Practical Tools for Prescribing Opioids L Paul Gianutsos

Practical Tools for Prescribing Opioids L. Paul Gianutsos, MD, MPH Associate Director Swedish Family Medicine Residency Cherry Hill Clinical Associate Professor of Family Medicine University of Washington

Drug related deaths in King County 1997 - 2007

Number of unintentional drug overdose deaths United States, 1999– 2007 Source: National Vital Statistics System. Multiple cause of death dataset.

Rate of unintentional drug overdose deaths United States, 1970– 2007 Source: National Vital Statistics System. * Per 100, 000 population.

Percentage of patients and prescription drug overdoses, by risk group, United States MMWR January 13, 2012 / 61(01); 10 -13

Nonmedical Use of Pain Relievers in the Past Year among Persons Aged 12 or Older: Percentages, Annual Averages Based on 2004, 2005, and 2006 NSDUH In 2007, Washington State had the 4 th highest rate of non medical use of prescription opiates in the US

Increased risk of overdose death in Medicaid population in WA TABLE 2. Number and rate of deaths attributed to overdoses of prescription opioid drugs, by Medicaid status — Washington, 2004 – 2007 Status DSHS PRC Non-DSHS No. 758 34 910 Crude rate 14. 8 580. 4 4. 5 Age-adj rate 30. 8 381. 4 4. 0 Age-adj RR 5. 7 (5. 3– 6. 1) 92. 6 (64. 1– 129. 5) Referent Overdose Deaths Involving Prescription Opioids Among Medicaid Enrollees, Washington, 2004– 2007, MMWR, October 30, 2009 / Vol. 58 / No. 42

Sources of prescription opiates among non-medical users 2007 data n n n 56. 5 % obtained free from a friend or relative 8. 9 % bought from a friend or relative 5. 2 % stole from a friend or relative 18. 1 % got the drugs from one doctor 4. 1 % got drugs from drug dealer 0. 5 % bought from Internet. 81. 0 % of users who obtained drugs from a friend or relative for free reported their friend or relative had obtained them from just one doctor. Only 1. 8 percent reported that the friend or relative had bought the drugs from a drug dealer or other stranger.

Elements of Management Have a diagnosis – what is the problem? Negotiate treatment goals with patient before starting opioid therapy Screen for and treat affective disorders Screen for and treat substance use disorders Risk stratify patients before starting opioids Use measurable functional outcomes Agree on the meaning of treatment failure Understand that opioids play a small role overall

Toolkit Universal Precautions Patient Agreements Screening for substance use disorders and risk of opioid misuse Screening for mood disorders A primary care approach to risk stratification Assessing pain and function Urine drug testing Accurate medication conversion table Prescription Monitoring Program Screening for Obstructive Sleep Apnea 4 A model of management Opiate replacement therapy - buprenorphine Exit strategies

Universal Precautions 1. Diagnosis with appropriate differential 2. Psychological assessment including risk of addictive disorders 3. Informed consent 4. Treatment agreement 5. Pre and post-intervention assessment of pain level and function 6. Appropriate trial of opioid therapy 7. Reassessment of pain score and level of function 8. Regularly assess the “Four As” of pain medicine: Analgesia, Activity, Adverse Reactions, and Aberrant Behavior 9. Periodically review pain and comorbidity diagnoses, including addictive disorders 10. Documentation Gourlay, Pain Med 2005; 6(2): 107– 12

Screening for Substance Use Disorders ASSIST – well validated in primary care, measures lifetime and current risk of drugs and alcohol and recommends level of intervention required http: //ww 1. drugabuse. gov/nmassist/ CAGE-AID screens for lifetime risk only, sensitive for dependent level use but not abuse or misuse TICS – Two Item Conjoint Screen, screens for lifetime risk only AUDIT C – well validated alcohol screening for current misuse and dependence

Screen for alcohol and other substance use disorders Available free http: //www. niaaa. nih. gov/Publications/ Education. Training. Materials/

Medication Agreement Essentials Will use opioid only as prescribed Patient understands risks of medication including need for safe storage No early refills and no refills for lost or stolen prescriptions One prescriber, one pharmacy Agree to UDA Opioids will be stopped if the prescriber or patient feel the medication is not effective, for intolerable side effects and for breaches of the agreement

Medication Agreements Address – – – Desired patient-centered, functional outcomes Adverse effects Aberrant behaviors Outcomes that denote a failed trial Exit strategies for failed trials Provide informed consent

SMG Pain Agreement Swedish Intranet

SMG Informed Consent Swedish Intranet

Patient-centered, functional outcomes Treatment Plan Negotiation What does your pain keep you from doing that you most want to do? If it is not possible to get back to 100% with these activities, what improvements would significantly improve your quality of life? What percent reduction in pain would allow you to make these improvements? What, besides medication, would help make these improvements? What medication side effects would be a significant problem for you?

