Prenatal Care Goals of Prenatal Care Testing order





























")






 >15, 000")





















 (WHO) Total Weight")


, 98,")




: 685 - 690, 2008), probably 2000")











: o Growth retardation o Facial anomalies")












- Slides: 94
Prenatal Care
Goals of Prenatal Care Testing – order certain tests at certain times o Surveillance – watch for warning signs of complications, check growth, etc. o o o Education - this is a great “teachable moment” in people’s lives (and maybe. . . relationship-building)
Contents of this talk: Efficacy of Prenatal Care o Timeline for routine testing o o Review of elements of the testing o o o Common Pregnancy Discomforts Pregnancy Nutrition (evidence-based) Supplements recommended in pregnancy Exercise Toxins – o Tobacco, alcohol, environmental exposures
Prenatal Care and Outcomes Inadequate prenatal care is associated with 2 -3 x risk preterm delivery J Am Osteopath Assoc. 2000 Aug; 100(8): 485 -92. But which direction is the causality? o
Risk factors for inadequate prenatal care: o o o Low educational achievement High parity, living with at least one child Unmarried Uninsured Smokers History of substance use/abuse J Matern Fetal Neonatal Med. 2004 Jul; 16(1): 45 -50.
How effective is our care? 1986 - US tied for 17 th place in infant mortality internationally - 10. 4 deaths/1000 live births o 2008 - US ranked 29 th in infant mortality o o Number of women receiving prenatal care in US has increased over past few decades
Still, maybe parts of what we do are helpful. .
Routine Measurements in Prenatal Care and Levels of Evidence Examination Component and Recommendations Level of Evidence Abdominal Palpation to assess presentation at 36 weeks B Blood pressure measurement at each visit C Evaluation for edema C Fetal heart tones C Fetal movement counting A – do not do routinely Symphysis fundal height measurement B Urinalysis C – some recent guidelines say no Weight measurement first visit B Weight each visit C Am Fam Physician 2005; 71: 1307– 16, 1321– 2
Prenatal vitamins Am J Epidemiol 1997; 146: 134 -41.
Health Behavior Advice and Low Birth Weight o Not receiving all the types of advice* associated with ↑risk LBW Infant (odds ratio = 1. 38; 95% confidence interval, 1. 18 to 1. 60) o Controlled for sociodemographic, utilization, medical, and behavioral factors JAMA 1994; 271: 1340– 5. * As recommended by the Expert Panel on the Content of Prenatal Care
Does prenatal education change behavior? West J Nurs Res 2007; 29; 258 Susan C. Vonderheid, Kathleen F. Norr and Arden S. Handler Prenatal Health Promotion Content and Health Behaviors
Are some modes of care delivery more effective at changing behavior? Table 3. Breastfeeding Initiation Rates and Rates at 6 Months for Each Group MCN, American Journal of Maternal Child Nursing. 33(5): 315 -319, September/October 2008. DOI: 10. 1097/01. NMC. 0000334900. 22215. ec © 2008 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
Group Prenatal Care RCT. Preterm delivery for total sample and African Americans only. All analyses were controlled for factors that were different by study condition. (PP=. 045; African American only: OR 0. 59, 95% CI 0. 38 -0. 92, P=. 02. ) Obstetrics & Gynecology. 110(2, Part 1): 330 -339, August 2007.
