Prescribing Update Catherine Armstrong Lead Pharmacist Pharmicus GMC

Prescribing Update Catherine Armstrong Lead Pharmacist - Pharmicus

GMC – Good Practice in Prescribing & Managing Medicines and Devices • Effective from 25. 2. 13 • Must explain and justify decisions / actions • YOU are responsible for any script you sign • Several MUSTs and SHOULDs • Full guidance available: http: //www. gmc-uk. org/Prescribing_Guidance__2013__50955425. pdf

GMC – Unlicensed Medicines • • GMC recommends that GPs can prescribe unlicensed or “off license” medicines but, if you decide to do so, you must: Be satisfied that an alternative, licensed medicine would not meet the patient's needs Be satisfied that there is a sufficient evidence base and/or experience of using the medicine to demonstrate its safety and efficacy Take responsibility for prescribing the medicine and for overseeing the patient's care, including monitoring and any follow up treatment Record the medicine prescribed and, where you are not following common practice, the reasons for choosing this medicine in the patient's notes. (Code 8 B 2 V)

Which are specials? Drug Average cost • Paracetamol 120 mg/5 ml • Paracetamol 250 mg/5 ml • Paracetamol 500 mg/5 ml • £ 1. 12 per 200 ml • £ 1. 30 per 200 ml • £ 73. 76 per 200 ml • Morphine 10 mg/5 ml • Morphine 20 mg/1 ml • £ 1. 78 per 100 ml • £ 689. 57 per 420 ml • £ 4. 98 per 30 ml

Specials • Is a liquid formulation needed? • Is the drug readily available in a liquid form? • Can another drug be substituted? • e. g. fluoxetine liquid for sertraline tablets • COST of licensed option is not a reason to avoid using

Controlled Drug Prescribing Not needed Form? Needs dose

Gastro-Intestinal • Mucogel not Maalox • Peptac not Gaviscon Advance – Can use Gaviscon Advance tablets for portability • PPI – Omeprazole / Lansoprazole / Pantoprazole – Avoid Omeprazole 40 mg – use 2 x 20 mg – Consider C Diff risk

Domperidone Interaction • Small increased risk of serious ventricular arrhythmia or sudden cardiac death • Higher risk – Patients aged 60+ – Daily doses >30 mg • MHRA advice – Use lowest effective dose – Consider QT prolongation interacting meds

Metoclopramide Interaction • August MHRA Drug Safety Update • Contraindicated in <1 year old • Restricted use/doses <18 years old • Maximum of 30 mg per day for 5 days in adults

MHRA Simvastatin Alert • List of drugs contra-indicated with simvastatin • List of drugs - maximum dose of simvastatin – Main action: amlodipine & diltiazem • Primary Prevention – ↓ simvastatin 20 mg • Secondary prevention – depends on latest lipid profile • Action at next review of patient
 Acute")
FATS 6 - Secondary Prevention of CVD (symptomatic or prior occlusive vascular disease) Acute Coronary syndrome / Acute MI • Initiate Atorvastatin 80 mg All other conditions • Simvastatin 40 mg 1 st-line (unless interactions) • Repeat lipid profile 8 weekly and consider titration unless TC < 4 mmol/l, LDL-C (fasting) < 2 mmol, or non-HDL < 2. 8 mmol/l • Titrate to Atorvastatin 40 mg then 80 mg

