PRELABOR RUPTURE OF MEMBRANES PROM Dr Vishal Chaudhari
 Dr Vishal Chaudhari")
PRELABOR RUPTURE OF MEMBRANES (PROM) Dr Vishal Chaudhari

• DEFINITION: • Spontaneous rupture of the membranes any time beyond 28 th week of pregnancy but before the onset of labor • TERM PROM : after 37 weeks • Preterm PROM : Before 37 weeks

• Prolonged Rupture of membranes : Rupture of membranes for > 24 hours before delivery • Incidence : 10% of all pregnancies

Normal events


CAUSES 1. 2. 3. 4. 5. 6. Increased friability of the membranes Decreased tensile strength of the membranes Polyhydramnios Cervical incompetence Multiple pregnancy Infection—Chorioamnionitis, urinary tract infection and lower genital tract infection 7. Cervical length < 2. 5 cm 8. Prior preterm labor 9. Low BMI (< 19 kg/m 2).

Diagnosis • Classic clinical presentation: sudden "gush" of clear or pale yellow fluid from the vagina. • Differentiate from : 1. Hydrorrhea gravidarum—a state where periodic watery discharge occurs …probably due to excessive decidual glandular secretion 2. Incontinence of urine

Confirmation of diagnosis • Per Speculum examination: inspect the liquor escaping out through the cervix • Leakage of amniotic fluid from the cervical os • Pooling in the vaginal fornix is pathognomonic • Collect the fluid for tests

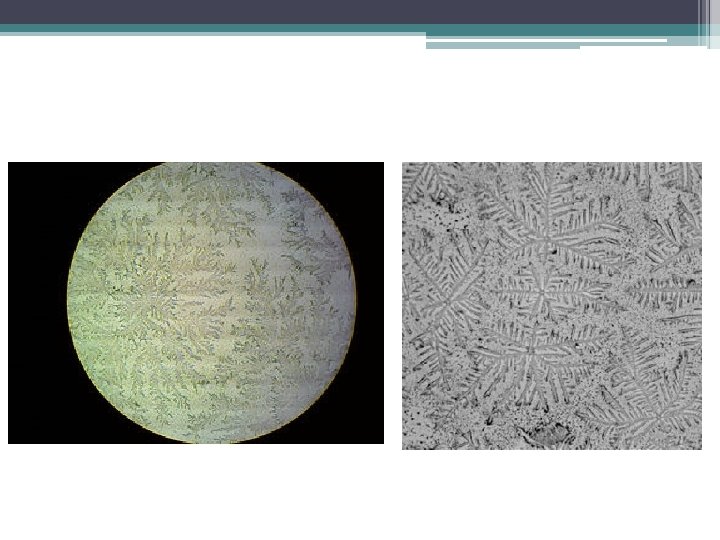
Tests for fluid 1. Detection of p. H - by litmus or Nitrazine paper. p. H in pregnancy- 6 -6. 2 Normal p. H – 4. 5 -5. 5 p. H of Liquor : 7 -7. 5 Nitrazine paper turns from yellow to blue at p. H > 6; 2. Microscopy : characteristic ferning pattern when a smeared slide is examined under microscope;

3. Centrifuged cells stained with 0. 1% Nile blue sulfate showing orange blue coloration of the cells (exfoliated fat containing cells from sebaceous glands of the fetus) 4. Amni. Sure—A rapid immunoassay is accurate 5. Ultrasonography: 50 to 70 % of women have low amniotic fluid volume (AFI), Fetal well being
: A negative fetal fibronectin result strongly supports")
Newer tests • Fetal fibronectin (f. FN): A negative fetal fibronectin result strongly supports absence of membrane rupture, but a positive result only indicates disruption of the interface between chorion and decidua, which can occur with intact membranes • Alpha-fetoprotein (AFP) in vaginal secretions suggest the presence of amniotic fluid
; Urine High vaginal")
INVESTIGATIONS 1. 2. 3. 4. Full blood count; C-reactive protein (CRP); Urine High vaginal swab for culture (specially for Gr. B Streptococcus) 5. Ultrasonography for fetal biophysical profile 6. Cardiotocography for nonstress test (NST)

Complications • In Term PROM labor starts in 80– 90% of cases within 24 hours. • PROM is one of the important causes of preterm labor and prematurity • Chance of ascending infection is more if labor fails to start within 24 hours. Liquor gets infected (chorioamnionitis) and fetal infection supervenes.