Centering
Bottom Line: We are not sure it makes a difference to provide prenatal care o Some aspects of care may be more effective, and they are the educational aspects o Our current delivery system may not be the best – groups and other strategies may make more sense o
Problems with current PNC Recommendations o Direction of communication o Lecturing vs. interchange o Focus on physical above the psychosocial o Violence more common than other conditions for which women are routinely screened o Emphasis on risk o Increases cost but generally does not improve outcome o Additive expectations – o Counseling on genetic testing, etc. in early pregnancy distracts from general health promotion
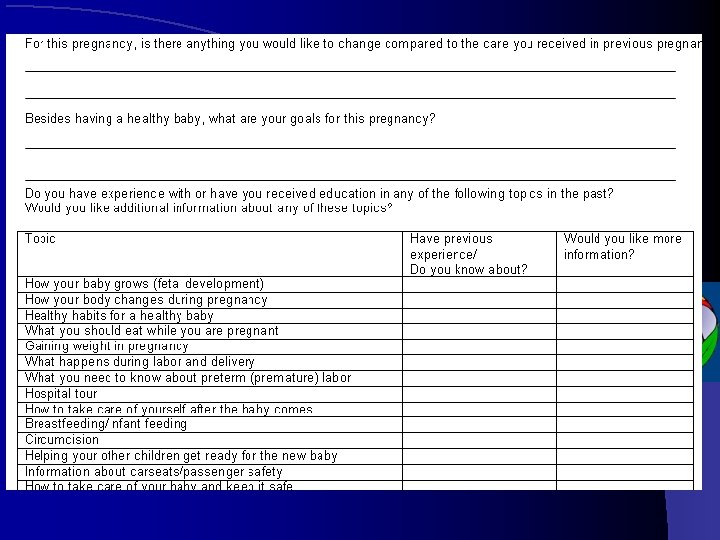
Direction of Communication o Adult learners are self-directed, goaloriented – want practical personally relevant information o My old practice had a questionnaire as part of intake process asking patients to rank their priorities for education
What do patients want? Continuity – same provider as much as possible o Comprehensiveness - counseling, education services, and support groups o Control - more collaborative providers who were good listeners and fostered their involvement in making decisions o Novick G. Women’s experience of prenatal care: An integrative review. J Midwifery Womens Health 2009; 54: 226– 37
Problems with current PNC Recommendations o Direction of communication o Lecturing vs. interchange o Focus on physical above the psychosocial o Violence more common than other conditions for which women are routinely screened o Emphasis on risk o Increases cost but generally does not improve outcome o Additive expectations – o Counseling on genetic testing, etc. in early pregnancy distracts from general health promotion
Problems with current PNC Recommendations o Direction of communication o Lecturing vs. interchange o Focus on physical above the psychosocial o Violence more common than other conditions for which women are routinely screened o Emphasis on risk o Increases cost but generally does not improve outcome o Additive expectations – o Counseling on genetic testing, etc. in early pregnancy distracts from general health promotion
The Fear-Monger’s Shop Pregnancy is a normal process and generally women get through with no problems o The medical model teaches us to be vigilant for problems, and to test women to be sure things are OK o o Be aware of our “glass half empty” approach and discuss this with patients
Problems with current PNC Recommendations o Direction of communication o Lecturing vs. interchange o Focus on physical above the psychosocial o Violence more common than other conditions for which women are routinely screened o Emphasis on risk o Increases cost but generally does not improve outcome o Additive expectations – o Counseling on genetic testing, etc. in early pregnancy distracts from general health promotion
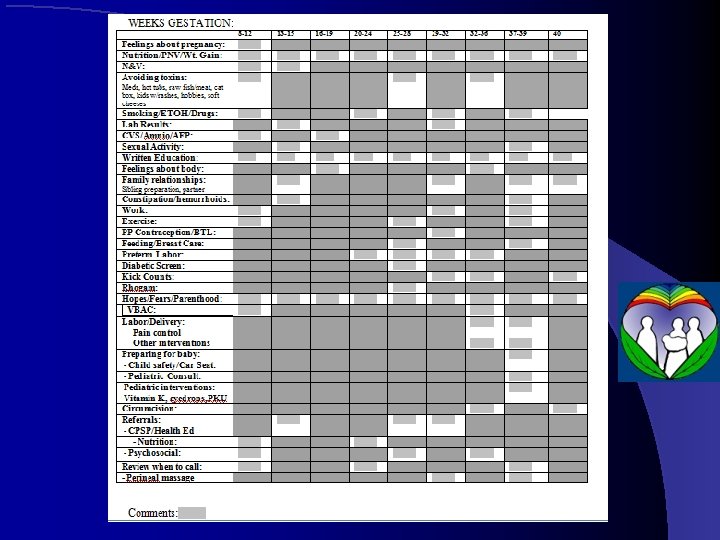
Plus, how do you keep track of education? o A: Systems
Still, this is what we do. . .