FATS 6 - Type 1 and Type 2 diabetes Consider drug treatment in all Type 1 and 2 diabetics: • with microalbuminuria/proteinuria (any age) • over 40 years • under 40 years if other CV risk factors present. • Simvastatin 40 mg 1 st-line (unless interactions) • Repeat lipid profile 8 weekly and consider titration unless TC < 4 mmol/l, LDL-C (fasting) < 2 mmol, or non-HDL < 2. 8 mmol/l • Titrate to Atorvastatin 40 mg then 80 mg • If Type 2 diabetes and triglycerides > 1. 7 & < 10 mmol/l – lifestyle measures for 6 months then consider adding a fibrate (Fenofibrate 200 mg daily, reduced doses in CKD)
 • Treatment")
FATS 6 - Primary Prevention (no symptomatic or prior occlusive vascular disease) • Treatment is based on risk and not cholesterol levels • If 10 year CVD risk ≥ 20%, consider Simvastatin 40 mg (reduce dose for drug interaction – more detail in full guidance)
 if TC")
FATS 6 - Other points to note • Consider familial hyperlipidaemia (FH) if TC > 7. 5 mmol/l, LDL cholesterol > 4. 9 • Suspected FH if triglycerides > 4. 5 mmol/l • If triglycerides > 10 mmol/l, seek specialist advice Simvastatin 80 mg • Prescribing of Simvastatin 80 mg is no longer recommended due to risk of myopathy. • Review patients taking Simvastatin 80 mg their next routine appointment.

Dual Antiplatelet Therapy Aspirin 75 mg daily STEMI NSTEMI UNSTABLE ANGINA EITHER INVASIVE THERAPY TICAGRELOR 90 MG BD FOR 12 MONTHS OR INVASIVE NOT SUITABLE PRASUGREL 5 MG OR 10 MG OD FOR 12 MONTHS CLOPIDOGREL 75 MG OD FOR 12 MONTHS

Respiratory • Beclometasone inhalers – BRAND • Consider combinations • 2 new COPD inhalers • Consider quantities when reviewing

Pregabalin • Avoid more than 1 capsule per dose • QDS is not licensed, use maximum of TDS • Each capsule/strength priced the same - £ 1. 15 • Most popular “street” drug abused

Paracetamol doses 120 MG/5 ML 250 MG/5 ML AGE DOSE 3 -6 M 2. 5 ML 6 -8 Y 5 ML 6 -24 M 5 ML 8 -10 Y 7. 5 ML 2 -4 Y 7. 5 ML 10 -12 Y 10 ML 4 -6 Y 10 ML ALL UP TO QDS Do NOT use in under 6 yrs

Antibiotics • “Preferred” antibiotics: Amoxicillin Clarithromycin Doxycycline Flucloxacillin Metronidazole Nitrofurantoin Oxytetracycline Penicillin V Trimethoprim (Erythromycin) • Aim for 85% of prescribing to be these • Linezolid = HOSPITAL PRESCRIBING ONLY

C Diff • THINK – Patient - aged 65+, frequent Abx, recent Abx – Environment – contact, hospital admission, institutionalised – Action – avoid high risk: cephalosporins, ciprofloxacin/quinolones, clindamycin, coamoxiclav • TEST • TREAT

Role of 4 C antibiotics on local guidelines • Sinusitis – 1 st = amoxicillin, 2 nd = doxycycline – Co-amoxiclav 625 mg tds x 21 for persistant symptoms only • COPD exacerbation – 1 st – amoxicilllin, 2 nd = doxycycline – Co-amoxiclav 625 mg tds x 15 if resistant risk factors • Prostatitis Ciprofloxacin 500 mg BD x 56 • Cellulitis/Wounds – 1 st = flucloxacillin, 2 nd = clarithromycin – Co-amoxiclav 625 mg tds x 21 only if facial involvement • Human/Animal Bites Co-amoxiclav 625 mg tds x 21 • Pyelonephritis Co-amoxiclav 625 mg tds x 42 Ciprofloxacin 500 mg bd x 14

Minocycline • No clear evidence better than alternatives • Safety concerns + monitoring • Higher cost: Minocycline 100 mg M/R caps OD £ 10. 04 Doxycycline 100 mg caps OD £ 3. 92 Minocycline 100 mg caps OD £ 13. 09 Lymecycline 408 mg caps OD £ 6. 22 Minocycline 100 mg tabs OD £ 13. 72 Erythromycin 250 mg tabs 2 BD £ 7. 96 Minocycline 50 mg caps BD £ 15. 27 Oxytetracycline 250 mg tabs 2 BD £ 5. 32 Minocycline 50 mg tabs BD £ 11. 42 28 day courses (Drug Tariff August 2013)

