Practical medical mycology Lab 7 identification of fungi

ﺑﺴﻢ ﺍﻟﻠﻪ ﺍﻟﺮﺣﻤﻦ ﺍﻟﺮﺣﻴﻢ Practical medical mycology Lab 7 identification of fungi ( part 2) Microsporum Cryptococcus neoformans Histoplasma capsulatum Coccidioides immitis Blastomyces dermatitidis

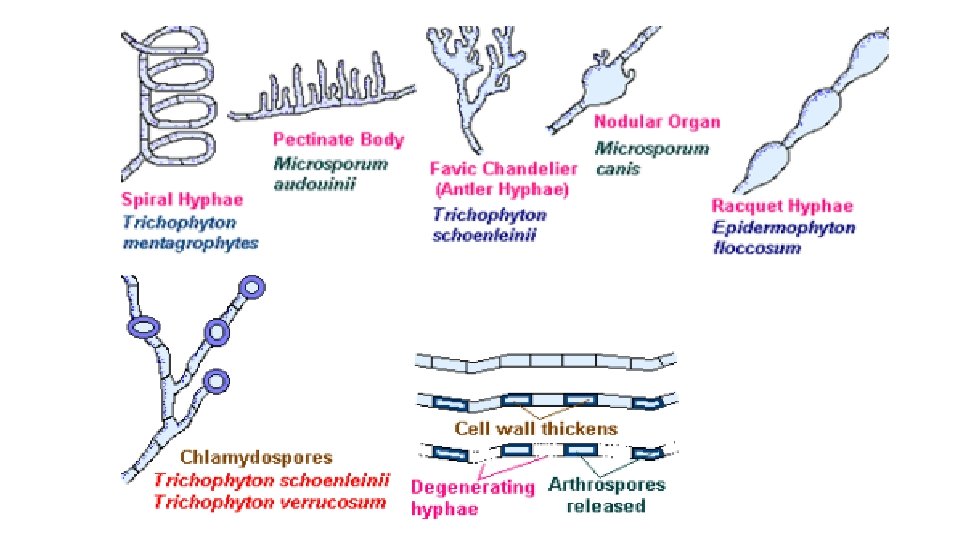
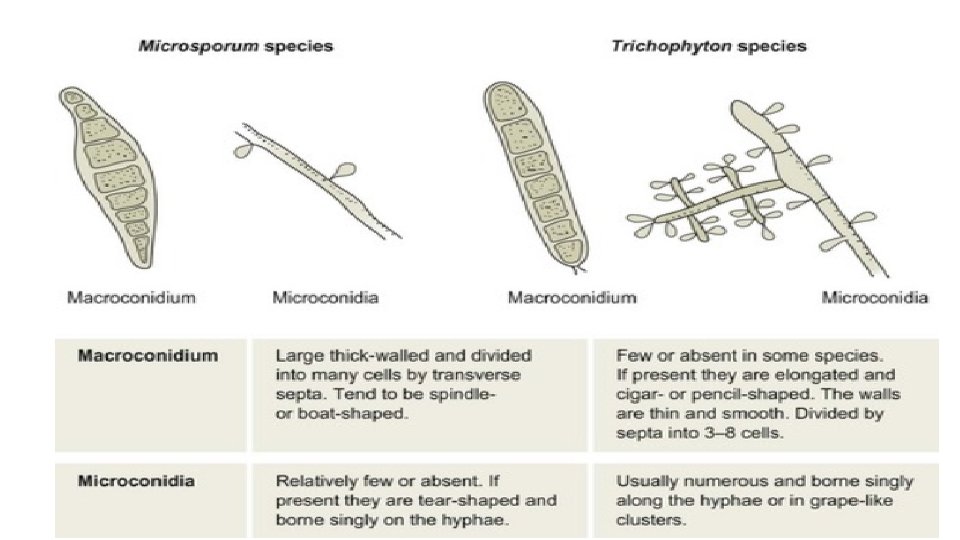
Microsporum • The genus Microsporum is characterized by fusiform or spindle-shaped macroconidia, often with thick, rough, or spiny walls. • The rough nature of spines may be difficult to demonstrate in some cultures and may be seen only on the tip of the conidium. • Macroconidia and colony morphology are used to identify the genus and species. • Although microconidia may be produced, they do not aid in identification.