Functional Goals may include: Physical – recreational activities, yard work, household work, employment, childcare, volunteering, hobbies Social – socializing with family or friends, attending religious services, group visits in clinic

Guidelines for Goal Setting Goals must be functional: what would you like to be able to do that you are unable to do now because of pain Being pain-free is not a realistic goal Patients should identify their own functional goals Goals should be realistic and measurable It is often helpful for another source such as a spouse, significant other, caregiver, or family member to verify attempts and achievement of goals
 how")
A Key Question In your own words (but without using the word ‘pain’) how will we know that this medication is working for you? From Mark Sullivan, MD UW Dept of Psychiatry

Goals: Follow up Review the success or failure in achieving goals at each visit New goals should be identified by the patient Consider short term (next visit) and longer term goals Provide encouragement Consider changing or tapering therapy if patient repeatedly fails to achieve goals or maintains a lack of motivation
 Pain Disability Index (PDI) Roland")
Monitoring pain and functional outcomes Brief Pain Inventory (BPI) Pain Disability Index (PDI) Roland Morris Disability Scale Oswestry Disability Index Two Item Graded Chronic Pain Scale Emerging consensus on what constitutes minimally significant improvement : 30% change from baseline Spine 2008; 33: 90– 94

Two Item Graded Chronic Pain Scale Opioid Dosing Guideline for Chronic Non-Cancer Pain, 2010 http: //www. agencymeddirectors. wa. gov/Files/Opioid. Gdline. pdf

Brief Pain Inventory

Urine Drug Testing Means of creating a therapeutic alliance Allows decision making based on data Should be non-judgmental, non-punitive In the clinical setting is not a legal tool requiring chain-of-custody documentation Assists in the identification of patients with a potentially life-threatening primary disease http: //intranet. swedish. org/Swedish. Physician. Division/Chronic. Pain. Management Program. html

Why test 1/3 to 1/2 of patients at risk for misuse of drugs or alcohol are missed on basis of behavior alone Self-report of illicit drug use and misuse of licit drugs is unreliable Adds an objective piece of information regarding the overall health of the patient Consider: diabetic doing SBGM – do we still perform Hgb. A 1 C? Of course.

Mistaken reasons for UDT Legal purposes Throw addicts out of your practice Say “I told you so” then throw them out Catch people lying (then throw them out)
 Confirmatory tests")
Types of UDT Screening tests n n Immunoassay Thin layer chromatography (TLC) Confirmatory tests n n Gas chromatography/mass spectroscopy High performance liquid chromatography
 Fast: 2 - 5 minutes Relatively")
Immunoassays Can be done in the office (POCT) Fast: 2 - 5 minutes Relatively inexpensive ~ $10 -15 Can identify several drugs simultaneously

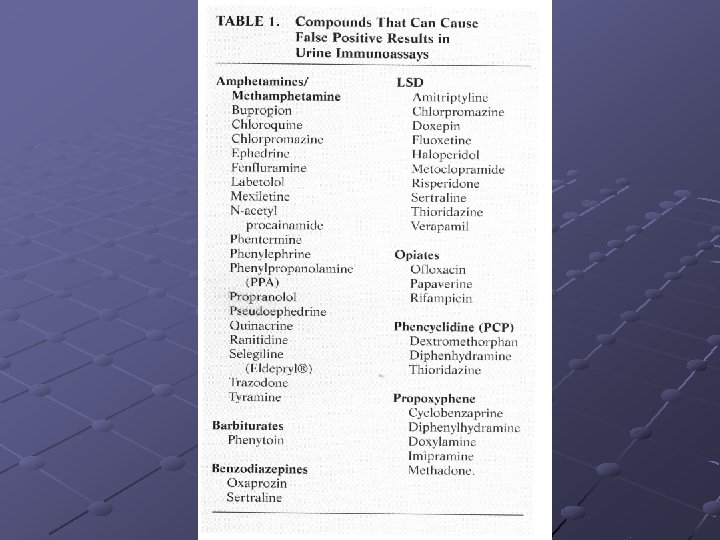
Immunoassays - disadvantages Lower sensitivity and specificity sometimes requires follow-up confirmation testing Cross reactions can cause false positive results Levels of detection may be too high to detect all drug use

GC/MS Gold standard for detection Used to confirm immunoassays Expensive: $35 – 50 per substance ordered

Urine Collect on-site, unobserved We check every patient on chronic opioids at every visit Normal urine characteristics: n n n temp 90 - 100 F p. H 4. 5 - 8. 5 creatinine > 20 mg/dl If tampering is suspected, send urine to lab for confirmation: write UA, suspect tampering

Most drugs can be detected in urine within 1 to 3 days of use • There is no direct relationship between dose and urine drug concentration. • Passive inhalation of smoke or handling contaminated items does not explain a positive test.

