Prescribing Teaching 5 Max Roberts max robertsnhs net

Prescribing Teaching 5 Max Roberts max. roberts@nhs. net

Aims & Objectives The basics • Laxatives • Anti-emetics

https: //giphy. com

Laxatives

You’re about to go for lunch on your first shift as an FY 1 doctor – but before you’re able to walk out the door, you’re intercepted by a nurse who asks you to prescribe some laxatives for one of their patients. The patient has requested it herself because she’s feeling a bit bunged up and uncomfortable. Name: Margaret Jones, admitted 5/7 ago DOB: 1/5/1940 MRN: 1234567 Problem list: 1) Urosepsis resolved 2) Reduced mobility 3) Awaiting increased POC PMHx: T 2 DM HTN AF DHx: metformin 1 g BD ramipril 2. 5 mg BD amlodipine 5 mg OD warfarin 2 mg OD O/E (from morning ward round): NEWS 0; blood tests: unremarkable, CRP raised but improving Unremarkable examination, mild tenderness in suprapubic region Bowels: opening once every 2 days, type 4; last opened yesterday evening What will you prescribe?

Movicol 2 sachets Dr Doc BD 123 Docusate sodium 50 mg Dr Doc OD 123 PO Today Lactulose 15 ml Dr Doc Senna 7. 5 mg Dr Doc ON PO 123 Today BD 123 PO Today

How to know what to prescribe…?
 • Dehydration")
Laxatives Why do patients get constipated? • Immobility • Diet (low fibre) • Dehydration • Medication (opioids, anticholinergics/ondansetron, iron tablets) • Electrolyte disturbance (high [Ca], low [K]) • Intestinal obstruction • Pain on defaecation • Psychological factors

Laxatives Why is it a problem? • Pain/discomfort • Nausea & poor appetite • Urinary retention • Delirium • Overflow diarrhoea • Prolonged stay in hospital

Laxatives So what can we do about it without prescribing drugs? • Increase fluid intake • Increase fibre in diet • Early mobilisation • Ensure patients can reach the bathroom + privacy! • Posture: raised toilet seat

https: //www. 123 rf. com/photo_79737053_stock-vector-correct-sitting-get-the-proper-degree-angle-of-body-on-toilet-seat-for-help-with-excretion-. html

Laxatives Other principles of managing constipation: • Anticipate constipation, especially with opioids • Oral medications before rectal preparations • Try to keep tablet numbers down • Don’t use more than one laxative of the same type
 Osmotics 2) Stool softeners 3) Bulk-forming agents")
Laxatives 4 main types of laxatives: 1) Osmotics 2) Stool softeners 3) Bulk-forming agents 4) Stimulants
 Osmotics: These cause the intestines to retain")
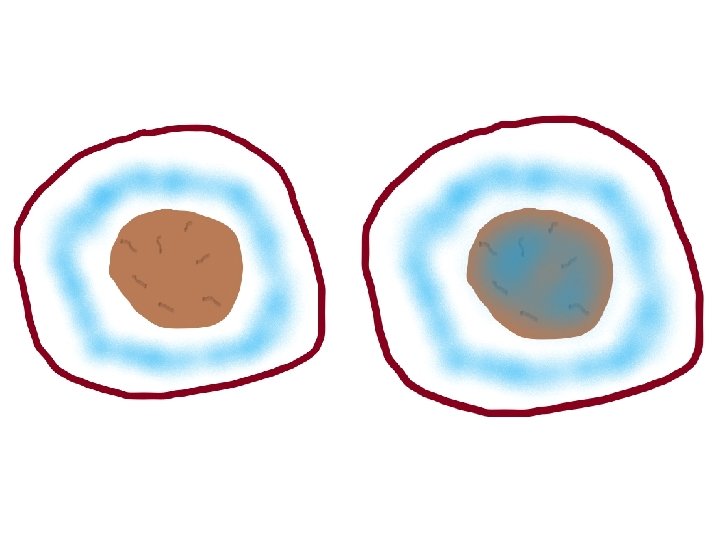
Laxatives 4 main types of laxatives: 1) Osmotics: These cause the intestines to retain more water Which helps makes the stool softer & bulkier, which helps peristalsis

