Practice Guidelines and Computerized Order Entry Brenda S

Practice Guidelines and Computerized Order Entry Brenda S O’Hara, MD President and CEO Leann Hostetler RN Research and Quality Improvement Nurse Fort Wayne Medical Education

The Research Project o Funded by the a private foundation awarded to the Northeast Indiana Innovation Center , (a biotechnology incubator) o Compares two groups of physicians, cardiologists from Fort Wayne Cardiology (FWC) with family practice residents and faculty from Fort Wayne Medical Education Program (FWMEP)

The Research Project o Hypothesis for the study was that compliance with medication guidelines increases when there are reminders imbedded within the medical record o Compliance rates were measured before study, and quarterly for one year o Family Practice residents and faculty took a preand post- study test on the epidemiology and treatment of congestive heart failure, atrial fibrillation and post-myocardial infarction

Why Study Congestive Heart Failure? o FWMEP is very interested in chronic disease management o CHF has high mortality and morbidity and drug treatment can impact this o The number of patients with CHF in our practice was manageable (100) o Guidelines for drug management of CHF are clear and evidence-based

Other Conditions Studied Included Chronic Atrial Fibrillation and Post Myocardial Infarction o The number of patients with these conditions was much smaller than the CHF patients (35 AF patients, 30 MI patients) o These patients were often co-managed with cardiologists so the medication lists were more difficult to keep updated

COE PROJECT Getting It All Started Research Nurse Perspective

COE PROJECT “RULES” 1. Developed By Cardiology Group, Utilizing American College 2. 3. 4. 5. of Cardiology (ACC) Guidelines. Cardiology Group & FWMEP Used Same EMR System Administrator Wrote Programs to Embed Rules into EMR System at Cardiology Group & FWMEP. System Looked At Diagnosis Codes, Medication Sheets, Information Entered Into Chart via Encounter Page. A Red Warning Would Appear In Patient’s Electronic File If a Rule Was Not Followed.

COE PROJECT “RULES” q Congestive Heart Failure q q q Left Ventricular Dysfunction Only If EF >55% And Less Than 1 Year Old, All Rules Were Ignored If Patient Had Creatinine >2 mg/dl, System Did Not Warn for ACE/ARB

COE PROJECT “RULES” o Congestive Heart Failure NYHA Class ACE/ARB Beta. Blocker Diuretic Digoxin (Spironolactone in Class IV only) Class I Yes Yes No No Class III Yes Yes Class IV Yes Yes Non-Specified Yes Yes

COE PROJECT “RULES” q Post-MI q q An MI of any type over 2 weeks old All Post MI Patients Should Be Taking q q q Aspirin Beta Blocker ACE Inhibitor (If EF < 55%) Cholesterol Lowering Agent Clopidogrel – for the First 9 Months Post-MI

COE PROJECT “RULES” q Atrial Fibrillation q Anticoagulation q q q Warfarin – Patients with Heart Disease, or over Age 75 Aspirin – Patients without Heart Disease, up to Age 75 Rate Control q Verapamil, Cardizem, Beta-Blocker, Digoxin, AV Node Ablation

GETTING STARTED q Baseline Patients q q Used 18 -month period prior to starting project Identify Patients for this period using Billing ICD-9 Codes Used Only Patients Seen In Clinic During The 18 -Month Period Chart Review on all Patients q q q Verify Diagnoses Ensure Record as Complete as Possible Exclude Right/Diastolic Heart Failure Patients Review/Correct Medication Lists 379 Patients on original list q 144 Entered into Research Database – eliminated Nursing Home Patients, Deceased Patients, Transfers out of Practice, and Diagnosis not Documented in Chart (Billing Error? )

GETTING STARTED q Research Database q q q Mirror Image Database to our EMR System Restricted Access Operated Similar to “Regular” EMR System Contained Only Baseline Patient Information Baseline Compliance Data Pulled from Research Database q Continuous Identification/Notification of New Patients q q Checking Daily Schedules of Physicians Posted Notice at Nursing Stations Requesting Research Nurse Be Notified of any New Patients Identified With Applicable Diagnoses

GETTING STARTED q Knowledge Training q q Pre-Test Didactic Lectures by Cardiologist Post-Test EMR Medication Entry Refresher Training q Accuracy Important - Medication Entries Triggered Warning Rules q COE Encounter Entry Training q One-on-One Daily Interface by Research Nurse q q Check Residents Daily Schedules Be Available In Clinic Area When Resident Saw Patient