The Simple Version o o o o Intake: Medical risk assessment, Psychosocial risk assessment, Prenatal panel 11 ½ - 14 weeks – first trimester screening; early DM screening at 14 weeks if risk factors 16 -20 weeks 2 nd trimester screening 18 -20 weeks sono for anatomy 24 -28 weeks GTT, CBC, Rhogam if indicated 35 -7 weeks GBS All along, weight, BP, fundal height (urine dip removed in recent EBM guidelines)
How many visits? We still see them q 4 weeks until 28 -30, q 2 weeks to 36, weekly thereafter o Fewer (mean of 5 visits) has equivalent outcomes Lancet 2001 May 19; 357(9268): 1551 o
Initial Evaluation Medical risk assessment for mom o Genetic/teratogenic risk assessment for fetus To include: o o Health conditions – HTN, DM, asthma, etc. o Psychosocial stressors/health behaviors Domestic violence l Substance use l Work exposures l
Testing Blood type, Rh, and antibody screen o Complete blood count o VDRL, HIV, HBs. Ag, chlamydia/gc o Rubella screen for immunity o Consider Pap smear if due but not just as a routine o Urine for protein, glucose, asymptomatic bacteriuria o
Additional Testing Hemoglobin electrophoresis o Thyroid screen – have a low threshold for sx o Early 1 -hour 50 -gm glucola challenge-14 wk o o FH DM, previous GDM, h/o macrosomic infant, obesity, maternal age >30 PPD o Toxoplasmosis – not recommended o Hepatitis A and C screen. o Wet prep if high risk for preterm delivery o
Dating Menstrual history – definite date and regular menses o Physical exam (S=D? ) o Ultrasound if indicated o o According to ACOG guidelines, OB ultrasound as a parameter for pregnancy dating is accurate within the following ranges: l + 1 Week < 20 Weeks l + 2 Weeks From 20 -30 weeks l + 3 Weeks > 30 Weeks
Genetic Screening o General principle: order a test if you will do something different based on the results
Genetic Screening o o The Modern Age or Brave New World? Benefits: o Information about an affected baby may allow parents to make a choice to terminate a pregnancy or plan delivery differently o If considering this option, tests that give results earlier in pregnancy allow earlier termination, which is safer o Risks: False positive and false negative tests These choices can be emotionally difficult Invasive testing involves some risk of miscarriage Cost: blood testing $105 -900 Amnio ~$2500 CVS ~$2000 Ultrasound: $400 - $900 o o
Genetic Screening o Blood testing for recessive problems: o Family history of birth defects or inherited problems o Ethnicity: l l Tay-Sachs disease: Occurs in 1 out of 3, 600 infants of Ashkenazi Jewish or French-Canadian parents. Sickle Cell disease: Affects approximately 1 out of 400 African Americans and a small percentage of Native Americans and people of Mediterranean descent o Cystic Fibrosis: 1 out of 2, 500 Caucasian descent.
Screening for Down’s o Non-invasive tests: o Benefits: No risk of pregnancy loss attributed to the test o Shortcoming: Troubled by false negative and false positive results o Options: o NT and PAPP-A 11 1/2 -14 weeks o AFP/Quad marker screening 16 -19 weeks
Diagnostic Testing for Down’s Offered for at-risk pregnancies: age over 34 or positive result on a screening test o Accurate: false positive or false negative extremely rare o Riskier: some increased incidence of miscarriage from the testing o Options: o o CVS (Chorionic Villus Sampling) at 10 -12 weeks – 0. 5 - 1% risk of miscarriage, rare limb injury o Amniocentesis at 16 weeks – 0. 3 - 0. 5% risk of miscarriage