• Most Microsporum species perforate hair in vitro. • Examination of tinea capitis or of cultures derived from it, when illuminated by Wood’s light, demonstrate a bright yellow-green fluorescence with M. canis. M. ferrugineum also has yellow-green fluorescence, while M. Audouinii produces a silver fluorescence.

Microsporum audouinii • Colony: Growth is slow, with glabrous to velvety dense mycelium, wrinkled, with a radiating edge. • Surface: Color is white-gray, tan, or rust-buff. • Reverse: peach to salmon color. • Microscopic: Macroconidia are rare and poorly developed. When seen they are similar to those of M. canis with terminal spine-like projections, pectinate hyphae, and chlamydospores. M. audouinii is differentiated from other Microsporum species by its poor growth on rice grains.

Microsporum gypseum • Colony: Microsporum gypseum rapidly covers the agar surface with floccose to powdery growth that may become pleomorphic. • Surface: Cinnamon-buff. • Reverse: May be colorless, buff, deep mahogany- brown, or variable. • Microscopic: Abundant clusters of macroconidia are produced: clavate or cylindrical to fusiform-shaped,

Cryptococcosis • The infections produced by the ubiquitous encapsulated yeast Cryptococcus neoformans which is usually acquired by inhalation. • immunosuppressed patients • Localized in The lung • Primary pulmonary Infection (bronchitis) • cough, low-grade fever and pleuritic pain • Soil, bird droppings

Cryptococcosis : Diagnosis • India ink smear or nigrosin stain of the CSF sediments will reveal a capsule, double cell wall. • Fungal culture- mostly done with CSF deposit, sputum and urine. • These are cultured on SDA. • C. neoformans colonies are smooth, convex and yellow or tan on solid media. • It produces brown colonies on bird seed agar (melanin production).

• It can also be identified by biochemical tests, eg. , API. (3 days system) • There also DNA probes that are available for diagnosis. • Cryptococcal antigen test- this a latex agglutination test that can be performed on CSF and serum that is >90% specific. • Histopathology- Methenamine silver or Periodic acid- Schiff staining show a yeastlike organism with narrow based buds. • Mayer’s mucicarmine stain will stain the capsule rose red.
 • India ink")
Identification of Crypto. spp • Urease (positive for Crypto sp. ) • India ink (positive for Crypto sp. )
 stained tissue section of lung showing typical encapsulated yeast cells")
Grocott’s methenamine silver (GMS) stained tissue section of lung showing typical encapsulated yeast cells of C. neoformans.

CRYPTOCOCCOSIS : culture Mucoid colonies of C. neoformans Bird seed agar plate showing the typical brown colour effect seen with C. neoformans.

Canavanine-glycine-bromothymol blue medium can be used to distinguish C. neoformans var. neoformans (medium remains yellow) from C. neoformans var. gattii (medium turns a deep blue in 2 -3 days).
 H. capsulatum var. capsulatum (North America, Mexico) H. capsulatum")
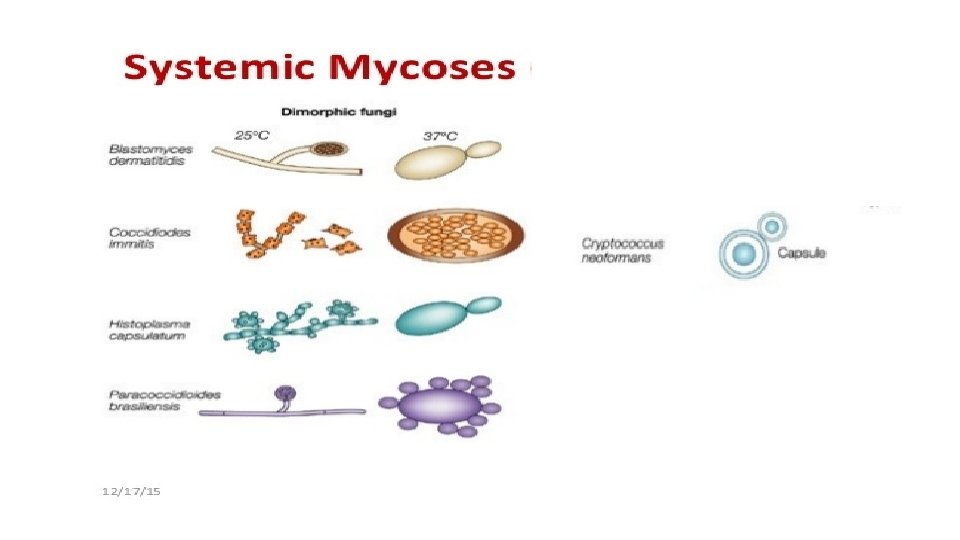
Histoplasma capsulatum Histoplasmosis (systemic mycoses) H. capsulatum var. capsulatum (North America, Mexico) H. capsulatum var. duboisii (Tropical areas of Africa)

