Pregnancy as Viewed by Rheumatologist Dr Ahmed Negm

Pregnancy as Viewed by Rheumatologist Dr. Ahmed Negm, MD Lecturer of Rheumatology, PM & Rehab.

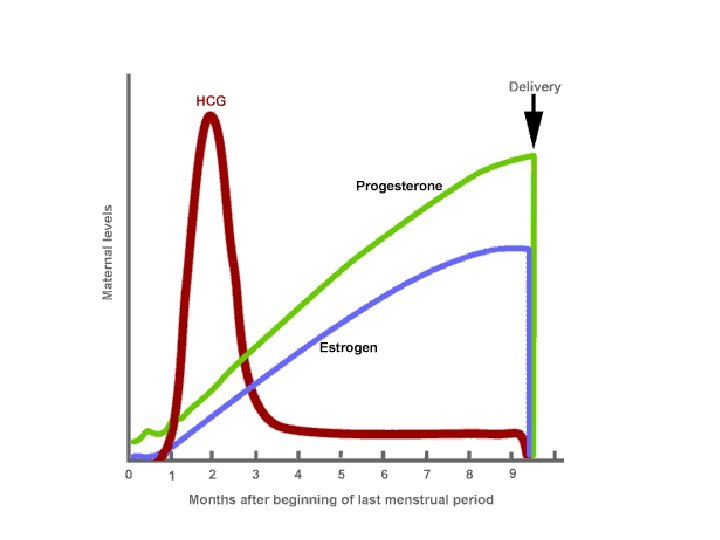
Pregnancy as an Endocrine Disorder - Normal pregnancy induces profound multisystemic changes similar in magnitude to those seen in many welldefined endocrine disorders. - However, unlike other endocrine conditions, pregnancy may affect up to half of the normal population.

Maternal changes by Hormones Anatomy Physiology Metabolism Immune system

Multisystemic Condition MSk Renal Skin Pregnancy? Rheumatic Disease? Hematologic CNS

Hormone-induced changes Pregnancy related symptoms A possible rheumatic disease

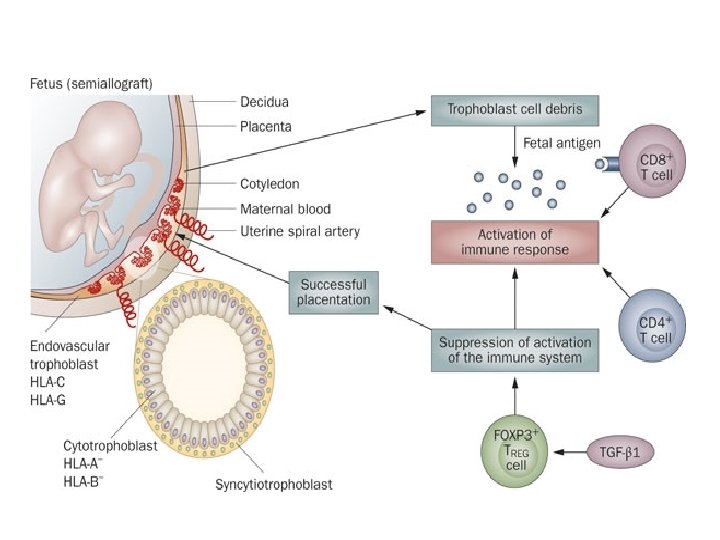
Maternal Immune tolerance to fetal Antigen In order for a pregnancy to be successful, the mother must tolerate the fetus, which is a hemi-allograft. some degree of immunosuppression is necessary

What happens to the immune system? Theories include variations in: - cytokine levels -alterations in levels of expressed adhesion molecules - attenuation of natural killer cell activity These changes in the immune system during pregnancy may modify disease activity of some rheumatologic conditions.