Interpretation and Clinical Use of Drug Tests Document and discuss all results with patient Know what you will do with UDA results: have a treatment plan Convey TRUST and SAFETY, you do what you do for the safety of the patient

Aberrant Behaviors Portenoy, RK. Opioid therapy for chronic nonmalignant pain: a review of the critical issues. J Pain Symptom Management 1996; 11: 203 -17

Opioid Misuse Screening Tools ORT SOAPP COMM None are supported by good studies in primary care populations Comparison of tools: Chou et al, The Journal of Pain, 2009 February; 10(2): 131 -146 Gianutsos, Safranek, J Fam Pract. 2008 Sep; 57(9): 609 -10.
 The SOAPP classifies patients")
Screen and Opioid Assessment for Patients with Pain (SOAPP 14) The SOAPP classifies patients as either high or low risk for opiate misuse 14 self administered questions Takes about 5 minutes Butler SF, et al, Pain, 112, 2004, 65 -75

SOAPP 14 operating characteristics

Current Opioid Misuse Measure COMM Identifies patients currently on long-term opioid therapy who may be exhibiting aberrant behaviors associated with misuse of opioid medications. 17 item patient self-assessment Completed in less than 5 minutes Validated with a group of approximately 500 chronic pain patients on opioid therapy in a specialty pain clinic Helpful for documenting decisions about the level of monitoring planned for a particular patient or justifying referrals to specialty pain clinic. Score < 9 predicts low risk of misuse. Butler SF, et al, Pain 130 (2007) 144– 156

COMM operating characteristics

Equianalgesic opioid doses AMDG Opioid Guidelines

Washington State Prescription Monitoring Program

Obstructive Sleep Apnea 2 – 4% prevalence in general adult population Higher in chronic pain populations due to higher rates of obesity, diabetes and CVD Opioids cause central sleep apnea and other sleep disordered breathing Opioids will increase the risk of respiratory depression especially in patients already at risk

Sleep apnea screening Variety of screening tests for OSA Only Berlin and Wisconsin questionnaires validated in general primary care population Berlin is complicated Wisconsin unavailable

Preoperative screening STOP Bang questionnaire 8 yes/no items 3 or more positive responses = high risk of OSA Only validated in preoperative populations n n n n Snore loudly Tired during the day Observed apnea high blood Pressure BMI ≥ 35 Age ≥ 50 Neck circumference ≥ 40 cm Gender male

Screening tests compared Berlin STOP Bang Sensitivity Specificity 55 - 80 50 - 97 93 43 Screening patients without history of sleep disorder. Detecting moderate OSA (AHI 15 - 29) STOP Bang is 100% sensitive for severe OSA Can J Anesth (2010) 57: 423 -438

Consider Naloxone Washington State’s “ 911 Good Samaritan Law” Anyone at risk for having an overdose or witnessing one can be prescribed Narcan. They are allowed to possess and administer Narcan to a person believed to have had an overdose.

Patient assessment 4 A Model Analgesia Adverse events Activity Adherence

Analgesia Assessment Document location and severity of pain at every visit Assess pain intensity at baseline and with changes in opiate dose Use a standardized assessment scale n n Brief Pain Inventory Two Item Graded Pain Scale

Adverse effects Constipation, nausea Dysphoria, euphoria, sedation, myoclonus, headache, depression, anxiety Increased pain: Opioid Induced Hyperalgesia (OIH) Addiction Amenorrhea, possible hypogonadism in males Itch Sexual dysfunction, decreased libido Urinary retention

Activity Use a standardized assessment scale n n Brief Pain Inventory Two Item Graded Pain Scale Ask: What are you doing now that you were unable to do previously? Review goals ADLs, employment, recreational and social activities Can you document improved function? Is there evidence of deteriorating function? MVA, DWI, DV, divorce, unemployment Do you need collaborative information from spouse, SO, caregiver?