GETTING STARTED q Develop COE Encounter Page q q Joint Effort by FWMEP and Cardiology Group with EMR System Administrator Great Pains Taken To Make It As Simple And Time-Saving As Possible q q Check-Boxes, Drop-Down Menus, Automatic Transferal of Information From Other Areas Of EMR Most Difficult Task Of Project q q EMR System Administrator’s Priorities vs. FWMEP’s Priorities Lack of Understanding of Family Practice Clinic Flow by EMR System Administrators

How the Study was Conducted o A baseline compliance with medication guidelines report was conducted o An example compliance question is “Class III-IV Heart Failure- patient on Aldactone? ” o Guidelines (rules) for appropriate medication prescribing were imbedded in the electronic medical record

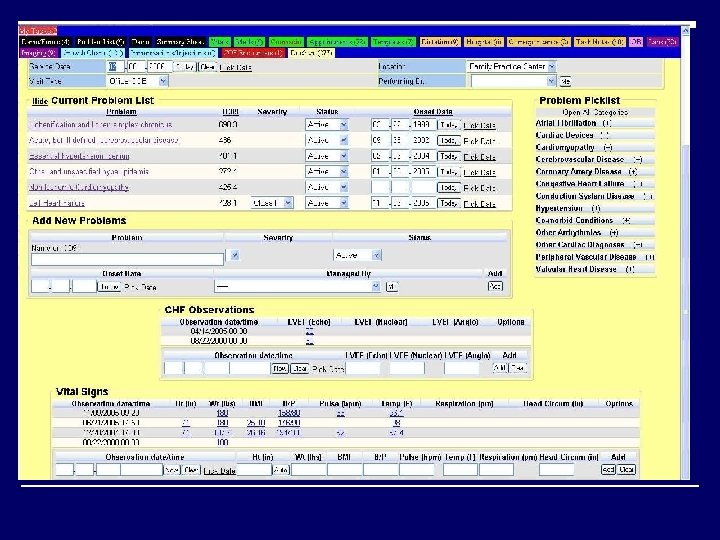
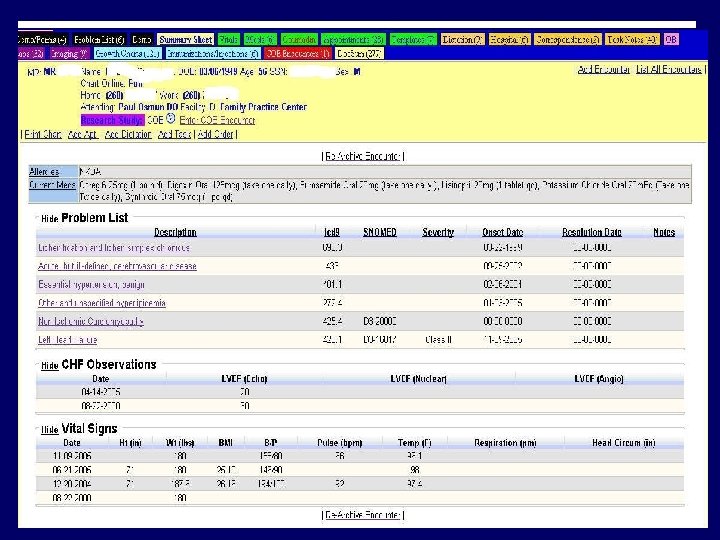
Conducting the Study o When a study participant was seen in the office, they were identified as a study patient and the provider was prompted to open a series of special screens o One screen asked for updated information about the underlying condition- new co-morbidities, most recent echo findings, new devices, etc