RHEUMATIC DISEASES DURING PREGNANCY Disease Activity during pregnancy RA Remits in 70%-80% of cases SLE Stable or worsens. Active renal disease is particularly problematic Ps. A Generally improves SSc Limited data Dermatomyositis Limited data

RHEUMATOLOGIC MANIFESTATIONS OF PREGNANCY

MUSCULOSKELETAL MANIFESTATIONS OF PREGNANCY ligamentous laxity Position of the gravid uterus shifts the center of gravity, causing hyperlordosis, which contributes to the mechanical strain on the back and sacroiliac joints. alteration in COG MSK Symptom s weight gain Widening of the symphysis pubis to permit transvaginal passage of the fetus. soft tissue edema In 80%, commonly in last 8 weeks Tenosynovial and Nerve entrapment Additional stress on joints: a 20% increase in weight during pregnancy can increase the force on a joint by as much as 100%.

Low-Back and Pelvic Pain • Up to 72%. • Risk of low-back pain increases with: - Advancing maternal age - History of previous pregnancy-related LBP - Multiparity - Higher body mass index - History of hypermobility • • • True Lumbar Radiculopathy 1% Cauda equina syndrome (1/10000) Pelvic girdle pain of pregnancy is common Syndrome of osteitis pubis Osteitis condensans ilii

Hip Pain Transient osteoporosis of the hip Usually in 3 rd trimester. Self limited OP “Transient!” Localized OP “Hip!” Recover in 6 months Usually unilateral Typical presentation is the onset of acute hip pain worsened by weight bearing and relieved with rest • Prognosis is Good “if recognized!!” • • • Avascular necrosis of the hip • Clinical presentation may be similar TOPH • Prognosis is variable, and postpartum core decompression or hip replacement may be necessary • MRI can distinguish both • Safe in pregnancy

Tenosynovitis • de Quervain tenosynovitis

Arthralgia and Arthritis • Healthy women may also complain of small joint pain during pregnancy, raising the question of inflammatory disease, such as SLE or RA Normal 10% Arthralgia Arthritis 17% 74%
 Vascular Changes • Spider")
CUTANEOUS MANIFESTATIONS OF PREGNANCY Melasma (chloasma or mask of pregnancy) Vascular Changes • Spider angiomas and telangiectasias • Nonpitting edema • Palmar erythema
 • A common pregnancy induced")
CUTANEOUS MANIFESTATIONS OF PREGNANCY postpartum hair loss (telogen effluvium) • A common pregnancy induced dermatologic change suggestive of connective tissue disease Nail Changes • Onycholysis • Grooving • Subungual hyperkeratosis

Erythema Nodosum • • Acute nodular erythematous eruption on the extensor aspect of the lower legs Septal panniculitis Common causes include streptococcal infection, tuberculosis, drugs (including oral contraceptives), sarcoidosis, Behcet syndrome, and enteropathies. Pregnancy is an uncommon but wellrecognized cause of erythema nodosum, accounting for 2% of cases.

HEMATOLOGIC MANIFESTATIONS OF PREGNANCY Physiologic anemia that may exacerbate or mimic anemia of chronic disease. Gestational thrombocytopenia
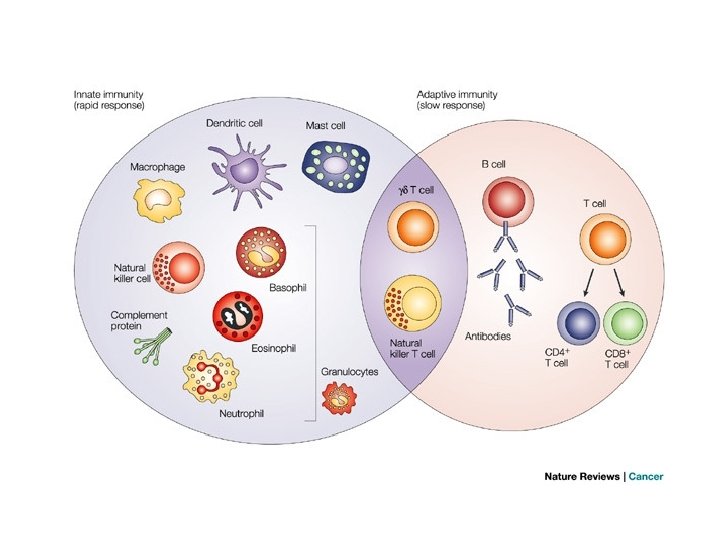

White blood cell • WBC increases slightly during pregnancy because of an increase in circulating neutrophils, and counts markedly increase from 20 to 30, 000/ mm 3 during labor, making WBC count less useful as an indicator of inflammation. • The immune system changes overall during pregnancy to allow maternal tolerance of the fetus, resulting in a decrease in cell-mediated cytotoxic immune responses and an increase in humeral and innate responses.