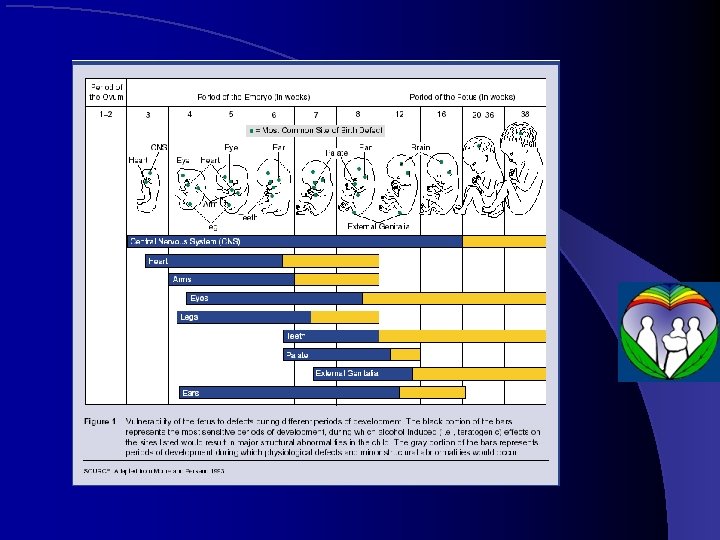
Screening Ultrasound o Safety: o Studied with lower energy technology than current. Confirmed effects have been found in mammals undergoing ultrasound exposures equivalent to current exposures. Am J Obstet Gynecol 1998; 179: 241 -54 o In humans, reported effects include growth restriction, delayed speech, dyslexia, and nonright-handedness associated with ultrasound exposure Epidemiology. 13(3) Supp: S 19 -S 22, May 2002
Efficacy - Sensitivity RADIUS study (Routine Antenatal Diagnostic Imaging With Ultrasound Study) >15, 000 women 16 -20 weeks and again at 31 - 33 weeks: Sensitivity 17% on first ultrasound, 35% overall o Eurofetus study: > 200, 000 women Sensitivity 61% (74% for major malformations) o False-positive: o o Eurofetus study, 10 percent of positives were false-positive
What will you do with the results? o No significant impact on the frequency of abortion for fetal anomalies. Survival rates for anomalous fetuses were also unaffected by screening. AM J OBSTET GYNECOL 1994; 171: 392 -9 o 27 fetuses w/severely crippling or lethal abnormalities; termination of pregnancy requested in 25. Early dx influenced timing and place of delivery in babies with severe cardiac or gastrointestinal anomalies BMJ. 1992 June 6; 304(6840): 1474.
GTT 50 gram, 1 -hour GTT universal screening 24 -28 weeks; Abnl is >130 mg/d. L o Equal sensitivity with jelly beans (28 Brachs -100 jelly beans); o o Jelly beans yielded fewer side effects (38% with 50 -g glucose beverage, 20% with jelly beans; P <. 001) and were preferred by 76% of participants (P <. 001) Am J Obstet Gynecol. 1999 Nov; 181(5 Pt 1): 1154 -7
Follow-up of Abnormal GTT o 3 -hour, 100 gram GTT: 95, 180, 155, 140 o 2 abnormals: definitive dx GDM o 1 abnormal: offer dietary counseling and repeat test in one month (vs. treat as diabetic). more macrosomia and neonatal hypoglycemia than normals or GDM patients under treatment l 28. 7% have IGT in 7 years (35% of those with GDM, 9% controls) Am J Obstet Gynecol. 1987 Sep; 157(3): 758 -63 l
GBS o Rectovaginal swab – patient self-collection equivalent to physician collection J Am Board Fam Med. 2009 Mar-Apr; 22(2): 136 -40. o 79% of women preferred self-sampling or had no preference. Less-educated women may be hesitant to self-sample, and clinician sampling should remain an option J Obstet Gynaecol Can. 2006 Dec; 28(12): 1083 -8.
Childbirth Education Encourage this and parenting preparation throughout o Check out classes if you are able o o Some are empowering o Some are fear-mongering o Hypnobirthing is particularly great
End of the line. . . o Induction by 41 weeks if undelivered decreases the risk of C/S o Hannah ME - N Engl J Med - 11 -JUN-1992; 326(24): 1587 -92 o Cochrane Database Syst Rev 2004; (3): CD 000170. o Obstet Gynecol 2003; 101: 1312– 8. o Or earlier if high risk. . . o Antepartum monitoring vs. induction
Antepartum Monitoring o Subject of another talk, but consider for o Chronic Hypertension at 32 weeks o GDM requiring meds at 32 weeks o IUGR (including suspected while sono pending) o Advanced maternal age o Other maternal conditions (APL syndrome, sickle cell, substance abuse, abnormal first or second trimester screen – ms. AFP, msh. CG, PAPP-A) o And more. .