bowel wall water stool

= osmotic laxative
 Osmotics: These cause the intestines to retain")
Laxatives 4 main types of laxatives: 1) Osmotics: These cause the intestines to retain more water Which makes the stool bulkier and helps peristalsis Macrogols (Movicol/Laxido), lactulose Patients need to drink a lot of water SE: bloating, cramping, flatulence (IBS-like symptoms)
 Stool softeners: Reduce surface tension of the")
Laxatives 4 main types of laxatives: 2) Stool softeners: Reduce surface tension of the stool (a bit like surfactant in the lungs) Allowing water & fat to be directly absorbed into the stool So the stool itself retains water
 Stool softeners: Reduce surface tension of the")
Laxatives 4 main types of laxatives: 2) Stool softeners: Reduce surface tension of the stool (like surfactant) Allowing water & fat to be directly absorbed into the stool So the stool itself retains water Docusate sodium is the most commonly used Also requires good fluid intake
 Bulk-forming: Similar to fibre, and are directly")
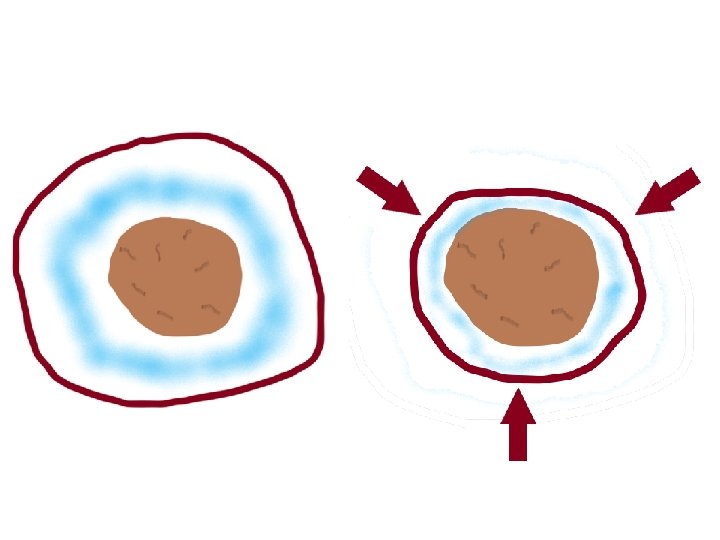
Laxatives 4 main types of laxatives: 3) Bulk-forming: Similar to fibre, and are directly incorporated into the stool Increase overall volume (‘bulk’) of stool, aiding peristalsis

bulk-forming laxative
 Bulk-forming: Similar to fibre Increase overall volume")
Laxatives 4 main types of laxatives: 3) Bulk-forming: Similar to fibre Increase overall volume (‘bulk’) of stool, aiding peristalsis Fybogel (isphagula husk) If fluid intake not adequate, they can worsen constipation and lead to faecal impaction
 Stimulants: Directly stimulate peristalsis through action on")
Laxatives 4 main types of laxatives: 4) Stimulants: Directly stimulate peristalsis through action on intestinal muscle
 Stimulants: Directly stimulate peristalsis through action on")
Laxatives 4 main types of laxatives: 4) Stimulants: Directly stimulate peristalsis through action on intestinal muscle Senna (Sennakot), bisacodyl (Dulcolax) Contraindicated in partial intestinal obstruction But good in cases where a patient can’t get good oral intake, e. g. IV fluids

Laxatives Other types: • Bowel prep - mixtures; clear out the whole bowel pre-colonoscopy • Suppositories - glycerin: osmotic • Enemas - phosphate: osmotic - arachis oil: stool softener

How to know what to prescribe…?

Laxatives How do we know what to prescribe? There’s no evidence base/guidelines Check local protocol But we can follow some simple rules…

Laxatives How often should people open their bowels? At least once every two days – but varies So if a patient is constipated (either subjective or objective): - talk to/examine the patient - do a PR exam

https: //radiopaedia. org/images/41297549? lang=gb

Laxatives If patient is not impacted or opening bowels at least once every three days: • start with osmotics: - lactulose 15 ml BD or Movicol 2 sachets BD • if the stool is soft on PR exam, add a stimulant as well - senna 15 mg ON • if stool is firm, add a stimulant after a few days, to let the osmotic take effect • if no improvement within 24 hrs, then either increase the doses or add a different type (e. g. stool softener) If constipation is chronic, bulk-forming agents are more ‘physiological’

Laxatives If they are impacted or they have not opened bowels for over three days - start osmotics - if stool in the rectum glycerin suppository, 4 g PR - if rectum empty or glycerin not effective phosphate enema PR - manual evacuation is a last resort that no-one wants…

Anti-emetics

You’re about to go home after your first shift as an FY 1 doctor – but before you’re able to walk out the door, you’re intercepted by a nurse who asks you to prescribe some anti-emetics for one of their patients, as he’s feeling a bit nauseous. Name: James Smith, admitted today DOB: 1/8/1985 MRN: 7654321 Problem list: 1) Renal colic for lithotripsy tomorrow PMHx: kidney stones DHx: diclofenac 50 mg BD PR Oramorph 5 mg 6 hrly PRN O/E (from afternoon ward round): NEWS 0; blood tests: unremarkable; normal ECG R-sided loin pain, no abdominal distension Bowels: opening daily, passing wind; weight 75 kg No vomiting Pain well-controlled Cannula in-situ What will you prescribe?