Complications • Cord Prolapse- especially when associated with malpresentation, polyhydramnios • Dry labor- Continuous escape of liquor for long duration • Placental abruption – Polyhydramnios , sudden gush /drainage of liqour

Complications • In Preterm PROM - Fetal pulmonary hypoplasia , when associated with oligohydramnios • Neonatal sepsis • RDS • IVH In Preterm PROM • NEC

Complications • • • Chorioamnionitis Placental abruption Retained placenta Endometritis Maternal sepsis

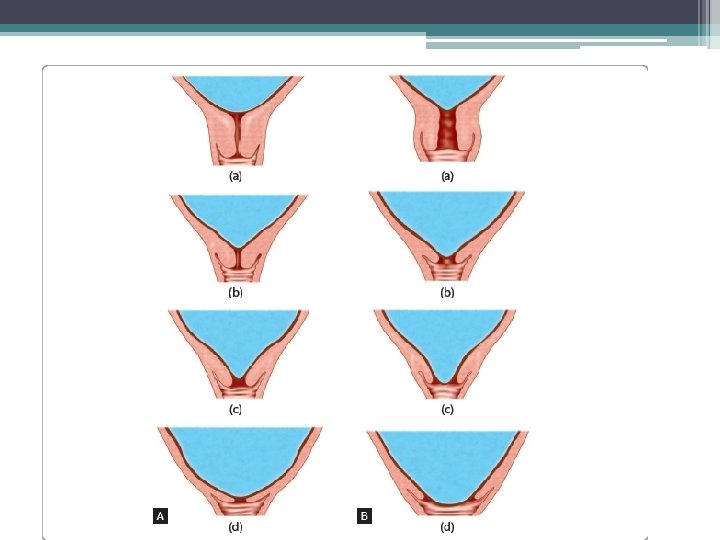
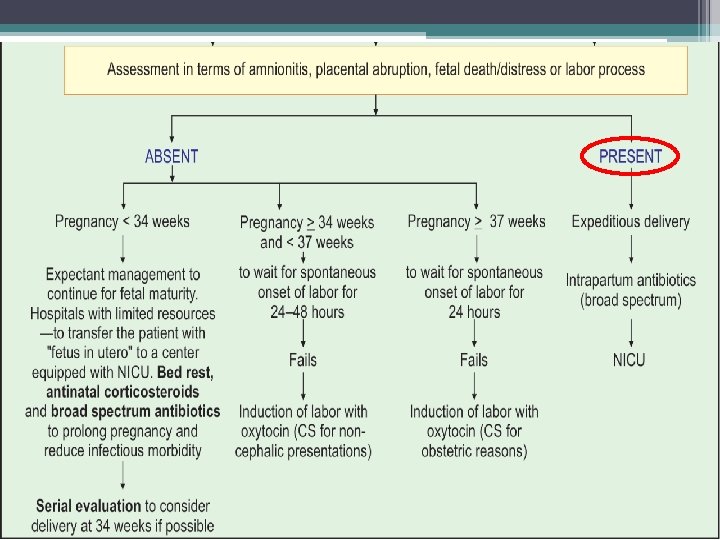
MANAGEMENT • Aseptic examination – confirm diagnosis , state of cervix- Bishop score , • Confirm Gestational age • Diagnosis of labor • Maternal Temperature , Pulse , FHR monitoring • Fetal assessment : Gest. age , weight , Pulmonary maturity

MANAGEMENT • Prophylactic antibiotics : to minimize maternal and perinatal risks of infection • Intravenous ampicillin, amoxicillin or erythromycin for 48 hours • Followed by - oral therapy for 5 days

