: 51 -6. doi: 10. 1016/j. jcrc. 2016. 04. 032. Epub 2016 May 4. Can early initiation of continuous renal replacement therapy improve patient survival with septic acute kidney injury when enrolled in early goal-directed therapy? Oh HJ 1, Kim MH 2, Ahn JY 2, Ku NS 3, Park JT 1, Han SH 2, Choi JY 2, Han SH 1, Yoo TH 1, Song YG 2, Kang SW 1, Kim JM 2.
CRRT in practice gets initiated : • • Fluid overload poorly tolerated Partly/un responsive to diuretics
Dose of CRRT • Ronco’s proposal – 35 mls/kg/hour – CVVH • RENAL and ATN Trials (NEJM) – No effect on dose – combination of IHD /CRRT, CVVH + CVVHD • Effect of dose on cytokine clearance and immunomodulatory effect • Effect on renal recovery?
Intensity of CRRT in Critically Ill Patients (The “RENAL” Study)
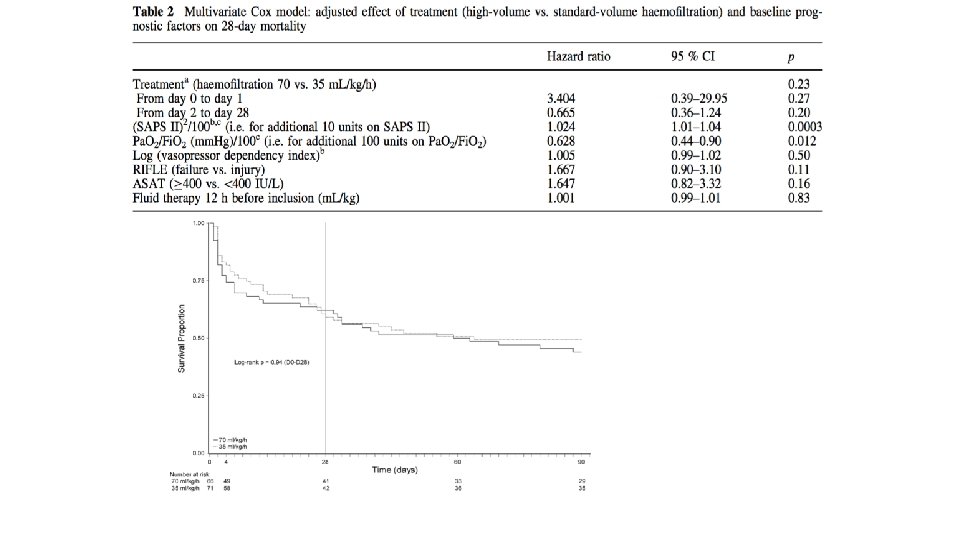
Mode dialysis in sepsis: CVVH vs CVVHD Acute Kidney Injury (OMAKI) Canadian Trial group CVVH vs CVVHD n=78 adults (80% sepsis) Same dialysis dose of 35 ml/kg/hr effluent rate No difference mortality CVVH 12/35 35% CVVHD 10/38 27% Wald et al. Critical Care 2012, 16: R 205
Endotoxin adsorption on haemofilter Kellum CCM 2004
Antibiotic dosing? • What happens in septic shock to : üProtein binding üVolume of distribution (Vd) üHigh volume CRRT – more clogging ----- less efficacious üAntibiotics üAntifungals üImportance of drug levels
Managing Thrombocytopenic AKI/MOF with plasma exchange
Plasma ADAMTS 13 levels in patients and healthy subjects. Tomoko Ono et al. Blood 2006; 107: 528 -534 © 2006 by American Society of Hematology
Correlation between the plasma ADAMTS 13 levels and the serum creatinine levels. 57% ADAMTS 13 Is considered normal s. CR > 1. 5 ADAMTS 13 > 57% Tomoko Ono et al. Blood 2006; 107: 528 -534 © 2006 by American Society of Hematology
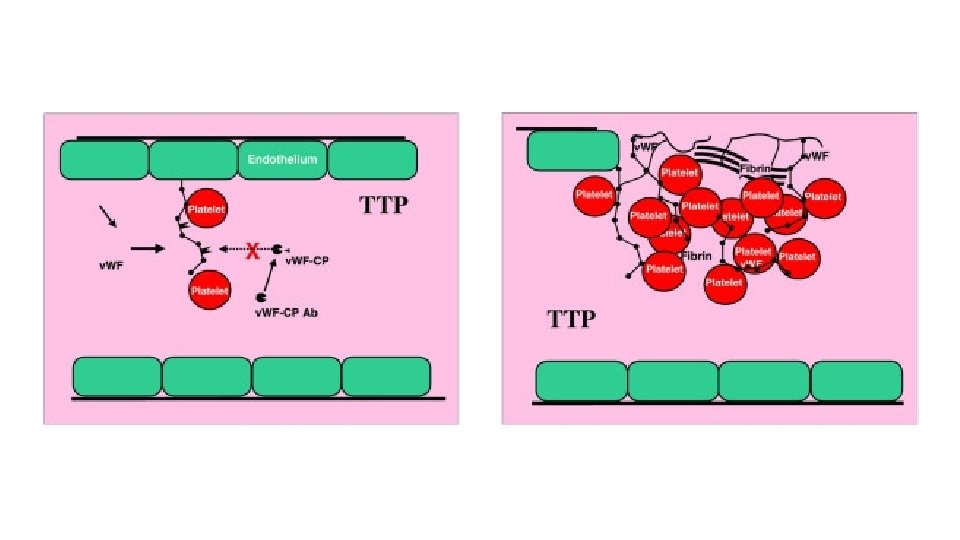
Platelet counts recovered in children with multiple organ failure who survived compared to those who did not survive. [1– 8] Von Willebrand Factor (VWF)-rich thrombi are seen in the small blood vessels of the brains, lungs, and kidneys of non-survivors with thrombocytopenia-associated multiple organ failure(A) Black circles represent platelet counts (mean +/− S. D. ) in children with multiple organ failure who survived (n = 30). White circles represent platelet counts in children who did not survive (n = 7). Patients who survived recovered their platelet counts compared to children who did not survive (2 Factor ANOVA p < 0. 