James Smith 7654321 1/8/1985 Ondansetron 4 mg Dr Doc Nausea TDS PO/IV 1234 Today Metoclopramide 10 mg Dr Doc Nausea TDS PO/IV 1234 Today Prochlorperazine 5 mg Dr Doc Nausea TDS PO 1234 Today Cyclizine 50 mg Dr Doc Nausea

How to know what to prescribe…?

Anti-emetics Why do patients feel sick? • • • Constipation/obstruction Food poisoning/infection (gastroenteritis, appendicitis, etc) Pain Severe cough Pregnancy Raised ICP Migraines Dizziness/motion sickness/inner ear problems Anxiety Medication (opioids, chemotherapy, alcohol) Electrolyte disturbances (hypercalcaemia) Seeing other people be sick…

Anti-emetics Principles of prescribing anti-emetics • Treat the cause • Conservative mgmt: avoid precipitating smells, acupressure wristsbands

https: //blog. dana-farber. org/insight/2016/12/how-to-perform-acupressure-for-vomiting-and-nausea/

https: //www. google. com/url? sa=i&source=images&cd=&ved=2 ah. UKEwigl. Yfb 6 ZPl. Ah. Wrz 4 UKHYh 4 A_o. Qj. Rx 6 BAg. BEAQ&url=https%3 A%2 F%2 Fwww. amazon. com%2 Facupressure-Anti-Nausea-Wristbands-controlling-chemotherapy%2 Fdp%2 FB 01351 B 8 WO&psig=AOv. Vaw 0 Qq 2 Kyy. V 8 q. Ngu. Dg 0 Pw 08 YS&ust=1570870210854341

Anti-emetics Principles of prescribing anti-emetics • Treat the cause • Conservative mgmt: avoid precipitating smells, acupressure wristbands • Is the patient actually vomiting? • If so, IV over oral + assessment of volume status • Regular or PRN? • Do we actually want to give anti-emetics? • The ‘better-out-than-in’ principle*: food poisoning, norovirus *I just made this name up

Anti-emetics http: //10. nhef. chfalaise. fr/label-ear-diagram-quiz. html Vestibular apparatus: H 1 receptors https: //commons. wikimedia. org/wiki/File: Pyramid_(medulla_oblongata)_-_lateral_view. png Cerebral cortex https: //www. pinterest. co. uk/pin/446911963007403716/ GI tract: D 2 receptors https: //www. researchgate. net/figure/Area-Postrema-is-Anatomical-Marker-for-the-Subregion-of-NTS-of-Primary-Hypothetical_fig 1_259320952 https: //commons. wikimedia. org/wiki/File: Pyramid_(medulla_oblongata)_-_lateral_view. png Vomiting centre: medulla Chemoreceptor trigger zone (CTZ): 5 -HT 3 receptors H 1 receptors
 Pro-kinetics: These mainly inhibit peripheral D 2 receptors in the GI tract")
Anti-emetics 1) Pro-kinetics: These mainly inhibit peripheral D 2 receptors in the GI tract (dopamine antagonists) They increase gastric output and gut motility So they’re good for nausea caused by gastric stasis: - large-volume vomiting with minimal nausea - acid reflux - early satiety - constipation (careful in bowel obstruction) https: //www. pinterest. co. uk/pin/446911963007403716/ Metoclopramide (which crosses the BBB), domperidone (which doesn’t) Don’t use in diarrhoea, partial bowel obstruction, or metoclopramide in Parkinson’s Haloperidol is also a dopamine antagonist, but we would only use it as an anti-emetic i palliative care
 Anti-histamines: These inhibit peripheral H 1 receptors in the vestibular system http:")
Anti-emetics 2) Anti-histamines: These inhibit peripheral H 1 receptors in the vestibular system http: //10. nhef. chfalaise. fr/label-ear-diagram-quiz. html So they’re good for nausea caused by motion sickness, labyrinthitis, etc Some H 1 receptors are found in our CTZ, so also good for raised ICP, drugs, etc Cyclizine and promethazine Side effects: sedation (careful in the elderly), anti-cholinergic side effects (blurred vision, dry mouth, constipation, urinary retention) IV cyclizine can also cause a transient ‘euphoria’
 Serotonin antagonists: These mainly inhibit peripheral 5 -HT 3 receptors in the")
Anti-emetics 3) Serotonin antagonists: These mainly inhibit peripheral 5 -HT 3 receptors in the chemoreceptor trigger zone So they’re good for nausea caused by chemotherapy and other drugs, as well as raised ICP Also good for post-operative nausea https: //www. researchgate. net/figure/Area-Postrema-is-Anatomical-Marker-for-the-Subregion-of-NTS-of-Primary-Hypothetical_fig 1_259320952 Ondansetron is our main serotonin antagonist used as an anti-emetic Side effects: constipation, serotonin syndrome if on SSRI/SNRIs, long QT syndrome So if patient has cardiac risk factors, then will need ECG monitoring