So what do we do with the rest of our time? Address discomforts Health Promotion
Address Discomforts Credibly and empathetically addressing discomforts and empowering patients in their self-care builds your relationship with them o Guide them towards safer remedies o
Common Discomforts Pregnancy Complaints Handout: Allergies/hayfever Nausea/Vomiting Heartburn Constipation Diarrhea Pain Headaches
Connie’s Pearls for Discomforts o o o o Allergies/hayfever – nasal saline, topical nasal meds Nausea/Vomiting – B 6, ginger, Neiguan acupressure Heartburn – digestive enzymes, tums before meds Constipation - magnesium Diarrhea - fiber Headaches – hydration (incl salt), magnesium to bowel tolerance Vein health – foods high in flavonoids (apples, onions, blueberries, citrus – the white part) Leg cramps – calcium and magnesium
Sex in Pregnancy Libido can increase, decrease, or be unchanged in pregnancy – nice to normalize this for couples o No association with miscarriage risk o No risk of head injury to baby, etc. o Some association with preterm labor o o Prostaglandins in semen – a chemical that can trigger contractions o Women who are sensitive to this effect might consider condom use/withdrawal from 20 – 35 weeks
Health Promotion! Capitalize on the Teachable Moment o o o o Infection Prevention – handwashing, food, etc. Nutrition Exercise Tobacco Alcohol Breastfeeding Parenting
Pregnancy Nutrition All bets are off in first trimester: eat what will stay down! o Lots of fruits and veggies (but go easy on juice) o o Antioxidants – help prevent preeclampsia Journal of Nutrition, Vol. 139, No. 6, 11621168, June 2009 o Limit processed foods. . .
Variety of Foods - Imprinting Dietary flavors are transmitted and flavor amniotic fluid o Experiences with such flavors lead to heightened preferences for these flavors shortly at birth and at weaning o Exposure to a flavor (eg, carrots, garlic, fruits) in mothers’ milk influences infants’ liking and acceptance of that flavor in a food base Journal of Pediatric o Gastroenterology and Nutrition 48: S 25–S 30 # 2009
Pregnancy Nutrition o Lots of protein o Vegetarians: be careful about excessive soy <16 weeks. o Calcium – 1000 -1300 mg/d o Mediterranean Diet? o Odds ratios for preterm birth and early preterm birth were 0. 61 (95% Confidence Interval (CI): 0. 35 -1. 05) and 0. 28 (0. 11 -0. 76), respectively, in MD women compared to women fulfilling none of the MD criteria Acta Obstetricia & Gynecologica Scandinavica; Mar 2008, Vol. 87 Issue 3, p 325 -330
Sucrose and Risk
Pregnancy Nutrition, cont’d o Avoid sugar o The equivalent of 1 ½ cans of soda per day increases preeclampsia risk by a factor of 17! o Big babies: insulin is a growth factor l o Glycemic index of foods – low GI diets stimulate less insulin secretion Milk: o 1 -2 cups per day may help prevent preeclampsia o Increased milk may contribute to big babies o Increased milk definitely contributes to risk of childhood -onset diabetes in the baby
Food Safety o Avoid: o o o Raw dairy or juice: listeria Deli meat (or have it heated to steaming) Anything undercooked; also wash fruits and veggies well Vitamin A >5000 IU per day (organ meats, etc. ) Fish (because of mercury, PCBs) – 12 oz per week OK per US gov.
Pregnancy Nutrition, cont’d o Organic vs. Not: o Data on contaminants found in meconium, cord blood* o Biomagnification o 12 most contaminated fruits and veggies: Strawberries Peaches Apricots Bell peppers Cantaloupe Green beans Spinach Celery Grapes Cherries Apples Cucumbers • http: //www. ewg. org/minoritycordblood/home Per the • Endocrine Society: even infinitesimally low levels of exposure [to endocrine-disrupting chemicals] –indeed, any level of exposure at all– may cause endocrine or reproductive abnormalities, particularly if exposure occurs during a critical developmental window. Surprisingly, low doses may even exert more potent effects than higher doses. ” More on this at the end if time allows. . . “
How Low-Income Women Can Eat Healthy Foods in Pregnancy o Those who ate healthy foods: • knew to eat balanced meals • had family support • willing to prepare foods that were different than other family members • ate at home more frequently Health Care for Women International, 26: 807– 820, 2005
IOM Guidelines for Weight Gain in Pregnancy Prepregnancy BMI+ (kg/m 2) (WHO) Total Weight Gain Range (lbs) Underweight <18. 5 28– 40 Normal weight 18. 5 -24. 9 25– 35 Overweight 25. 0 -29. 9 15– 25 Obese (includes ≥ 30. 0 all classes) 11– 20 Rates of Weight Gain* 2 nd and 3 rd Trimester (Mean Range in lbs/wk) 1 (1– 1. 3) 1 (0. 8– 1) 0. 6 (0. 5– 0. 7) 0. 5 (0. 4– 0. 6) Note contradictory findings in German study: 8 -25 kg, 2 -18 kg, -7 to 12 kg, -15 to 2 kg Am J Clin Nutr. 2009 Dec; 90(6): 1552 -8.
