PRACTICAL ECG COLLECTION Normal ECG Lead Placement is





 V 3 & v 4(ANTERIOR) V 1 & v 2(SEPTAL) V")























")









- Slides: 48
PRACTICAL ECG COLLECTION
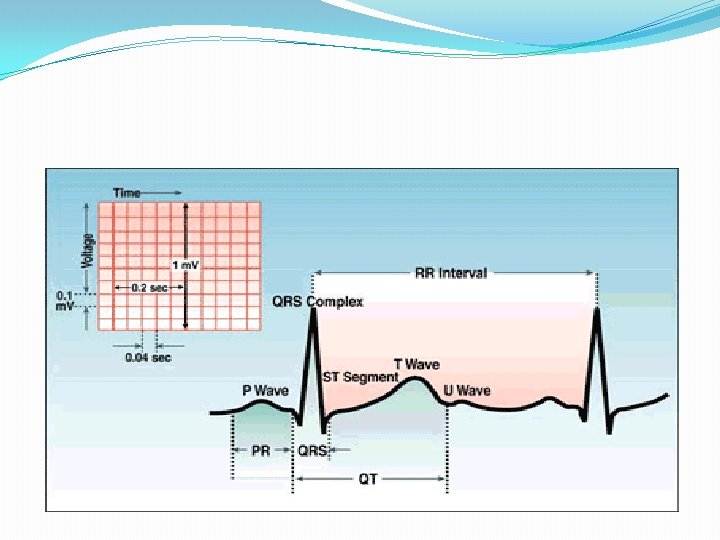
Normal ECG
Lead Placement is Important �Each positive electrode acts as a camera looking at the heart �Ten leads attached for twelve lead diagnostics. The monitor combines 2 leads. �Mnemonic for limb leads � White on right � Smoke(black) over fire(red) � Snow(white) on grass(green) � 2004 Anna Story
Precordial Leads � 2004 Anna Story 4
Rhythm
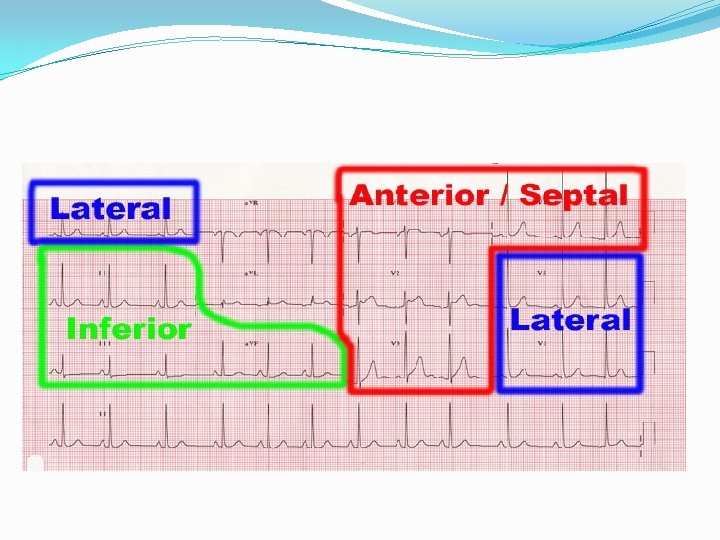
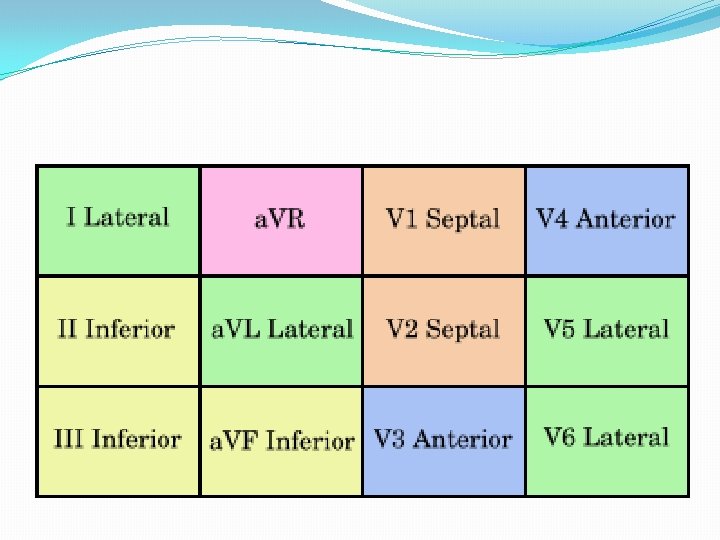
I and AVL(LATERAL) V 3 & v 4(ANTERIOR) V 1 & v 2(SEPTAL) V 5 & v 6(LATERAL) II, III and AVF(INFERIOR) � 2004 Anna Story Where the positive electrode is positioned, determines what part of the heart is seen! 7
angina
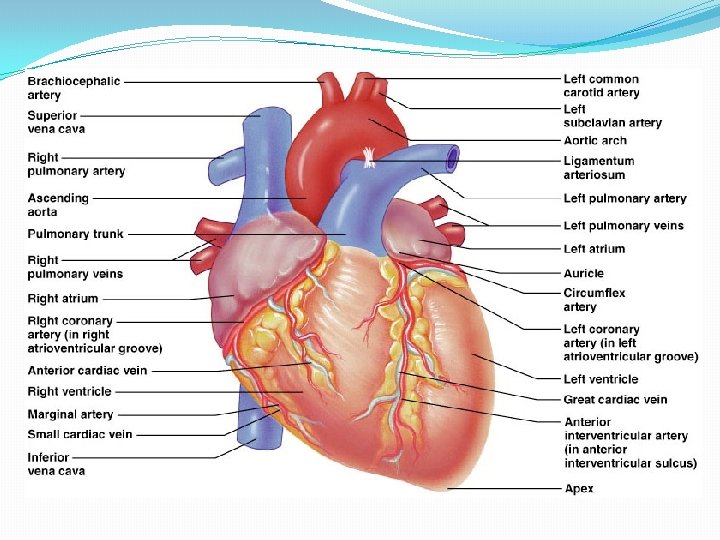
CORONARY CIRCULATION The left coronary artery distributes blood to the left side of the heart, the left atrium and ventricle, and the interventricular septum The circumflex artery arises from the left coronary artery The larger anterior