Diabetic Drugs • Prescribe all insulin by brand name • Blood Glucose Testing advice – Type 1 - appropriate amounts – Type 2 - see local guidance – Consider latest DVLA advice also – local guidance under review as a result • Insulin Passports – NPSA safety alert, all patients aged 18+ using insulin should have or have opted out

Bisphonates • Alendronate or Risedronate 1 st line • Strontium has VTE warning – Avoid if current/previous VTE – Avoid if temporary/permanent immobilisation

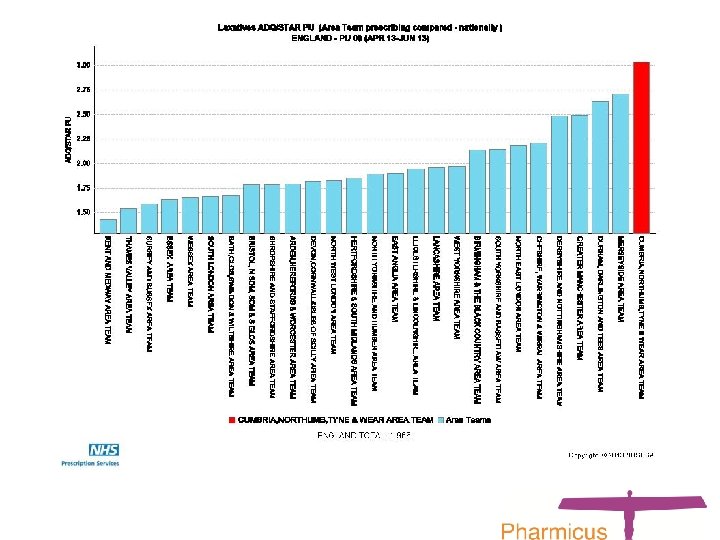
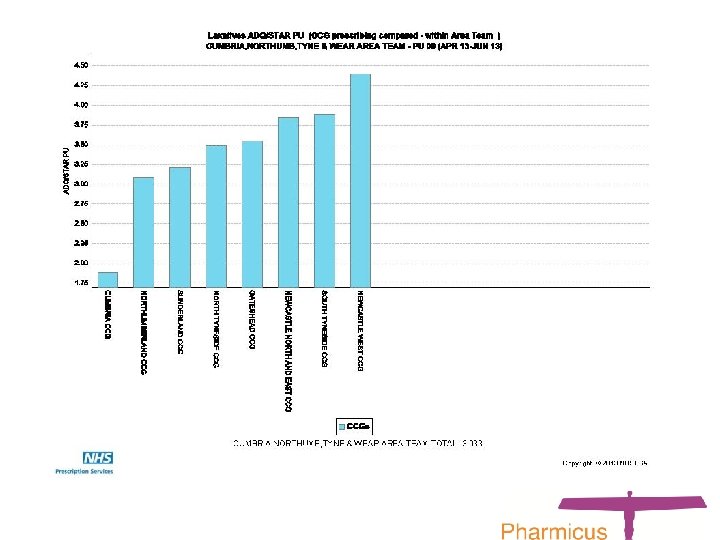
Prescribing Engagement Scheme • MANDATORY - Review of repeat prescribing and dispensing systems AND engagement with Pharmicus / Medicines Optimisation support • FINANCIAL – Collectively deliver financial balance for CCG ALL 3 AREAS Wound management Strong opioid prescribing (morphine) Laxatives Emollient s – Gateshead 1 st line antidepressants - Gateshead Erectile Dysfunction Drugs – Newcastle Ezetimibe – Newcastle North & East Effervescent analgesics – Newcastle West Venlafaxine MR caps to MR tabs – Newcastle West Specials – Newcastle North & East

Useful websites • Gateshead Information Network www. ginportal. info • North of Tyne Area Prescribing Committe www. northoftyneapc. nhs. uk • Electronic Medicines Compendium www. medicines. org. uk • Athens registration https: //register. athensams. net/nhseng/ • Medicines and Prescribing support from NICE http: //www. nice. org. uk/mpc/index. jsp
- Slides: 28