Weight Gain in Pregnancy o Significant controversy – my approach is to consider weight gain an indicator, not a goal o Assure nutritional adequacy of micronutrients, protein o Limit toxic calories – refined sugar, trans fats, etc. o NO DIETING!
Supplements o Prenatal vitamins and minerals o Consider a “green drink”/vegetable powder if vegetable intake inadequate B 12 for vegetarians o Fish oil – target 200 - 300 mg DHA/day o o Benefits of omega 3’s for mom and baby Vitamin D o Probiotics? o Calcium (if low intake), - decrease preterm delivery, PIH o Magnesium– o o decrease in preterm delivery 15 mmol mg-aspartate Br J Obstet Gynaecol. 1988 Feb; 95(2): 120 -5
Omega-3’s in Pregnancy o Reduced early preterm delivery British Journal of Nutrition (2007), 98, 253– 259 o Baby brain development o Prog Lipid Res. 2001; 40: 1– 94; J Pediatr. 2003; 143: S 17; This American Journal of Clinical Nutrition, Vol. 85, No. 6, 1572 -1577, June 2007
Omega-3’s in Pregnancy o Baby Atopy o Asthma reduced 63% up to 16 yo Am JClin. Nutr, Vol. 88, No. 1, 167 -175, July 2008 o Atopic Dermatitis Curr Opin Allergy Clin Immunol. 2005; 5: 215– 21. Proceedings of the Nutrition Society (2010), 69, 316– 323 o Proc Nutr Soc. 2010 Aug; 69(3): 373 -80. o Lower blood pressure at age 6 Br Med J. 2003; 953 o Decreased BMI in late infancy Journal of Perinatal o Medicine. Volume 35, Issue 4, Pages 295– 300
Omega 3 and Mood Disorders o Perinatal Depression – o Epidemiology – lower DHA content in mothers' milk and lower seafood consumption were associated with higher rates of postpartum depression J Affect Disord. 2002 May; 69(1 -3): 15 -29 o Antepartum RCT 62% vs. 27% response rate American Journal of Clinical Nutrition, Vol. 88, No. 1, 167 -175, July 2008 o Postpartum interventional trials disappointing l 200 mg per day starting week 16 not helpful • Prog Neuropsychopharmacol Biol Psychiatry. 2009 Feb 1; 33(1): 49 -52
Vitamin D o Low D assoc with o BV J Ped Ad Gyn 2009 Jul 28 o Risk for primary C/S: controlling for race, age, education level, insurance status, and alcohol use, women with 25(OH)D less than 37. 5 nmol/liter were almost 4 times as likely to have a cesarean than women with 25(OH)D 37. 5 nmol/liter or greater (adjusted odds ratio 3. 84; J Clin Endocrinol Metab. 2009 Mar; 94(3): 940 -5 o preeclampsia, LBW, neonatal hypocalcemia, poor postnatal growth, bone fragility, and increased autoimmune dz Am J Obstet Gynecol. 2009 Oct 19.