Anti-emetics Others: • Cerebral cortex: - dexamethasone: unclear mechanism, good for chemotherapy - benzodiazepines: anxiety • Anti-psychotics: - prochlorperazine (Stemetil): good for vestibular causes haloperidol: palliative care levomepromazine: broad spectrum big side effect profiles! don’t use if already on anti-psychotics
 A 30 -year-old man who presents to")
Anti-emetics Please prescribe some anti-emetics for: 1) A 30 -year-old man who presents to A&E, feeling like the room is spinning every time he turns his head. He is also having difficulty hearing and has recently had a cold. 2) A 90 -year-old man, admitted with delirium secondary to constipation. Background of Parkinson’s disease. Clinically improving and now mobilising around the ward with OT/PT input. Bowels still not opening regularly however, and feeling nauseous. 60 kg. 3) A 60 -year-old woman with lung cancer and brain metastases, who is feeling nauseous. She is on citalopram for depression and is on her first cycle of chemotherapy.
 A 30 -year-old man who presents to")
Anti-emetics Please prescribe some anti-emetics for: 1) A 30 -year-old man who presents to A&E, feeling like the room is spinning every time he turns his head. He is also having difficulty hearing and has recently had a cold. Cyclizine 50 mg TDS Dr Doc 1234 Nausea PO Today Prochlorperazine 5 mg TDS Dr Doc 1234 Nausea PO Today
 An 90 -year-old man, admitted with delirium")
Anti-emetics Please prescribe some anti-emetics for: 2) An 90 -year-old man, admitted with delirium secondary to constipation. Background of Parkinson’s disease. Clinically improving and now mobilising around the ward with OT/PT input. Bowels still not opening regularly however, and feeling nauseous. 60 kg. Domperidone 10 mg TDS Dr Doc 1234 Nausea PO Today
 A 60 -year-old woman with lung cancer")
Anti-emetics Please prescribe some anti-emetics for: 3) A 60 -year-old woman with lung cancer and brain metastases, who is vomiting intermittently. She is on citalopram for depression and is on her first cycle of chemotherapy. Cyclizine 50 mg TDS Dr Doc 1234 Nausea IV Today Ondansetron would work but be careful of serotonin syndrome Dexamethasone would also help – but only with senior input!

Anti-emetics http: //10. nhef. chfalaise. fr/label-ear-diagram-quiz. html Vestibular apparatus: H 1 receptors https: //commons. wikimedia. org/wiki/File: Pyramid_(medulla_oblongata)_-_lateral_view. png Cerebral cortex https: //www. pinterest. co. uk/pin/446911963007403716/ GI tract: D 2 receptors https: //www. researchgate. net/figure/Area-Postrema-is-Anatomical-Marker-for-the-Subregion-of-NTS-of-Primary-Hypothetical_fig 1_259320952 https: //commons. wikimedia. org/wiki/File: Pyramid_(medulla_oblongata)_-_lateral_view. png Vomiting centre: medulla Chemoreceptor trigger zone (CTZ): 5 -HT 3 receptors H 1 receptors

Anti-emetics There is more of a structure for prescribing anti-emetics than laxatives… …however, there is still a large element of trial-and-error. D 2 receptors 5 -HT 3 receptors ACh receptors H 1 receptors https: //commons. wikimedia. org/wiki/File: Pyramid_(medulla_oblongata)_-_lateral_view. png

Anti-emetics If the cause of the nausea is unclear/multi-factorial and there are no obvious contraindications: - metoclopramide 10 mg TDS PO/IV - cyclizine 50 mg TDS PO/IV - ondansetron 4 -8 mg TDS PO/IV (ECG first!) A single dose of ondansetron is good at preventing N&V in the first place

You’re about to go home after your first shift as an FY 1 doctor – but before you’re able to walk out the door, you’re intercepted by a nurse who asks you to prescribe some anti-emetics for one of their patients, as he’s feeling a bit nauseous. Name: James Smith, admitted today DOB: 1/8/1985 MRN: 7654321 Problem list: 1) Renal colic for lithotripsy tomorrow PMHx: kidney stones DHx: diclofenac 50 mg BD PR Oramorph 5 mg 6 hrly PRN O/E (from afternoon ward round): NEWS 0; blood tests: unremarkable; normal ECG R-sided loin pain, no abdominal distension Bowels: opening daily, passing wind; weight 75 kg No vomiting Pain well-controlled Cannula in-situ What will you prescribe?

Thanks! Any questions? www. surveymonkey. co. uk/r/29 Z 3 VF 5
- Slides: 56