05). (B). Brain (I, IV), kidney (II, V), and lung (III, VI) tissue from a representative patient stained for VWF (brown color) (polyclonal rabbit anti-human VWF antibody). Panels I, II, and III serve as negative controls from the same patients as in Panels IV, V, and VI respectively, labeled with isotype antibody (non-specific rabbit anti-human Ig. G). The secondary antibody was conjugated with horse radish peroxidase (brown color).
Plasma exchange replenishes ADAMTS 13, and reduces organ failure. Plasma exchange patients are represented by black circles (n = 5), and Standard therapy patients are represented by white circles (n = 5). (A) There was a robust reduction (p<0. 001 2 Factor Repeated Measures ANOVA group × time) over the 28 day study period in PELOD scores in patients randomized to the plasma exchange arm compared to those given standard therapies. (B) There was a significant increase in ADAMTS-13 activity with plasma exchange (44 ± 10% on day 1 increased to 56 ± 11. 5% on day 7; mean ± SEM) compared to standard therapy (25 ± 11% on day 1 decreased to 17 ± 11% on day 7; mean ± SEM) (p<0. 05, 2 Factor ANOVA group × time). Crit Care Med. Author manuscript; available in PMC 2009 Nov 3. Published in final edited form as: Crit Care Med. 2008 Oct; 36(10): 2878– 2887. PMCID: PMC 2772176 NIHMSID: NIHMS 98335 Intensive Plasma Exchange Increases ADAMTS-13 Activity And Reverses Organ Dysfunction In Children With Thrombocytopenia-Associated Multiple Organ Failure Trung C. Nguyen, 1 Yong Y. Han, 2 Joseph E. Kiss, 3, 4 Mark W. Hall, 5 Andrea C. Hassett, 4 Ron Jaffe, 6 Richard A. Orr, 7 Janine Janosky, 8 and Joseph A. Carcillo 7
Sepsis specific blood purification/kidney protection strategies • • Concept - Host inflammatory immune modulation Newly designed, hyper-adsorptive membranes – AN 69 Apheresis or selective plasma exchange Polymyxin B hemoperfusion Ø Cruz DN, Antonelli M, Fumagalli R, Foltran F, Brienza N, Donati A, et al. Early use of polymyxin B hemoperfusion in abdominal septic shock: the EUPHAS randomized controlled trial. JAMA. 2009; 301: 2445– 52 Ø Honore PM, Joannes-Boyau O, Boer W, Gressens B. High Volume haemofiltration and hybrid techniques in sepsis: new insights into the rationale. Neth J Crit Care. 2007; 11: 239– 42.