More on Vitamin D o GDM: After adjustment for covariates including BMI, vitamin D deficiency was associated with a 2. 66 -fold increased GDM risk PLo. S One. 2008; 3(11): e 3753 o Eczema/wheeze in infants and asthma/allergic rhinitis in 5 -year olds Clin Exp Allergy. 2009 Jun; 39(6): 875 -82 o Bone health(even in adolescence), prevention of DM 1, prevention of schizophrenia, possibly certain cancers; deficiency can present w/ seizures Crit Rev Clin Lab Sci. 2008; 45(4): 339 -414 and others
Supplementing D Dose: >800 IU/d (Clinical Endocrinology 70(5): 685 - 690, 2008), probably 2000 IU per day o Preeclampsia risk ↓ 27% for women taking 10– 15 µg/d (400 – 600 IU) Epidemiology 20(5), 2009, pp 720 -726 o Interventional trial: Ca, vitamin D decreased preeclampsia rate from 17 to 10% in high-risk population Int J Gynaecol Obstet. 1994 Nov; 47(2): 115 -20 o
Probiotics o L. rhamnosus to mothers, one month before through six months after delivery, or to the infants themselves. o → 50% ↓ incidence atopic eczema in at-risk infants at ages 2 and 4 Lancet 361: 1869– 1871, Lancet 357: 1076– 1079
Other conditions responsive to Probiotics o Decreased incidence and increased resolution of bacterial vaginosis. Clin Ther 1992; 14(1): 11 -16, Microbes and Infection 2006; 8: 1450 -54 and candidal vaginitis Lett Appl Microbiol 2009; 48(3): 269 -74 including decrease in preterm delivery in a Russian study *Dobrokhotova YE, Sci M All-Russian Scientific Forum: Mother and Baby. October 2, 2007 o Decreased incidence or recurrence of urinary tract infections Microecology Therapy 1995; 23: 32 -45
And obesity? Dietary No treatment counseling + + placebo probiotics Central obesity 1 year 25% after childbirth (BMI > 30 or waist circ >80 cm) 43% 40% Presentation at European Congress on Obesity by Kirsi Laitinen May 2009 o Speculations on mechanism: Mayo Clinic Proceedings April 2008 vol. 83 no. 4 460 -469 o Better glucose tolerance in the diet/probiotics group was confirmed by a reduced risk of elevated glucose concentration compared with the control/placebo group (OR 0. 31 (95 % CI 0. 12, 0. 78); P = 0. 013) as well as by the lowest insulin concentration (adjusted means 7. 55, 9. 32 and 9. 27 m. U/l; P = 0. 032) and homeostasis model assessment (adjusted means 1. 49, 1. 90 and 1. 88; P = 0. 028) and the highest quantitative insulin sensitivity check index (adjusted means 0. 37, 0. 35 and 0. 35; P = 0. 028) during the last trimester of pregnancy. Br J Nutr. 2009 Jun; 101(11): 1579 -80.
Exercise in Pregnancy – recommendations are C level o Safety: o No clear connection between exercise and miscarriage or birth defects – but watch for increases in body temperature o Vigorous exercise throughout pregnancy may be associated with a slight decrease in birth weight (conflicting data) o Avoid scuba diving, high-impact exercise
Exercise in Pregnancy - Benefits o Lower risk of BW > 90 th %ile Obstet Gyn 2009 Oct; 114(4): 770 o Shorten labor, decrease fetal distress and operative delivery Am J Obstet Gynecol 1990 Dec 1990; 163(6): 1799, J Reprod Med 1990 Jul; 35(7): 704; Am J Obstet Gynecol. 2009 Dec 18 o Improve glycemic control in GDM Diabetes 1991 Dec; 40 Suppl 2: 182 o Decrease the “third trimester miseries” Med Sci Sports Exerc 1995; 27(5): 634 o Decreased risk of preterm delivery. Am J Obstet Gynecol 2008; 198: 180
Exercise in Pregnancy - Comfort Ligamentous laxity starts for some women fairly early in pregnancy – be cautious with stretching and yoga poses o Supine positioning: if there is a circulatory compromise in this position, women will generally feel it before their baby does o Swimming places the least stress on the joints and back (Tsunami Mommies) o
Tobacco in Pregnancy o Nicotine: o Constricts blood vessels o Is concentrated by the placenta – levels are 10 - 15% higher in the fetus than the mother o Interacts with specific neuroreceptors for acetylcholine in the developing brain o Carbon monoxide decreases oxygen delivery to the fetus
Tobacco Effects Not just smaller babies. . o Pregnancy effects: o Miscarriage 2 X o Growth restriction 4 X o Preterm PROM 3 X o Preterm labor 2 X o Abruptio placentae 2. 5 X o Placenta Previa 3 X