interventricular artery, also known as the left anterior descending artery (LAD), is the second major branch arising from the left coronary artery. The right coronary artery proceeds along the coronary sulcus and distributes blood to the right atrium, portions of both ventricles, and the heart conduction system.
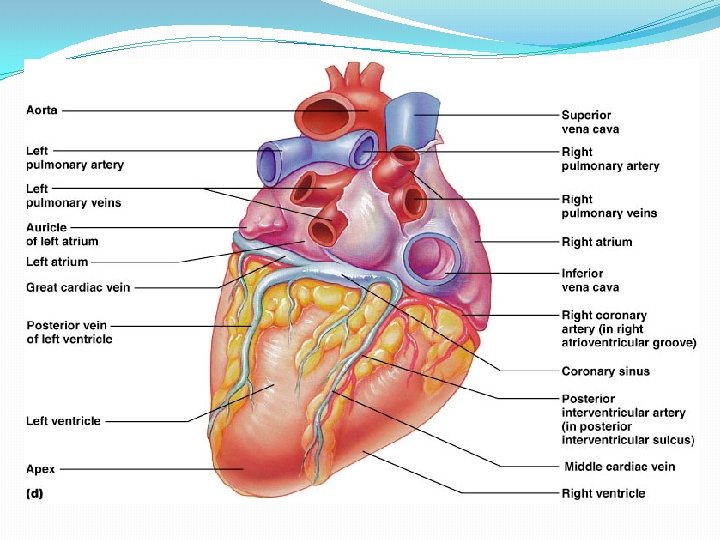
marginal arteries arise from the right coronary artery inferior to the right atrium. marginal arteries supply blood to the superficial portions of the right ventricle On the posterior surface of the heart, the right coronary artery gives rise to the posterior interventricular artery, also known as the posterior descending artery. supply the interventricular septum and portions of both ventricles. [1]
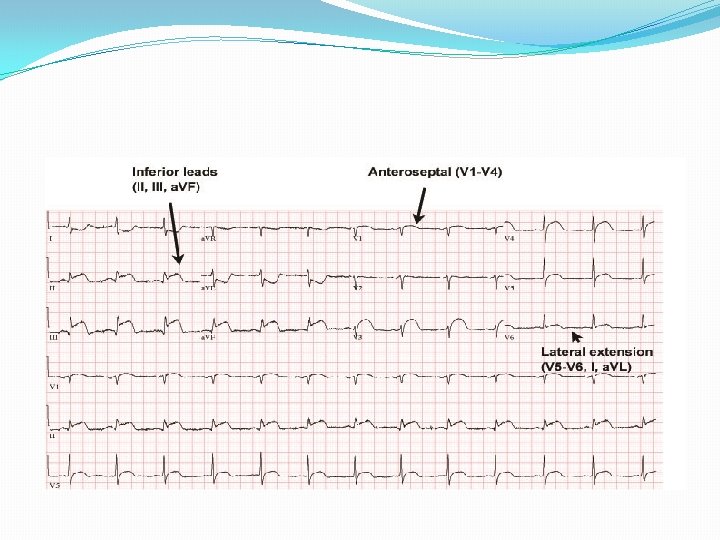
ECG leads Location of MI Coronary Artery II, III, a. VF Inferior MI Right Coronary Artery V 1 -V 4 Anterior or Anteroseptal MI Left Anterior Descending Artery V 5 -V 6, I, a. VL Lateral MI Left Circumflex Artery ST depression in V 1, V 2 Posterior MI Left Circumflex Artery or Right Coronary Artery
acute infero-postero-lateral MI.