MANAGEMENT • Use of corticosteroids to stimulate surfactant synthesis against RDS in preterm neonates is advised. • Dexamethasone – 6 mg 12 hourly , 4 doses • Betmethasone – 12 mg 24 hours apart • Combined use of antibiotics and corticosteroids has reduced the risks of – neonatal RDS, IVH and NEC

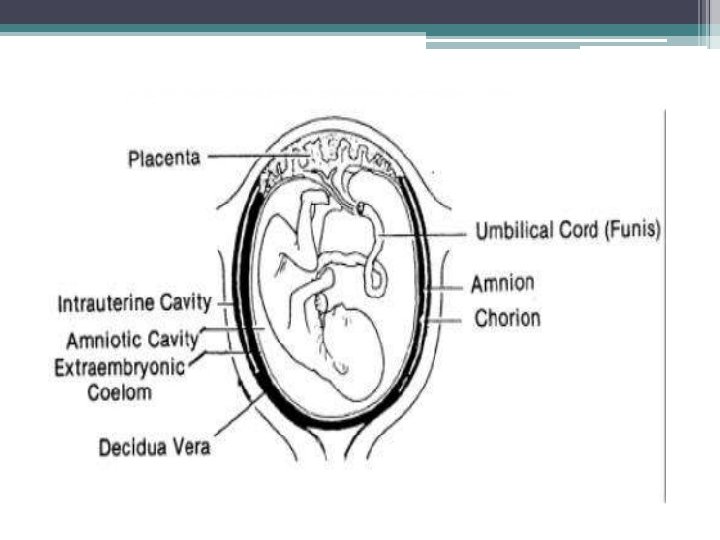
Chorioamnionitis • Chorioamnionitis is a bacterial infection that occurs before or during labor. • The name refers to the • Chorion (outer membrane) and • Amnion (fluid-filled sac). • Chorioamnionitis occurs when bacteria infect the chorion, amnion, and the fluid around the fetus (amniotic fluid).

Causes • Usually develops due to an infection • Bacteria that are normally present in the vagina ascend into the uterus • Most common causes of chorioamnionitis E. coli, group B streptococci, and anaerobic bacteria

Risk Factors • History of previous premature birth • Presence of premature labor • PSROM prior to onset of labor • Prolonged rupture of membranes • young maternal age • multiple vaginal examinations during labor (only in women with ruptured membranes)

Clinical feature • High temperature and fever • Rapid heartbeat (The fetus might also have a rapid heartbeat. ) • Sweating • A uterus that is tender to the touch • A discharge from the vagina that has an unusual smell (Lochia/ vaginal discharge)
 • Abdominal pain •")
Diagnosis Clinically • maternal pyrexia (fever >37. 5– 38 C) • Abdominal pain • Uterine tenderness, • Foul vaginal discharge, • Maternal tachycardia (>100 beats/min), • Fetal tachycardia (persistent elevation of fetal heart rate >160 - beats/min)
 • High levels of C-reactive")
Laboratory tests • CBC Maternal leucocytosis (>15, 000/mm 3) • High levels of C-reactive protein (CRP) • An amniocentesis : a small amount of amniotic fluid is removed for testing if the amniotic fluid has a low concentration of glucose (sugar) and a high concentration of white blood cells and bacteria.

Complication • Infections in the pelvic region and abdomen • Endometritis (an infection of the endometrium, the lining of the uterus) • Thrombosis and embolism • Sepsis • High morbidity and mortality rates

Treatment • Ampicillin 2 gm IV every 6 hours, plus • Gentamicin 1. 5 mg/kg IV every 8 hours • Followed by a postpartum dose of each antibiotic at the appropriate drug-specific interval. • For cesarean delivery: Add metronidazole 500 mg IV

Alternative • Clindamycin 900 mg IV every 8 hours, plus • Gentamicin 1. 5 mg/kg IV every 8 hours • Followed by a postpartum dose of each antibiotic at the appropriate drug-specific interval.
- Slides: 35