Blood Purification and Mortality in Sepsis: A Meta. Analysis of Randomized Trials*. Zhou, Feihu; MD, Ph. D; Peng, Zhiyong; MD, Ph. D; Murugan, Raghavan; MD, MS; Kellum, John; MD, MCCM Critical Care Medicine. 41(9): 2209 -2220, September 2013. DOI: 10. 1097/CCM. 0 b 013 e 31828 cf 412 Figure 2. Risk ratios for blood purification versus conventional treatment. Pooled risk ratios are from a random effects model; size of the data markers indicates weight of the study. MH = Mantel-Haenszel. © 2013 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc. 5
Blood Purification and Mortality in Sepsis: A Meta-Analysis of Randomized Trials*. Zhou, Feihu; MD, Ph. D; Peng, Zhiyong; MD, Ph. D; Murugan, Raghavan; MD, MS; Kellum, John; MD, MCCM Critical Care Medicine. 41(9): 2209 -2220, September 2013. DOI: 10. 1097/CCM. 0 b 013 e 31828 cf 412 Figure 3. Risk ratios for different modality of blood purification versus conventional treatment. Pooled risk ratios are from a random effects model; size of the data markers indicates weight of the study. A, Different modalities of blood purification versus conventional treatment 6 Published by Lippincott Williams © 2013 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins, Inc.
Summary – Therapies that prevent and treat sepsis induced AKI • Early resuscitation and antibiotics improves outcomes as measured by mortality and new AKI • Targeting Sc. VO 2 and MAP-CVP also improves outcomes as measured by mortality and new AKI • Fluid overload – Look for it and treat aggressively • Keep intrabdominal pressure < 12 • CRRT - Decision about when to , how to ( timing, dose) • Plasma exchange for thrombotic microangiopathy AKI • Role of anti-inflammatory strategies Type IV PDE I, Alkaline Phosphatase to be determined
Experimental Anti-inflammatory therapies Type IV PDEI inhibitors Alkaline Phosphatase
Effect of PDE 4 inhibition with Ro 20 -1724 on renal vascular resistance changes induced by zymosan and norepinephrine. Neal J. Thomas et al. J Pharmacol Exp Ther 2001; 296: 168174 The American Society for Pharmacology and Experimental Therapeutics
Effect of PDE 4 inhibition with Ro 20 -1724 on renal blood flow changes induced by zymosan and norepinephrine. Neal J. Thomas et al. J Pharmacol Exp Ther 2001; 296: 168174 The American Society for Pharmacology and Experimental Therapeutics
Effect of PDE 4 inhibition with Ro 20 -1724 on glomerular filtration rate changes induced by zymosan and norepinephrine. Neal J. Thomas et al. J Pharmacol Exp Ther 2001; 296: 168174 The American Society for Pharmacology and Experimental Therapeutics
RAP – Recombinant Alkaline phosphatase • Endogenous enzyme – Exerts detoxifying effects and combats renal inflammation through dephosphorylation of endotoxins, lipopolysaccharide and ATP. It is reduced during systemic inflammation Ø Peters E, Masereeuw R, Pickkers P. The potential of alkaline phosphatase as a treatment for sepsis-associated acute kidney injury. Nephron Clin Pract. 2014; 127: 144– 8. ( Exogenous RAP in septic patients improved endogenous creatinine clearance and reduced the requirement and duration of RRT ) Ø Peters E, Heemskerk S, Masereeuw R, Pickkers P. Alkaline phosphatase : a possible treatment for sepsis-associated acute kidney injury in critically ill patients. Am J Kidney Dis. 2014; 13: 1636– 43.