Acute Anterior Myocardial
Axis Left or right axis deviation? Look at limb leads I and a. VF. � Normal: I +, a. VF + � LAD: I +, a. VF – � RAD: I -, a. VF +
HEART AXIS Many factors may alter the electrical heart axis including: Anatomic Factors: Abnormal anatomic position of the heart in the thoracic cavity (such as in dextrocardia) Abnormal thoracic anatomy Abnormal position of the diaphragm (such as in obesity, pregnancy, ascites) Cardiopulmonary Pathology: Prior myocardial infarction Recent ischemia Pulmonary embolism Pulmonary obstructive disease Myocardial hypertrophy Dilated cardiomyopathy Conduction abnormalities Others
Left axis deviation
Right axis deviation
Sinus Bradycardia - SB
Sinus Tachycardia - ST
Sinus Arrhythmia - SA
Irregular irregular
Atrial Fibrillation : A Fib
Atrial Flutter : A Flutter
Junctional rhythms
Premature Ventricular Contraction: PVC
Ventricular Tachycardia - VT
Ventricular Fibrillation - VF
Asystole
Artifact:
nd 2 Degree AV Block, Type I (Wenckebach)
2 nd Degree AV Heart Block, Type II
rd 3 Degree Heart Block
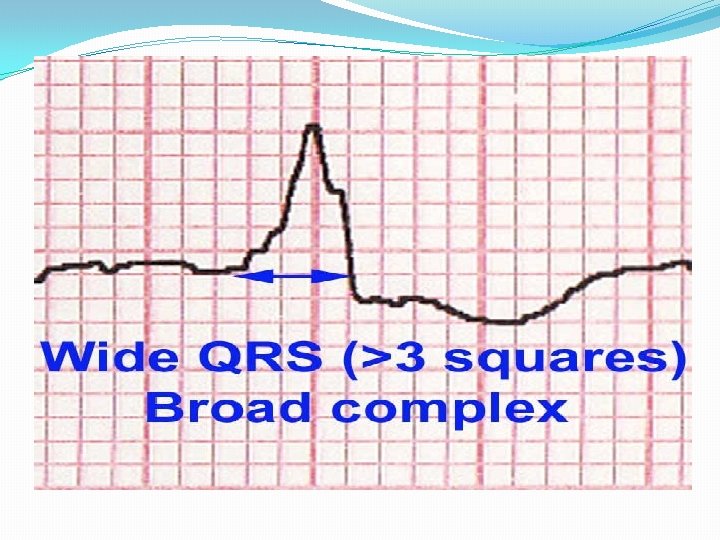
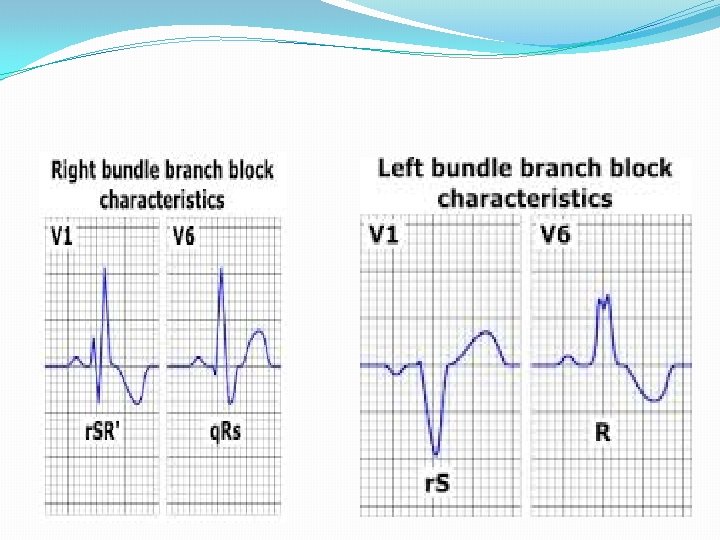
LBBB
cardioversion
automated external defibrillators or AEDs.
X-ray on chest showing pacemaker
Left ventricular hypertrophy (the left ventricle is enlarged and generates more electrical activity, so the heart axis is “pulled” to the left) S in V 1 + R in V 5 or V 6 (whichever is larger) ≥ 35 mm (≥ 7 large squares)
Left ventricular hypertrophy
Left ventricular hypertrophy