PREMATURE SPONTANEOUS RUPTURE OF THE MEMBRANES ASSOCIATE PROFESSOR

PREMATURE SPONTANEOUS RUPTURE OF THE MEMBRANES ASSOCIATE PROFESSOR IOLANDA BLIDARU MD, PHD

DEFINITION PROM = spontaneous rupture of the membranes at any time before the onset of labor, irrespective of the duration of gestation. PROM occurs in approximately 10% of all pregnancies

ETIOLOGY The etiology - unknown The fetal membranes → amnion + chorion, directly opposed to maternal decidua The amount of physical stress tolerated by the membranes decreases as pregnancy progresses.

ETIOLOGY Maternal associated conditions ♦ multiple previous pregnancies ♦ cervical incompetency ♦ urinary tract infections vaginal infections: Trichomonas vaginalis, C. trachomatis, N. gonorrhoeae, beta-hemolytic streptococci ♦ sexually transmitted diseases ♦ familial history of PROM ♦ nutritional deficit, cigarette smoking, heavy work

ETIOLOGY Fetal associated disorders twin pregnancy abnormal presentations hydramnios placenta praevia

DIAGNOSIS Symptoms → the key to diagnosis. a sudden gush of fluid or continued leakage. a persistent trickle → a small tear or perforation.

DIAGNOSIS Additional useful symptoms: 1. color + consistency of the fluid 2. the presence of flacks of vernix 3. reduced size of the uterus 4. increased prominence of the fetus to palpation

DIAGNOSIS Examination with a sterile speculum p. H tested with nitrazine paper (AF→ p. H=7, 0 -7, 25) cervical secretions for culture fern test (air-dry a drop of the fluid on a slide ► arborization) Nile blue sulfate staining of fetal cells + cervical aspect (degree of effacement and dilatation) check for cord prolapse determination = L/S ratio, phosphatidylglycerol (after 34 th week)
. Laboratory tests maternal")
DIAGNOSIS of AMNIONITIS Physical examination → signs of infection (fever, tachycardia). Laboratory tests maternal leukocytosis (> 16, 000), amniotic fluid C-reactive protein measurements, aerobic or anaerobic culture. US examination → fetal size.

Differential diagnosis urinary incontinence vaginitis amnio-chorial pouch rupture decidual endometritis

PROGNOSIS Maternal risks Intrauterine infection = a serious complication. Intrauterine infection ► defined as the presence of a positive amniotic fluid culture regardless of the presence or absence of clinical evidence of infection Amnionitis may be more common at 23 to 31 weeks gestation than at 32 to 34 weeks.

PROGNOSIS Fetal and neonatal risks Infection - a major complication → congenital pneumonia, sepsis or meningitis. cord prolapse particularly before to 26 weeks. Preterm birth - the most important risk.

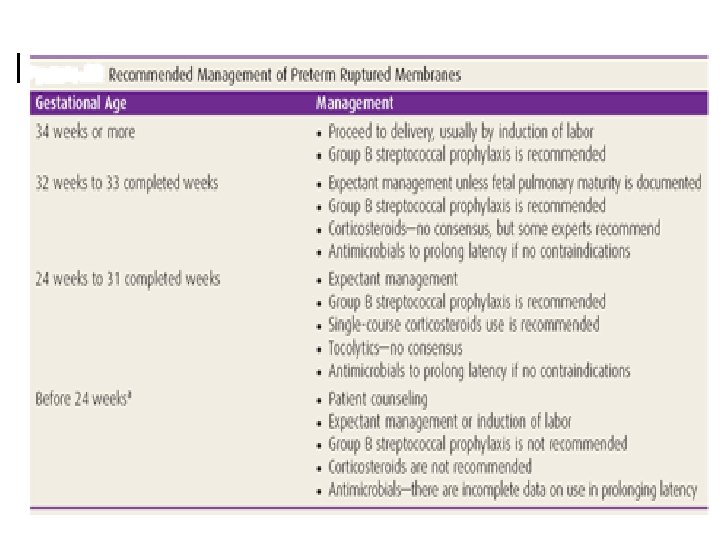
TREATMENT Differences of opinions Ø nonintervention may be more beneficial for both preterm and term fetuses than attempts to deliver. Ø delivery should be induced within a reasonable interval (usually no more than 8 -12 hours) if GA > 34 weeks or if the fetus is mature according to physiologic maturity tests.

If intervention is selected, the following recommendations have been helpful GA > 36 weeks, fetal weight >2, 5 kg, if the latent period exceeds 8 -12 hours, induction by oxytocin infusion. GA= 34 -36 weeks: induction of labor GA = 24 -34 weeks, fetal weight 500 -2000 g if evidence of lung maturation or chorioamnionitis, labor induction; if no evidence of amnionitis, bed rest; corticosteroid drugs (for lung maturation), antibiotics. GA < 24 weeks: very little chance of fetal salvage, considerable maternal risk.

TREATMENT Contraindications to induction à abnormal fetal presentations à feto-pelvic disproportion à uterine scars Cesarean section labor does not progress fetal distress abnormal presentation prolapsed cord
- Slides: 16