Adherence Is the patient able to control use or are there aberrant drug related behaviors? early refills repeated, unauthorized dose escalations lost or stolen Rx multiple ER visits or other prescribers failure to comply with non-drug therapies multiple calls to clinic positive UDAs

Detecting addiction using the 4 As Loss of control and use despite harm are hallmarks of addiction Activity = Function The patient’s insistence on continued use despite deteriorating function or side effects without demonstrated benefit characterizes use despite harm Adherence = Control early refills, unsanctioned dose escalations, lost and stolen Rx, multiple prescribers despite agreement , positive UDA suggest loss of control

Mood Disorders in Chronic Pain Review by Blair and Katon, et al, Depression and pain co morbidity: a literature review. Arch Int Med. 2003; 163: 24332445 42 studies across settings, 1966 - 2002 Over 14, 000 pain patients 50% of chronic pain patients have clinically significant depression n n Depression is associated with greater pain complaints and increased disability Depression reduces compliance with pain treatment recommendations

Which comes first, pain or depression? 200 patients with chronic low back pain 59% met DSM III criteria for at least one psychiatric diagnosis: depression and anxiety were the most common 51% Axis 2 disorder Anxiety disorders preceded pain (95%); depression (54%) Polatin PB et al, Psychiatric illness and chronic back pain. Spine, 1993, 18(1): 66 -71

Does depression affect the transition from acute to chronic pain ? Pincus et al, Spine, 2002; 27: E 109 - E 120 Systematic review 6 methodologically sound studies (out of 25 trials) Several hundred patients overall Variety of psychometric and pain scoring systems examined

Depression is related to development of chronic low back pain “There is strong evidence for the role of distress/depressive mood in the transition from acute to chronic low back pain. The effect size was moderate, but exceeded that of physical clinical factors measured in the samples. ”

A Longitudinal Prospective Study of Industrial Back Injury Reporting Prospectively evaluated 3020 volunteers at Boeing plant to assess risk factors that predisposed workers to file industrial back injury claims 279 subjects reported acute back problems Most predictive factors were: job dissatisfaction and distress on scale 3 (hypochondriasis) of MMPI Bigos et al. Clin Orthop Relat Res 1992

Psychiatric assessment Depression: The Patient Health Questionnaire PHQ – 9 http: //www. depression-primarycare. org/ Anxiety: Generalized Anxiety Disorder Score GAD-7 Arch Intern Med. 2006; 166: 1092 -1097 Bipolar Disorder: MDQ

Exit Strategies Lack of improvement at ~ 120 mg morphine/day equivalents with either insufficient pain relief or lack of functional improvement: consider tapering opioids and referral to specialist Fails to comply with other treatment requests: PT, exercise, counseling, group visits Aberrant behaviors

Opioid tapers Methadone 5 mg q 3 -4 days 10% weekly Stop opioid prescribing without taper for illicit opioid use, diversion or fraud Ending opioid prescribing for a patient does not necessarily mean stopping care for a patient: there are multiple methods of pain control including exercise, PT, chiropractic, massage, acupuncture, integrative medicine, behavioral techniques, neuromodulation, non-opioid analgesics

Opiate Replacement Therapy Buprenorphine is approved for use by primary care physicians for treatment of opiate addiction Highly effective at decreasing opiate misuse Effective for pain management Requires 8 hour CME course http: //buprenorphine. samhsa. gov/pls/bwns /training

Recommended Opiate Prescribing Guidelines Know what you are treating n n n Opioids not recommended for fibromyalgia Ann Rheum Dis 2008; 67: 536– 541. Opioids are 2 nd line drugs for neuropathic pain Am J Med 2009 122, S 22–S 32 Evidence is limited regarding benefit of opioids for chronic low back pain Ann Intern Med. 2007; 146: 116 -127. Do not prescribe for new patients without obtaining medical records Assess risk of opiate misuse and risk stratify patients Contraindications include: n n Active substance use disorder Serious or uncompensated personality, mood and thought disorders Max dose 120 mg morphine equiv/day Consider every new start on opioids a trial and stop if not effective. Stop opiates for failure to comply with other treatment requests or for aberrant behaviors Refer to chemical dependency treatment for substance use disorders Use universal precautions

Risk Stratification Risk Low Moderate High Psychiatric No history of psychiatric disorder Stable, well compensated mood disorder Unstable mood, psychotic or personality disorder Poor adherence to therapy Chronic benzodiazepines Addiction No personal or family history of addiction Past history of addiction or family history of addiction Active addictive disorder including non substance use disorders Medical No medical comorbidities Stable comorbidities Unstable comorbidities Poor adherence to therapy. Social Good social support Social discord Isolated Destructive social network Litigation Activity Active engagement in work, recreation or hobbies Unemployment due to compensable injury No satisfying work or recreation Pain Etiology Clear etiology Uncertain etiology Unclear etiology with non anatomic distribution of pain Indications FM, IBS Adapted from Stephen Passik

What were the ratings for the pain education initiative? • Content & relevancy of program rated 4. 49 on 5 point scale • Value of topic was 4. 37 • Format rated 4. 26

Medical students perception of pain in the primary care? • Do not like dealing with pain • Particularly chronic

Medical Student Perceptions Chronic Pain 75% Negative 11% Positive 13% Neutral
- Slides: 70