Tobacco Effects: the baby Withdrawal syndrome in neonatal period o Colic o Brain development: o o Shorter attention span o Increased hyperactivity o Increased conduct-disordered behaviors o SIDS
Who o Not just the mom. . . o Maternal passive smoking was associated with 2 x risk of low birth weight in one study
Quitting o Quitting smoking is hard o Now is women’s most motivated time to quit o It really helps if everyone in the household quits at the same time o Even cutting down is helpful – o Many of the risks decrease dramatically when a woman gets to 10 or fewer cigarettes per day
Alcohol in Pregnancy o Fetal Alcohol Syndrome (FAS): o Growth retardation o Facial anomalies o Central nervous system dysfunction o Alcohol-Related Neurodevelopmental Disorder – (ARND) just the brain dysfunction o More common o Can happen with as little as 8 drinks per week or 5 drinks on one occasion o Alcohol Related Birth Defects (ARBD) Cardiac Skeletal Renal CNS
Fetal Alcohol Syndrome
Behavior and Alcohol Exposure Odds ratio for delinquent behavior 3. 2 in alcohol-exposed children vs. unexposed kids o ADHD cases 2. 5 times more likely to have been exposed to alcohol in utero as controls (and 2. 1 times more likely to have been exposed to cigarettes) o
Dose Response Effects are seen in 10% of infants exposed to 1 oz of alcohol daily o Seen in 40% of those exposed to 5 oz per day o The same weekly dose via binge drinking is more harmful than lower, daily usage
Other Determinants of Injury o Genetic determinants of damage: o Alcohol dehydrogenase 2 genotype 1/3 – those who can drink more with less intoxication may be at more risk o In rats, fish oil was partially protective against brain effects of fetal alcohol exposure
Manifestations of Toxins Affecting Pregnancy o o o Increased SAB rate Malformations Neurotoxicity Endocrine Disruptors DNA modification with epigenetic effects o a fungicide exposure in rats caused tumors, kidney problems etc. for 4 generations
Endocrine Disruptors o Phthalates – plastic softener, cosmetics SAB, PTL, decrease in anogenital distance, smaller penis in children o BPA – hard clear plastic, some recycling #7, thermal cash register receipts SAB, ADHD in girls, feminization in boys Herbicides (atrazine) – dec semen quality, insulin resistance, Pesticides o PCB’s – thyroid fetal growth, cognitive delays o Organic solvents – toluene, xylene, styrene o OR 2. 9 for SAB in painters o 1. 6 in cosmetologists (nail polish-exposed) o
Endocrine Disruptors. . . Triclosan – inhibits estrogen sulfonation in placenta o PFOA, PFOS (nonstick cookware, microwave o popcorn, etc. ) low birth weight, preeclampsia o Red meat - maternal consumption in pregnancy correlates with low sperm count in the sons (!) Hum Reprod. 2007 Jun; 22(6): 1497 -502. o Trihalomethanes – in tap water SAB OR 2. 17 – 2. 8 for highest consumption o PAH – polycyclic aromatic hydrocarbons – blacktop, exhaust, grilled foods, cigarettes, coal tar shampoo OR 2 IUGR; OR 5 for Preterm delivery
More Toxins Affecting Pregnancy EMF’s? : OR for SAB 1. 8 for >20 hr/wk use of CRT o Caffeine: OR 1. 73 for SAB if intake >150 mg/d (but o nausea could be a confounder) o Heavy Metals –actively transported by placenta o Mercury – SAB, PTL, neurological impairment o Lead – as above o Cadmium – LBW, Low IQ Tobacco o Alcohol o
Preconception Care o Any annual or other visit may be a preconception visit o MVI/folate prior to conception o Correct iron deficiency prior to pregnancy o Confirm vaccinations (MMR) o Toxins – Limit/avoid alcohol l Medications l Plastics, mercury, etc. l o Control diabetes. . .
Helpful Resources o Am Fam Physician 2005; 71: 1307 -16, 1321 -2 o Review of prenatal care – levels of evidence, content of counseling, etc. o ICSI – Guidelines for Routine Prenatal Care o Nice sample questionnaires for assessing risk Toxins in Pregnancy: o Protecting Children from Environmental Toxins. PLo. S Med 2(3): e 61 – review of vulnerability of children to environmental toxins o For patients: • Raising Baby Green, by Alan Greene • Having Faith, by Sandra Steingraber
More Resources o J. Nutr. 133: 1606 S-1625 S, May 2003 o Review on nutrition in pregnancy o Implications of vitamin D deficiency in pregnancy and lactation. Am J Obstet Gynecol 2009; 201
An Appeal o Looking for 2 residents with interest in OB to pilot group prenatal care next year