Histoplasma capsulatum Yeast form Round and oval budding yeast The yeast phase is inhibited by cyclohexamide GMS stain of lymph node showing blastoconidia of H. capsulatum Mycelial form Hyaline septate hyphae Pear-shaped microconidia Tuberculate macroconidia of H. capsulatum (LPC)

Histoplasma capsulatum Laboratory diagnosis 1. Direct examination KOH wet mount of sputum showing blastoconidia of H. capsulatum Bone marrow aspirate with macrophage containing numerous blastoconidia of H. capsulatum

• Culture: Definitive diagnosis is by culture and is done for up to 6 weeks at 300 C in brain heart infusion agar, blood, antibiotics and cyclohexamide. Fungus from culture is confirmed using a probe for ribosomal DNA. • Organism detection: This is the detection of polysaccharide antigen in urine and blood. • Serology: (Complement fixation test Immunodiffusion (ID) test) • Histochemical: stains can allow rapid identification of fungus from tissues and body fluids.
 pulmonary infection 60% in normal host pulmonary")
Coccidioides immitis MCoccidioidomycosis MAsymptomatic MProgressive (systemic mycoses) pulmonary infection 60% in normal host pulmonary infection in immunocompromised patients

Coccidioides immitis MIn tissues or body fluids, C. immitis exists as spherules (10 -80 um ), which contain endospores (2 -5 µm) KOH wet mount of sputum showing spherule and endospores of C. immitis

Mycelial form Coccidioides immitis MHyaline septate hyphae MBarrel-shaped arthroconidia that alternate with empty C. immitis on PDA, 300 C (Lactophenol cotton blue ) cells(

Coccidioides immitis Spherules

Coccidioides immitis Laboratory diagnosis M Culture Isolation of the organism- definitive diagnosis is by culture or the identification of fungal elements within clinical specimens. • There is minimal risk to the medical personnel because infection is not transmitted from primary specimen. • Stains such as silver, periodic acid –Schiff or H&E will reveal spherules • C. immitis grows on standard microbiological media in aerobic conditions and typically takes the form of a white mold at around 5 -7 days. At this point, it is highly infectious. • Unlike the spherule, the mycelial form is not unique, and identification is made by reference laboratories either antigenic detection or by the detection of specific ribosomal RNA.

Blastomyces dermatitidis Yeast form S Broad base budding yeast cells S The yeast phase is inhibited by cycloheximide Mycelial form S Slow growing S Microscopic similar to : S Scedosporium S Chrysosporium apiospermum B. dermatitidis mycelial form ( lollipop )

Mycelial colony similar to B. dermatitidis S. apiospermum in slide culture Chrysosporium sp. in slide culture
 B. dermatitidis,")
Blastomyces dermatitidis Laboratory diagnosis S Direct examination B. Dermatitidis ( H-E ) B. dermatitidis, GMS

• Microscopy of secretions- The characteristic yeast cell may be seen in a wet preparation of sputum or pus. • Body fluids such as urine or pleural fluid should be centrifuged and the sediment examined. • BAL (Bronchio Alveolar Lavage) may be useful in patients who are not producing sputum. • When organisms are low, they may be more easily identified on papanicolaou (PAP) preparations. • Histology- Gmomori’s methenamine silver and PAS stains readily the fungus.

• Culture- Material should be inoculated onto Sabouraud’s or more-enriched agar and incubated at 300 C. • The mycelial form is not diagnostic, and ideally conversion to yeast at 370 C should be demonstrated. • This is not always possible and mycelial identification can be achieved by nucleic acid probes for Blastomyces RNA. • Serology-Complement fixation, immunodiffusion and ELISA based tests are available but sensitivity and specificity vary widely.

- Slides: 31