Serum complement levels • Normal or slightly increased; as a result, these levels are less reliable in diagnosing or ruling out autoimmune disease activity.

Risk of thromboembolism during pregnancy Changes in coagulation system Compression by the gravid uterus, Increased venous stasis Bed Rest Most procoagulant factors increase, including fibrinogen and factors VII, IX, and X, whereas protein S levels decrease

ESR • The increase in fibrinogen is associated with an increase in the erythrocyte sedimentation rate (ESR), so that it is no longer useful as an indicator of inflammation.


Sexual Dimorphism in RA EULAR textbook

Cumulative probability to develop the disease in women with RA over time

Influence of estrogens on important pro- and antiinflammatory pathways in different cell types
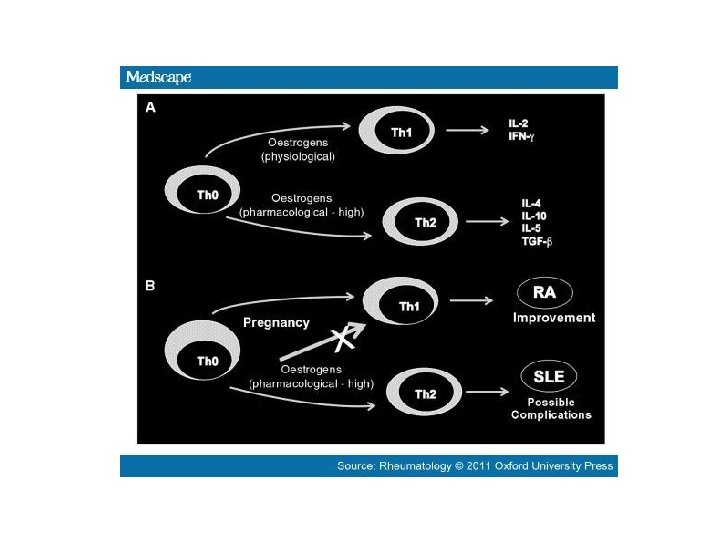

RHEUMATIC DISEASES DURING PREGNANCY Disease Activity during pregnancy RA Remits in 70%-80% of cases SLE Stable or worsens. Active renal disease is particularly problematic Ps. A Generally improves SSc Limited data Dermatomyositis Limited data

TREATMENT PRINCIPLES OF PATIENTS WITH RHEUMATIC DISEASES DURING PREGNANCY • 1. Disease should be in remission or under good control at the time of conception. • 2. Minimize medications or discontinue medications as appropriate. • 3. Treat the disease symptoms, not the diagnosis (e. g. , patient with SLE does not empirically need steroids during pregnancy unless the disease is active).

FOOD AND DRUG ADMINISTRATION USE-IN-PREGNANCY RATINGS

Treatment Recommendations
")
Acceptable medications during pregnancy and lactation Pregnancy Lactation NSAID Yes (avoid after 32 weeks) Yes Sulfasalazine Yes Antimalarials Yes Corticosteroids Yes Cyclosporin Yes probably yes Azathioprine Yes probably yes Mycophenolate No No Methotrexate No No Cyclophosphamide No No Anti-tumor necrosis factor (TNF) No No Rituximab No No

What makes a pregnancy “high risk”? • • • Previous pregnancy with complications Underlying kidney disease Underlying heart disease Underlying lung disease (including pulmonary hypertension) Flare of rheumatic illness A history of previous blood clot the presence of SSA and SSB antibodies IVF (in vitro fertilization) pregnancy with twins, triplets, etc Maternal age over 40 years

Dr. ahmednegm@Hotmail. com

Thank you
- Slides: 40