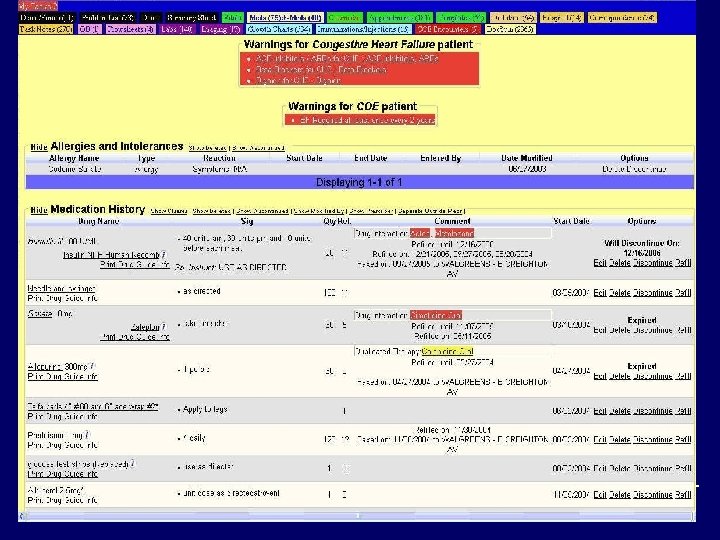
Conducting the Study o The medication screen showed current medications o If a medication was indicated but not on med list and not marked as “allergic” or “intolerant”, the physician received a warning pointing out the discrepancy o Guideline warnings could be dismissed by entering the correct medication or entering an allergy or intolerance o Intolerance categories included “patient can’t afford” or “prescribed but patient won’t take”
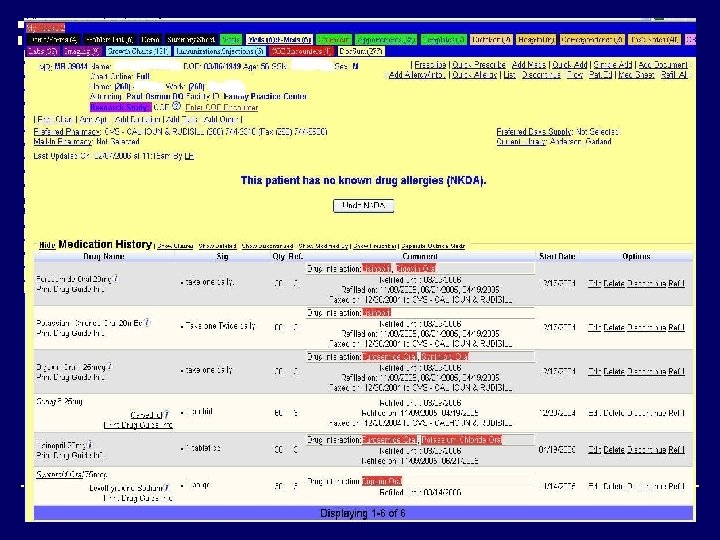

Initial Problems with Study o Medication lists were inaccurate and out of date o Old meds were pushed from former prescribing module into new EMR, carrying over expired and discontinued drugs o Medications prescribed by other physicians were not listed in FWMEP’s med lists o FWMEP providers felt the cardiologist or other physician was “in charge” of medication changes

Solving the Med List Problem o Providers given protected time to update med lists o Frequent reminders to keep med lists current o Research nurse evaluated med lists and queried providers about meds to be discontinued o Research nurse reconciled FWMEP med list with consult letters from cardiologist

Other Study Problems o A few faculty physicians still not comfortable with electronic medication prescribing o Some patients with CHF on problem list actually have right heart failure o Ejection Fractions must be entered manually into the record

Preliminary Results for FWMEP o Percent compliance increased in many categories o Compliance with appropriate drug prescribing following MI increased the most dramatically ( More accurate med lists? ) o Knowledge gains from pre-test to posttest did not occur in a significant number of participants

COMPLIANCE RATES

Preliminary Results o Compared to Fort Wayne Cardiology physicians, FWMEP physicians had compliance percentages higher in four measures, same as in two measures, and lower than in five measures o The lowest compliance rates, FWMEP compared to FWC, were in the conditions with fewer numbers in the study (AF and post-MI)

COMPLIANCE RATES

Questions for the Future o Why weren’t compliance rates 100%? Poor documentation? Resistance to the project? Disagreement with guidelines? Insufficient time? o What was the outcome of the patients? Fewer hospitalizations? If hospitalized, shorter length of stay? Increased quality of life?

Barriers to Compliance Identified in Other Studies o Outpatient clinic workload o Time to remove inapplicable reminders o False alarms o No training o System difficult to use o Accessibility of workstations o Administration benefits more than providers

What Was Missing From Our Guidelines? o Patient education reminders Smoking cessation Moderate Exercise Dietary Guidelines Self-management plan

Questions for the Future? o Can this model be applied to other chronic conditions where the guidelines aren’t as explicit? o Can the process be streamlined and less intrusive to workflow? o Can data such as med lists and test results be shared seamlessly from practice to practice?

Questions for the Speaker?
- Slides: 34